Therapy & Theory
Therapy & Theory
ACT
ACTAcceptance & Commitment Therapy (ACT)
Developed within a coherent theoretical and philosophical framework, Acceptance and Commitment Therapy (ACT) is a unique empirically based psychological intervention that uses acceptance and mindfulness strategies, together with commitment and behavior change strategies, to increase psychological flexibility. Psychological flexibility means contacting the present moment fully as a conscious human being, and based on what the situation affords, changing or persisting in behavior in the service of chosen values.
Based on Relational Frame Theory, ACT illuminates the ways that language entangles clients into futile attempts to wage war against their own inner lives. Through metaphor, paradox, and experiential exercises clients learn how to make healthy contact with thoughts, feelings, memories, and physical sensations that have been feared and avoided. Clients gain the skills to recontextualize and accept these private events, develop greater clarity about personal values, and commit to needed behavior change.
How To Start Learning About ACT
There is a vast amount of information available for browsing available on this site. When you have the time, consider browsing through the clinical resources, protocols, measures, books, visual aids, and videos available on the site (under the Resources tab). However, there is so much information available that it can be a little overwhelming.
To get started, we've compiled a comprehensive list of resources for learning more about ACT.
If you are a member of the public, you are welcome to look around the website or join our association to get full access to videos, attachments, publications, etc. You can find publications, find ACT therapists, join the ACT for the Public listserv, and so on.
ACBS members can click here to join our email listservs: ACT for Professionals listserv, RFT listserv, Student listserv, special interest group listservs, and chapter listservs. We have found that participation in these listservs predicts whether you will stay an ACBS member, probably because you can get your questions answered so easily and come to appreciate the importance of being part of a helpful and values-based community.
About ACT
About ACTPsychological Inflexibility: An ACT View of Suffering and Failure to Thrive
The core conception of Acceptance and Commitment Therapy (ACT) or (as it is usual called outside of a therapy context, Acceptance and Commitment Training ... also "ACT") is that psychological suffering and a failure to prosper psychologically is usually caused by the interface between the evolutionarily more recent processes of human language and cognition, and more ancient sources of control of human behavior, particular those based on learning by direct experience. Psychological inflexibility is argued to emerge from six basic processes. Stated in their most general fashion these are emotional inflexibility, cognitive inflexibility, attentional inflexibility, failures in perspective taking, lack of chosen values, and an inability to broaden and build habits of values-based action. Buttressed by an extensive basic research program on an linked theory of language and cognition, Relational Frame Theory (RFT), ACT takes the view that trying to change difficult thoughts and feelings in a subtractive or eliminative way as a means of coping can be counter productive, but new, powerful alternatives are available to deal with psychological events, including acceptance, cognitive defusion, mindful attention to the now, contacting a deeper "noticing" sense of self or "self-as-context", chosen values, and committed action. These six flexibility processes are argued to be inter-related aspects of psychological flexibility. Each of these in turn can be extended socially. For example, acceptance of emotions can extend to compassion for others; chosen values can extend to social values; a "noticing" sense of self to healthy social attachment; and so on.
The ACT Model
ACT is an orientation to behavior change and well-being that is based on functional contextualism as a philosophy of science, and behavioral and evolutionary science principles as expanded by RFT. As such, it is not a specific set of techniques or a specific protocol. ACT methods are designed to establish a workable and positive set of psychological flexibility processes in lieu of negative processes of change that are hypothesized to be involved in behavioral difficulties and psychopathology including
- cognitive fusion -- the domination of stimulus functions based on literal language even when that process is harmful,
- experiential avoidance -- the phenomenon that occurs when a person is unwilling to remain in contact with particular private experiences and takes steps to eliminate the form or diminish the frequency of these events and the contexts that occasion them, even when doing so causes psychological harm
- the domination of a conceptualized self over the "self as context" that emerges from perspective taking and deictic relational frames
- lack of values, confusion of goals with values, and other values problems that can underlie the failure to build broad and flexible repertoires linked to chosen qualities of being and doing
- inability to build larger and larger unit of behavior through commitment to behavior that moves in the direction of chosen values
and other such processes. Technologically, ACT uses both traditional behavior therapy techniques (defined broadly to include everything from cognitive therapy to behavior analysis), as well as others that are more recent "3rd wave" methods, and those that have largely emerged from outside the behavior tradition, such as cognitive defusion, acceptance, mindfulness, values, and commitment methods.
Research Support
Research seems to be showing that these methods are beneficial for a broad range of clients and positive psychological goals as well, not just in mental health areas but also in behavioral health, and social wellness areas. ACT teaches clients and therapists alike how to alter the way psychological experiences function rather than having to eliminate them from occurring at all. This empowering message has been shown to help clients cope with a wide variety of clinical problems, including depression, anxiety, stress, substance abuse, and even psychotic symptoms; to step up to the challenges of diet, sleep, exercise, or the behavioral challenges of physical disease; to help address social problems such as stigma or prejudice; or to seek positive outcomes in areas like relationships, cooperation, business, social justice, climate change, gender bias, and so on. The benefits are as important for the clinician as they are for clients. ACT has been shown empirically to alleviate therapist burnout, for example. By focusing on processes of change what began as a way of dealing with mental health issues is now a model that is used to understand and change human behavior more generally.
How Do You Learn and Apply ACT to Your Practice?
The list of resources below are a great, easy-to-access way to learn more about ACT, it's theoretical and philosophical background. We recommend checking out these pages, as they will provide an important foundation of knowledge. We've also compiled a list of ways to learn about ACT by reading ACT books, as well as getting consultation from others as you begin to apply the work to your work and practice. This additional list of resources will help you do so as well. ACBS members are strongly encouraged to join the ACT for Professionals email listserv. Once on that listserv you can ask virtually any question, or raise virtually any issue, and thousands of ACBS members will read it ... and you can almost be guaranteed of interesting and helpful responses. We've found that members of this listserv are nearly eight times more likely to remain as ACBS members over the years than those who are not on the listserv, and we think the reason is that listserv members come to appreciate the value of being part of a helpful and values-based knowledge development community. If you are not sure, join and lurk for a while. If you do not like it, it easy to step off later on -- you can do so with a single click in your membership dashboard.
Philosophical roots
Philosophical rootsFunctional Contextualism
ACT is rooted in the pragmatic philosophy of functional contextualism, a specific variety of contextualism that has as its goal the prediction and influence of events, with precision, scope and depth. Contextualism views psychological events as ongoing actions of the whole organism interacting in and with historically and situationally defined contexts. These actions are whole events that can only be broken up for pragmatic purposes, not ontologically.
Because goals specify how to apply the pragmatic truth criterion of contextualism, functional contextualism differs from other varieties of contextualism that have other goals. ACT thus shares common philosophical roots with constructivism, narrative psychology, dramaturgy, social constructionism, feminist psychology, Marxist psychology, and other contextualistic approaches, but its unique goals leads to different qualities and different empirical results than these more descriptive forms of contextualism, seeking as they do a personal appreciation of the complexity of the whole rather than prediction and influence per se.
ACT itself reflects its philosophical roots in several ways. ACT emphasizes workability as a truth criterion, and chosen values as the necessary precursor to the assessment of workability because values specify the criteria for the application of workability. Its causal analyses are limited to events that are directly manipulable, and thus it has a consciously contextualistic focus. From such a perspective, thoughts and feelings do not cause other actions, except as regulated by context.
Therefore, it is possible to go beyond attempting to change thoughts or feelings so as to change overt behavior, to changing the context that causally links these psychological domains.
Further information on functional contextualism is available here
Theoretical roots
Theoretical rootsRFT: A Theory of Language and Cognition
ACT is based on Relational Frame Theory (RFT), which is a comprehensive basic experimental research program into human language and cognition. RFT has become one of the most actively researched basic behavior analytic theories of human behavior, with over 70 empirical studies focused on it tenets. In ACT, virtually every component of the technology is connected conceptually to RFT, and several of these connections have been studied empirically.
According to RFT, the core of human language and cognition is the learned and contextually controlled ability to arbitrarily relate events mutually and in combination, and to change the functions of specific events based on their relations to others. For example, very young children will know that a nickel is larger than a dime by physical size, but not until later will the child understand that a nickel is smaller than a dime by social attribution. In addition to being arbitrarily applicable (a nickel is “smaller” than a dime merely by social convention), this more psychologically complex relation is mutual (e.g., if a nickel is smaller than a dime, a dime is bigger than a nickel), combinatorial (e.g., if a penny is smaller than a nickel and a nickel is smaller than a dime then a penny is smaller than a dime), and alters the function of related events (if a nickel has been used to buy candy a dime will now be preferred even if it has never actually been used before).
The applied implications of RFT derived from the following key features:
- Human language and higher cognition is a specific kind of learned behavior. RFT researchers have shown that arbitrarily applicable comparative relations (the nickel and dime situation just mentioned) can be trained as an overarching operant in young children; similar evidence has emerged with frames of opposition and coordination.
- Relational frames alters the effects of other behavioral processes. For example, a person who has been shocked in the presence of B and who learns that B is smaller than C, may show a greater emotional response to C than to B, even though only B was directly paired with shock
- Cognitive relations and cognitive functions are regulated by different contextual features of a situation.
The primary implications of RFT in the area of psychopathology and psychotherapy extend from the three features just described. RFT argues that:
- verbal problem solving and reasoning is based on some of the same cognitive processes that can lead to psychopathology, and thus it is not practically viable to eliminate these processes,
- much as extinction inhibits but does not eliminate learned responding, the common sense idea that cognitive networks can be logically restricted or eliminated is generally not psychologically sound because these networks are the reflection of historical learning processes;
- direct change attempts focused on key nodes in cognitive networks creates a context that tends to elaborate the network in that area and increase the functional importance of these nodes, and
- since the content and the impact of cognitive networks are controlled by distinct contextual features, it is possible to reduce the impact of negative cognitions whether or not they continue to occur in a particular form. Taken together, these four implications mean that it is often neither wise nor necessary to focus primarily on the content of cognitive networks in clinical intervention. Fortunately, the theory suggests that it is quite possible instead to focus on their functions.
RFT has proven itself successful so far in modeling higher cognition in a number of areas, and the neurobiological data collected so far comport with the theory. RFT is meant to be a comprehensive contextualistic account of human language and cognition and thus its goals extend far beyond ACT or even the behavioral and cognitive therapies in general. Because all of the key features of the theory are cast in terms of manipulable contextual variables, it has readily lead to applied interventions in such areas as education.
Theory of Psychopathology
Theory of PsychopathologyCore Problem Processes
From an ACT / RFT point of view, while psychological problems can emerge from the general absence of relational abilities (e.g., in the case of mental retardation), a primary source of psychopathology (as well as a process exacerbating the impact of other sources of psychopathology) is the way that language and cognition interact with direct contingencies to produce an inability to persist or change behavior in the service of long term valued ends. This kind of psychological inflexibility is argued in ACT and RFT to emerge from weak or unhelpful contextual control over language processes themselves, and the model of psychopathology is thus linked point to point to the basic analysis provided by RFT. This yields an accessible and clinically useful middle level theory bound tightly to more abstract basic principles.
A core process that can lead to pathology is cognitive fusion, which refers to the domination of behavior regulatory functions by relational networks, based in particular on the failure to distinguish the process and products of relational responding. In contexts that foster such fusion, human behavior is guided more by relatively inflexible verbal networks than by contacted environmental contingencies. This is fine in some circumstances, but in others it increases psychological inflexibility in an unhealthy way. As a result, people may act in a way that is inconsistent with what the environment affords relevant to chosen values and goals. From an ACT / RFT point of view, the form or content of cognition is not directly troublesome, unless contextual features lead this cognitive content to regulate human action in unhelpful ways.
The functional contexts that tend to have such deleterious effects are largely sustained by the social / verbal community. There are several. A context of literality treats symbols (e.g., the thought, “life is hopeless”) as one would referents (i.e., a truly hopeless life). A context of reason-giving bases action or inaction excessively on the constructed “causes” of one's own behavior, especially when these processes point to non-manipulable “causes” such as conditioned private events. A context of experiential control focuses on the manipulation of emotional and cognitive states as a primary goal and metric of successful living.
Cognitive fusion supports experiential avoidance -- the attempt to alter the form, frequency, or situational sensitivity of private events even when doing so causes behavioral harm. Due to the temporal and comparative relations present in human language, so-called “negative” emotions are verbally predicted, evaluated, and avoided. Experiential avoidance is based on this natural language process – a pattern that is then amplified by the culture into a general focus on “feeling good” and avoiding pain. Unfortunately, attempts to avoid uncomfortable private events tend to increase their functional importance – both because they become more salient and because these control efforts are themselves verbal linked to conceptualized negative outcomes – and thus tend to narrow the range of behaviors that are possible since many behaviors might evoke these feared private events.
The social demand for reason giving and the practical utility of human symbolic behavior draws the person into attempts to understand and explain psychological events even when this is unnecessary. Contact with the present moment decreases as people begin to live “in their heads.” The conceptualized past and future, and the conceptualized self, gain more regulatory power over behavior, further contributing to inflexibility. For example, it can become more important to be right about who is responsible for personal pain, than it is to live more effectively with the history one has; it can be more important to defend a verbal view of oneself (e.g., being a victim; never being angry; being broken; etc) than to engage in more workable forms of behavior that do not fit that that verbalization. Furthermore, since emotions and thoughts are commonly used as reasons for other actions, reason-giving tends to draw the person into even more focus on the world within as the proper source of behavioral regulation, further exacerbating experiential avoidance patterns. Again psychological inflexibility is the result.
In the world of overt behavior, this means that long term desired qualities of life -- values -- take a backseat to more immediate goals of being right, looking good, feeling good, defending a conceptualized self, and so on. People lose contact with what they want in life, beyond relief from psychological pain. Patterns of action emerge and gradually dominate in the person’s repertoire that are detached from long term desired qualities of living. Behavioral repertoires narrow and become less sensitive to the current context as it affords valued actions. Persistence and change in the service of effectiveness is less likely.
Quick & Dirty ACT Analysis of Psychological Problems
Quick & Dirty ACT Analysis of Psychological Problems- Most psychological difficulties have to do with the avoidance and manipulation of private events.
- All psychological avoidance has to do with cognitive fusion and its various effects.
- Conscious control belongs primarily in the area of overt, purposive behavior.
- All verbal persons have the “self” needed as an ally, but some have run from that too.
- Clients are not broken, and in the areas of acceptance and defusion they have the psychological resources they need if they can be harnessed.
- To take a new direction, we must let go of an old one. If a problem is chronic, the client's solutions are probably part of them.
- When you see strange loops, inappropriate verbal rules are involved.
- The value of any action is its workability measured against the client's true values (those he/she would have if it were a free choice). The bottom line issue is living well, not having small sets of “good” feelings.
- Two things are needed to transform the situation: accept and move.
The Six Core Processes of ACT
The Six Core Processes of ACTThe Psychological Flexibility Model
The general goal of ACT is to increase psychological flexibility – the ability to contact the present moment more fully as a conscious human being, and to change or persist in behavior when doing so serves valued ends. Psychological flexibility is established through six core ACT processes. Each of these areas are conceptualized as a positive psychological skill, not merely a method of avoiding psychopathology.
Acceptance
Acceptance is taught as an alternative to experiential avoidance. Acceptance involves the active and aware embrace of those private events occasioned by one’s history without unnecessary attempts to change their frequency or form, especially when doing so would cause psychological harm. For example, anxiety patients are taught to feel anxiety, as a feeling, fully and without defense; pain patients are given methods that encourage them to let go of a struggle with pain, and so on. Acceptance (and defusion) in ACT is not an end in itself. Rather acceptance is fostered as a method of increasing values-based action.
Cognitive Defusion
Cognitive defusion techniques attempt to alter the undesirable functions of thoughts and other private events, rather than trying to alter their form, frequency or situational sensitivity. Said another way, ACT attempts to change the way one interacts with or relates to thoughts by creating contexts in which their unhelpful functions are diminished. There are scores of such techniques that have been developed for a wide variety of clinical presentations. For example, a negative thought could be watched dispassionately, repeated out loud until only its sound remains, or treated as an externally observed event by giving it a shape, size, color, speed, or form. A person could thank their mind for such an interesting thought, label the process of thinking (“I am having the thought that I am no good”), or examine the historical thoughts, feelings, and memories that occur while they experience that thought. Such procedures attempt to reduce the literal quality of the thought, weakening the tendency to treat the thought as what it refers to (“I am no good”) rather than what it is directly experienced to be (e.g., the thought “I am no good”). The result of defusion is usually a decrease in believability of, or attachment to, private events rather than an immediate change in their frequency.
Being Present
ACT promotes ongoing non-judgmental contact with psychological and environmental events as they occur. The goal is to have clients experience the world more directly so that their behavior is more flexible and thus their actions more consistent with the values that they hold. This is accomplished by allowing workability to exert more control over behavior; and by using language more as a tool to note and describe events, not simply to predict and judge them. A sense of self called “self as process” is actively encouraged: the defused, non-judgmental ongoing description of thoughts, feelings, and other private events.
Self as Context
As a result of relational frames such as I versus You, Now versus Then, and Here versus There, human language leads to a sense of self as a locus or perspective, and provides a transcendent, spiritual side to normal verbal humans. This idea was one of the seeds from which both ACT and RFT grew and there is now growing evidence of its importance to language functions such as empathy, theory of mind, sense of self, and the like. In brief the idea is that “I” emerges over large sets of exemplars of perspective-taking relations (what are termed in RFT “deictic relations”), but since this sense of self is a context for verbal knowing, not the content of that knowing, it’s limits cannot be consciously known. Self as context is important in part because from this standpoint, one can be aware of one’s own flow of experiences without attachment to them or an investment in which particular experiences occur: thus defusion and acceptance is fostered. Self as context is fostered in ACT by mindfulness exercises, metaphors, and experiential processes.
Values
Values are chosen qualities of purposive action that can never be obtained as an object but can be instantiated moment by moment. ACT uses a variety of exercises to help a client choose life directions in various domains (e.g. family, career, spirituality) while undermining verbal processes that might lead to choices based on avoidance, social compliance, or fusion (e.g. “I should value X” or “A good person would value Y” or “My mother wants me to value Z”). In ACT, acceptance, defusion, being present, and so on are not ends in themselves; rather they clear the path for a more vital, values consistent life.
Committed Action
Finally, ACT encourages the development of larger and larger patterns of effective action linked to chosen values. In this regard, ACT looks very much like traditional behavior therapy, and almost any behaviorally coherent behavior change method can be fitted into an ACT protocol, including exposure, skills acquisition, shaping methods, goal setting, and the like. Unlike values, which are constantly instantiated but never achieved as an object, concrete goals that are values consistent can be achieved and ACT protocols almost always involve therapy work and homework linked to short, medium, and long-term behavior change goals. Behavior change efforts in turn lead to contact with psychological barriers that are addressed through other ACT processes (acceptance, defusion, and so on).
Taken as a whole, each of these processes supports the other and all target psychological flexibility: the process of contacting the present moment fully as a conscious human being and persisting or changing behavior in the service of chosen values. The six processes can be chunked into two groupings. Mindfulness and acceptance processes involve acceptance, defusion, contact with the present moment, and self as context. Indeed, these four processes provide a workable behavioral definition of mindfulness (see the Fletcher & Hayes, in press in the publications section). Commitment and behavior change processes involve contact with the present moment, self as context, values, and committed action. Contact with the present moment and self as context occur in both groupings because all psychological activity of conscious human beings involves the now as known.
A Definition of ACT
ACT is an approach to psychological intervention defined in terms of certain theoretical processes, not a specific technology. In theoretical and process terms we can define ACT as a psychological intervention based on modern behavioral psychology, including Relational Frame Theory, and evolutionary science, that applies mindfulness and acceptance processes, and commitment and behavior change processes, to the creation of psychological flexibility.
ACT Video Series - Six Core Processes of ACT
ACT Video Series - Six Core Processes of ACTThe Veterans Health Administration, part of the US Department of Veterans Affairs, has a video series about ACT that provides an introduction to the six core processes of ACT.
ACT Therapeutic Posture
ACT Therapeutic Posture- Whatever a client is experiencing is not the enemy. It is the fight against experiencing experiences that is harmful and traumatic.
- You can't rescue clients from the difficulty and challenge of growth.
- Compassionately accept no reasons—the issue is workability not reasonableness.
- If the client is trapped, frustrated, confused, afraid, angry or anxious be glad—this is exactly what needs to be worked on and it is here now. Turn the barrier into the opportunity.
- If you yourself feel trapped, frustrated, confused, afraid, angry or anxious be glad: you are now in the same boat as the client and your work will be humanized by that.
- In the area of acceptance, defusion, self, and values it is more important as a therapist to do as you say than to say what to do
- Don't argue. Don't persuade. The issue is the client's life and the client's experience, not your opinions and beliefs. Belief is not your friend.
- You are in the same boat. Never protect yourself by moving one up.
- The issue is always function, not form or frequency. When in doubt ask yourself or the client “what is this in the service of.”
Readings on this topic
Follette, V. M., & Batten, S. V. (2000). The role of emotion in psychotherapy supervision: A contextual behavioral analysis. Cognitive and Behavioral Practice, 7(3), 306-312.
Pierson, H. & Hayes, S. C. (2007). Using Acceptance and Commitment Therapy to empower the therapeutic relationship. Chapter in P. Gilbert & R. Leahy (Eds.), The Therapeutic Relationship in Cognitive Behavior Therapy (pp. 205-228). London: Routledge.
Wilson, K. G., & Sandoz, E. K. (2008). Mindfulness, values, and the therapeutic relationship in Acceptance and Commitment Therapy. In S. F. Hick & T. Bein (Eds.), Mindfulness and the therapeutic relationship. New York: Guilford Press.
ACT Therapeutic Steps
ACT Therapeutic Steps- Compassionately confront the unworkable agenda, appealing always to the client's experience as the ultimate arbiter
- Support the client in feeling and thinking what they directly feel and think already—as it is not as what it says it is—and to find a place from which that is possible.
- In the service of that goal, teach acceptance and defusion skills.
- Help the client make a richer and less defended contact with the present moment, and with their own on-going thoughts, feelings, and sensations.
- Help the client contact a transcendent sense of self.
- Help the client become more consistently mindful.
- Help the client move in a value direction, with all of their history and automatic reactions.
- Help the client detect traps, fusions, and strange loops.
- Repeat, expand the scope of the work, and repeat again, until the clients generalizes.
- (and don't believe a word you are saying).
Common Misunderstandings About ACT / RFT
Common Misunderstandings About ACT / RFTHere are a number of common misunderstandings about ACT and RFT and CBS. I've listed only ones that I think are demonstrably false. Ones that could be true I have not listed since this page is about misunderstandings, not legitimate weaknesses. Comments follow each. If you know of others, let me know - Steven Hayes
- ACT is just _____ (fill in your favorite: Buddhism, CT, BT, CBT, Logotherapy, a psychology of the will, Gestalt, existential, est, Morita, constructive living, solution focused therapy, Kelly role therapy, and so on and so on)
Resemblance is a fun game to play but I have yet to have anyone say these things in strong form (it is just _____) when they have really delved into the philosophy, theory, data, and technology. It is actually a positive sign when you see that others are pointing to somewhat similar issues. If multiple paths lead in a direction perhaps that is a direction worth exploring. If folks want to draw the connections above, it would be good to do them seriously and in print so people can understand the connections. The only ones I could see myself fully agreeing to is "ACT is just behavior analysis" ... or, properly understood, "ACT is just behavior therapy," but I'd quickly want to add "but that area itself has to be understood in a different way to say that." As far as roots, some of these are indeed influences on ACT. You could find some historical connections with CT, BT, CBT, Logotherapy, Gestalt, existential, and est for example. Maybe Buddhism if you mean "estern thought" -- as a child of the 60's it would be hard to avoid that. Probably a few more and as it expands lots of new things come in. ACT is a vast community now. - ACT is a cult
James Herbert has a great powerpoint on this site walking through why that comparison is unfair and inaccurate. Cults are closed off; they avoid criticism; they are hierarchical; they suppress open expression. ACBS is the exact opposite in all of these areas. - ACT is just the latest fad
ACT will ultimately die, as will we all, and it may indeed do so in a matter of decades or sooner, as what is worthwhile inside it become better understood and enters into the mainstream (that process of assimilation is happening at light speed right in front of our eyes), but if you mean that it is frivolous or insubstantial, that is just factually incorrect. When you last 35 years, do over 1000 basic and applied studies, and train over 50,000 people, "fad" is just not an applicable term. Is it? Inside the ACBS community we suspect that the applied and basic theory underlying ACT and RFT (etc) is wrong but that is because so far in science all theories have ultimately been shown to be incorrect. We just don't know where it is wrong yet ... but we are chasing that rabbit! Come help us prove ourselves wrong! - ACT is new on the scene
It is just under 35 years old. The first ACT workshop was given in 1982 at Broughton Hospital in North Carolina. - ACT is old on the scene and thus its outcome studies should be __ times more
When I first posted this page in the early 2000s I had to explain our slow start, but now the criticism is just so far out of date even that explanation seems unneeded. OK, here is the explanation I used to give: ACT followed a different development path linked to philosophy, basic research, and process measurement. There was a 14 year gap in outcome studies from 1986 to 2000. That gap should not be held against the tradition because the detour was linked to even higher standards and goals. During that time, functional contextualism, the psychological flexibility model, RFT, measures of psychological flexiblity, and a contextual behavioral science approach were created -- and it seemed responsible to do that before larding up with RCTs after the first 3 successful ones in the mid 1980s. ACT is willing to be held to RCT-linked standards but RCTs alone are not enough to create a progressive field. You need a theory and development strategy that works. Once we had that better worked out we did indeed come back to outcome studies. If you look at the outcome studies since 2000 it would be a hard case to make that ACT does not care about outcome data. In 2000 there were 3 RCTs in ACT but it began to pick up in the mid 2000s. When I first rewrote this page as 2011 began it was up to 37 RCTs. Wow. Now it is five years later and I'm rewriting the page again in early 2016. The number of RCTs is hard to say precisely because a new one appears every week or less and no one can keep up anymore and still have a life. My best guess is that it is sliding past 200 (I have 153 in a file but a new paper my students wrote for a class tells me that there are about 70 more studies I missed that are not in English). And meanwhile ACT has more and more consistent mediation outcomes than any approach in existence. Our guess is over 50 studies. And it is the ONLY psychotherapy with a vigorous basic science of cognition underneath it, with hundreds of studies on RFT. An entire book has been written on the ACT Research Journey (Hooper & Andersson, 2015: http://www.amazon.com/Research-Journey-Acceptance-Commitment-Therapy/dp/1137440163/ref=sr_1_1?s=books&ie=UTF8&qid=1459110186&sr=1-1&keywords=ACT+research+journey). So, really, anyone suggesting we are slack in terms of research just does not know what he or she is talking about. Counting all areas of CBS my best guess based on search engines is that there are over 2000 studies if you apply a liberal set of search criteria and about 1000 if you apply a strict set. - ACT seeks ridiculously high goals and thus is making grandiose predictions or claims. Aspirations are not predictions or claims. Seeking a comprehensive account of behavior that would apply to all human action has always been the goal of behavior analysis as is shown in things such as Walden II. Why is a grand aspiration grandiose?
- ACT works only with the well-educated
There are many trials indicating ACT is helpful for those who are poor, uneducated, intellectually disabled, children, those diagnosed with psychotic disorders, and so on and on. This criticism comes because the theory can be hard to understand (especially RFT). But we do not teach theory to client, we do therapy. That is different. - ACT works only for white middle class Americans
There are ACT studies from 15 countries includinging countries in Asia, the Middle East, and Africa. Successful studies have been done with poor urban black populations; unemployed poor Asian American populations; institutionalized South African blacks, etc. As of early 2016 there are 45 RCTs done on ACT in Iran; over 30 RCTs in Korea. The outcomes are equally good. The criticism is simply invalid. - ACT is not committed to science
Come on; wake up. Put in key ACT and RFT terms into the Web of Science or Google Scholar and look at what is out there dude. Download the studies. It after you do all that you repeat this claim that within arm's reach of me or you'd better be able to duck fast. - The ACT research base is weak
ACT has drawn a lot of interest from funded researchers and ACT funded studies are as good as any out there. There are a lot of them too (perhaps 50 RCTs of that kind) and the outcomes are often (not always) impressive. Yes, in some areas the research base is lean -- but ACT is not just for one problem area. In some areas, such as smoking or chronic pain, you'd have to distort the meaning of evidence to say that they ACT research base is weak. And these are areas where people have worked for years to dial in how to move ACT processes. So overall the research base seems impressive given the scope of ACT work. Having said that, we need to add three things. First, ACT draws a lot of interest from students, the developing world, or parts of the developed world without a grant infrastructure. These studies often have methodological issues (sample size; controls; etc) but jeez, how do they DECREASE what we know if they ADD to what we know from the best studies? Can someone please explain that to me? It happens IMHO only if people doing meta-analyses average methodology ratings. I'm sorry, that is just a dumb idea. Sure, weight findings study by study in light of methodological issues. But if a person in Liberia shows that ACT is helpful for problem x, and a huge grant-based study at a Western academic medical center with all of the bell and whistles showed that ACT is helpful for that same problem, the one in Liberia added to what we know regardless of its weaknesses. It showed that these approaches to not just apply to the western world, for one thing. It is fine to use the well controlled one to estimate effect sizes. But don't average the methodology ratings from the two and then say that the overall knowledge is weak in problem area x because the average methdology score is humble. Aaaagh. That is just stupid. Second, you need a string of studies in a given area with a given population to learn how to move psychological flexibility processes. If the technology has weak outcomes but did not move the processes, that is an unfortunate technology error, not a model failure. If you move the processes and the outcomes are poor that is a model failure. Yes, there are technology failures in ACT, but usually with new populations, settings, or modes of delivery. I know of no replicated model failures in 35 years of ACT / RFT / CBS research. Finally, some meta-analyses are biased. They are. Look at the overall pattern of meta-analyses and look carefully for responses to meta-analyses. For example, Ost claimed in 2008 that 13 ACT RCTs were weaker than 13 matched CBT RCTs; but then Gaudiano showed that effect was 100% due to grant funding, and furthermore 12 of the 13 ACT studies published mediational outcomes while 1 of the 13 CBT studies did so. An objective reader should reject Ost's comparison. You have to look at the criteria too. For example, if you rightly put "well defined population" on a list of methodological criteria, and then in small print insist on a DSM diagnosis as the only metric for a "well defined population," ACT will look methodologically weaker due to intellectually defensible choices that the reader might not realize is at play. CBS researchers generally despise the DSM. Including such a scoring approach behind an item will lead to a biased "criterion" (one that even NIMH has abandoned!). But the reader has to dig deep to sniff out bias liek that when it is there -- and sometimes not matter how much care, the reader will be bamboozled (e.g., if the ratings themselves have horrible kappas that are not reported). But the ACT community does not lay back on such things. We keep asking for the information and we keep trying to understand findings. As a reader: Keep your powder dry; be careful before leaping; look at the entire set of criticisms, responses, and meta-analyses; use your best judgment. - ACT is just a technology
It is a far more ... do your reading. It is a model linked to a philosophy, basic science, and a strategy of development. - ACT is just a philosophy
Ditto. - ACT is just acceptance
Ditto. - ACT is just commitment
Ditto. - ACT is just acceptance and commitment
Aw, come on. This kind of thing comes from folks reading the titles of books and studies instead of books and studies. - Acceptance is important because it is a way to change the content of emotion (so ACT is really about that)
The data suggest otherwise. Emotion do often change, but that change predicts behavioral outcomes more poorly than changes in the functions of emotions -- and sometimes good outcomes come without a change in emotion within the extant ACT literature. - Defusion is important because it is a way to change the content of thought (so ACT is really about that)
Double ditto. Same point. Also decent data supporting it. Will thoughts change? Sure! RFT is all about changing thoughts and of course ACT changes thoughts. - The ACT model of cognition is no different than any CBT model -- it is just different in its terminology
If you believe that, have the courage to do your homework in detail and write it up in article form. Then be prepared to have others go after your ideas. We have so far responded to every single serious criticism in print in ACT or RFT, so anyone can read the criticisms and the response and judge the arguments. So far no one, I mean no one, has made the claim above in a careful scholarly article. But it is not the ACT world's obligation to prevent the claim from being made in the hallways of convention hotels or on listserves. Even here we do what we can, however. You are reading exhibit A in that area. - Defusion is just distancing as that concept is used in CT
They are indeed related. That is one of the real historical sources of ACT. But in ACT there are scores of such techniques, the are emphasized a great deal, and they are put to a quite different purpose than in traditional CT. - ACT is just mindfulness as that concept is used by Buddhists or ______ (fill in the blank)
ACT is clearly broader at the level of theory and technology. Mindfulness is itself a broad term that ican be vague if it is left at that level. That is why we have written 4-5 articles walking through the concept of mindfulness and trying to come up with a tighter analysis of it. When defined in the right way, ACT is a mindfulness-based approach but it is more than that as well. - Defusion is just exposure in a traditional sense
Research shows that defusion supports exposure. If you say it is exposure then you have expanded exposure to conver most contact of human beings with events and that is troublesome. Besides exposure itself is not well understood, and ACT folks have a flexibility and pattern-based account of exposure that comports with the ACT model. - Acceptance is just exposure in a traditional sense
Research shows that it supports exposure and appears to empower the impact of exposure. ACT is an exposure-based technology and we said in the first chapter on ACT in 1987. But the ACT view of exposure is that it is organized contact with previously repertorie narrowing events for the purpose of creating response flexibility. That is why our goal is teaching more flexible contact with private events and more flexible patterns of responding. We want patients to be able to label emotions; to feel them openly; and to be able to approach their values in action. The most recent work in traditional exposure in CBT is finally catching up that approach. We do not do exposure to reduce emotions (thought they usually are reduced) -- but it turns out that is not why exposure works even in traditional CBT. - ACT does not care about the relationship
We have a model of it; we teach it; we emphasize it. We have data showing that ACT gets high aliance scores; they predict outcome; but they are themselves explained in part by changes in acceptance/defusion/valued action. So no only do we care about the relationship, we care enough to be able to teach clinicans how to create powerful ones: create a psychologically flexibile relationship. - ACT eschews meditation and contemplative practice
Contemplative practice is often in our protocols (about 40% of the RCTs); Guided meditations is in nearly 100% of the protocols; ACT targets mindfulness at the level of process in multiple ways; it moves and is mediated by these processes; psychological flexibility impacts the brain or telomere length (etc) similarly. Now if you insist that mindfulness = sitting and following the breath, yes ACT is mostly not that. But if you insist on that narrow definition you now have to go to war with ancient mindfulness traditions too. Is a koan about mindfulness? Is chanting? This is why I resisted the word "mindfulness" in early ACT writing. I did not want to enter into arguments that were thousands of years old. ACT cares about mindfulness as a process. - You should not mix behavioral procedures with ACT
The model says you should. ACT is part of behavior therapy. With all due respect, you don't get to peel it away from its model just because that makes you uncomfortable in your sorting of things into cubby holes. - If you do mix behavioral procedures with ACT you now have a combined treatment
ACT is a model. Since the model says you should do this, it does not become a combination treatment to follow the model. In early ACT work we often deliberately hobbled the model so we could be heard by others (e.g., taking out formal exposure in studies on OCD). Times up. After 200 RCTs, no more hobbling the model to avoid science critics and their cubby holes. - The other aspects of ACT add nothing to the behavioral elements
We know that these other elements are helpful and that they can support the behavioral elements. If you mean that the other elements are inert, that is clearly untrue. We published a meta-analysis of the first 60 or so component studies and all of the components matter [Levin, M. E., Hildebrandt, M. J., Lillis, J., & Hayes, S. C. (2012). The impact of treatment components suggested by the psychological flexibility model: A meta-analysis of laboratory-based component studies. Behavior Therapy, 43, 741–756. DOI: 10.1016/j.beth.2012.05.003.] More formal component analysese are beginning to appear [Villatte, J. L., Vilardaga, R., Villatte, M., Vilardaga, J. C. P., Atkins, D. A., & Hayes, S. C. (2016). Acceptance and Commitment Therapy modules: Differential impact on treatment processes and outcomes. Behaviour Research & Therapy, 77, 52-61. doi:10.1016/j.brat.2015.12.001]. And we know that all of the aspects of the psychological flexibility model contribute to outcomes (McCracken and colleagues have a study on that in the chronic pain area). - The data on traditional CBT is far stronger
Well, duh. Your father's retirement account is bigger than yours too. ACT is part of the CBT / BT / BA family but its specific research program takes a large community to mount. The CBS community is focused on basic science, processes of change, micro-studies, prevention, social change, link to evolution science, and so on and on. But dig deeper. The vast majority of what is specifically supported in traditional CBT is stuff that ACT folks agree with anyway. If you insist on drag race studies --OK. Be patient. But you can't start outcomes studies in 2000 and expect 16 years later to have the same amount of data as the biggest dog on the block. But our research productivity is now obvious for anyone to see. If you know how to de searches - It is surely safe to mix ACT techniques with other techniques I'm more comfortable with while I wait passively to understand the model
Ah, no. Down that path lies chaos. It is such a poor model of scientific development. Understand first. Get the data. Then add anything that makes sense for good theoretical and practical reasons, not just because you feel like it. One great benefit we have in ACT: if the thinks you like to do already improve psychological flexibility (measure it regularly) than by all means include those things. - When I do that I should be able to rename it and get famous tomorrow because what I added (here you can pick any of the other misunderstandings -- relationship, emotion, mindfulness, etc etc) is obviously missing from the model
You can rename it and still come and talk at our conventions etc. We don't care about names. Some folks in the CBS community call ACT "Acceptance Based Behavior Therapy" for example. It turns out that psychological flexibility still mediates the outcomes. But branding helps people find the work so at least rename it for a good reason (e.g., sometimes it make it hard to do meta-analysises). It's up to you. - You can mix ACT with the cognitive elements of CT / CBT easily
With some, but be careful. Incoherence is not usually helpful and patients will detect the incoherence if it is there. - It is safe to do research on ACT without doing any training in ACT
Is it safe to do surgery that way? You cannot read a book and do this well. Get some training. It is cheap and available and non-proprietary. ACT folks will collaborate and consult. Reach out. - It is safe to criticize ACT based on what you've heard about it from others who are not expert in it
What is it about reading carefully that is so aversive? - ACT contains nothing new
If you've studied it thoroughly, just say it in print and say why you say that and let us all look at it dispassionately. If you've not done your homework yet, see above. - ACT is behavioral in an S-R sense
ACT is actively hostile to S-R psychology. - ACT is behavioral in a traditional behavior analytic sense
ACT / RFT is part of behavior analysis, but RFT changes everything. ACT is part of post-Skinnerian behavior analysis -- which is a new form. We call it "contextual behavioral science." Read the RFT book for why we say that. - For these reasons ACT is not oriented toward cognition
200 studies on cognition later, how can folks still say that?! Come to a training at least. - For these reasons ACT is not oriented toward emotion
Come to a training! Watch some tapes! Go look at my TEDx talk: www.bit.ly/StevesFirstTED - Because ACT is broadly applicable it is primarily based on a non-specific clinical process
The theory says why it is broadly applicable and the process data so far say it is successful due to specific process changes. We now have socres of mediational analyses out or in press. - Anything that works for such a broad range of problems must be bulls**t
The theory says why it is broadly applicable. Who are you to say a priori what nature is like? - There are not many outcome studies on ACT
About 200 RCTs and scores more controlled time series designs and counting. - ACT / RFT is a small minority
Maybe. But there are about 3000 folks on the ACT / RFT listservs and over 8000 in the association. ACBS is bigger than ABCT or ABAI. Its one of the the fastest growing associations of its kind out there. Besides, minority or not, we are speaking of ideas and data, not politics. - ACT proponents make excessive claims that go beyond the data
A quote would be nice. - ACT is hierarchical and you have to pledge allegiance to a leader to be involved with it
It's an open list serve; an open website; no certification of therapists; no cut goes to originators from members/trainers/etc; you can get our protocols for free; anyone can become a trainer. There are more ACT books by others than by the originators, by far. This is just so unfair. Its a cartoon, and an ignorant one at that. - ACT processes have not been studied
Download the list of studies and read them. We think our process data are stronger than just about any other approach in all of applied psychology, and our link to basic science is excellent. - RFT can't explain anything other models of cognition cannot explain
RFT researchers have explained phenomena that other approaches have had hard times with. For example, we are learning how to establish a sense of self, we know a lot about how metaphor works, we know a core process in human cognition. And it appears that RFT programs raise IQs more dramatically than anything else out there; it helps with acquisition of language in disabled children; it has better implicit measures than anyone; it can predict who will succeed for fail clinically; etc. - RFT is just jargon
How much have you carefully read so far? Until you read carefully you cannot distinguish jargon and a technical language. RFT has a techical language, but only when technical terms are needed. If you disagree, pick a technical term and show how it is the same as a common sense one. Maybe there was a slip. - ACT is just jargon
Same reaction as above. - No one can understand RFT
Do the RFT tutorial on this website. Yes the basic studies are damn hard to understand ... you are languaging about language and that is just confusing. But it is not beyond anyone reading this website. Physics is hard too -- so? - No one can understand ACT
You can. And "understanding" in a purely intellectual sense is not the point for clients anyway. Usually what therapists mean when they say this is that they are afraid that if they don't understand it thoroughly they can't do it effectively. Folks like Raimo Lappalainen have shown that ACT works even when delivered by beginning therapists who don't really understand it. In fact most of the outcome data on ACT was not done with experienced ACT therapists. It's a miracle these studies work at all -- but they do. Understanding does help: we have studies - RFT has little to do with ACT
ACT and RFT co-evolved. There are many, many links are there and in both directions. It is not a matter of point to point correspondence and it should not be if we are right and applied and basic science should relate in a reticulated way. - ACT folks don't want CT people to be involved and they look down on them
Ask some CT people who got involved in ACT work what they think about how they were treated. Just ask. - We don't know which components work because there are no dismantling studies
ACT comes from an inductive tradition. Rather than wait decades for dismantling studies we've done over 60 technique building and micro-analytic studies (see the reference above) and every aspect of the model has at least some targetted research data. And we do have some studies that dismantle the methods to a degree (an example was listed above) - I hate the enthusiasm of students who do these workshops -- it scares me
We can all agree that enthusiasm is not the same as substance ... but suppose that enthusiasm is hostile to substance? Besides this concern itself sounds emotional so why let emotions substitute for data just because it is now your emotions we are talking about (it scares me) ? Be consistent. If enthusism creeps you out, try to make room for being creeped out, hang on to your legitimate skepticism, and follow the data. - I just don't like ACT
See above. - Talk of spirituality in ACT is creepy
It is treated as a naturalistic concept. ACT is not a religion. - I don't want to be told my values
ACT folks will never do that ... your values are your choice. - There is no data on ACT in groups
About a third of the RCTs on ACT are done in groups, so that means scores of studies. - ACT works through the same process as ____ (fill in your favorite)
Show me the actual research please. The reverse is much more likely to be true so far (the psychological flexibility model explains your favorite). But that is cool, no? Now that we know how things work we can chase the outcomes together. - ACT is not self-critical
Lurk on the list serve and see. Come to a WorldCon and see. - Steve Hayes is a jerk -- I saw him do a mean joke or a mean comment at ABCT or ABAI
ACT is not Steve Hayes -- there are scores of leaders in ACT / RFT. Besides, distinguish the message from the messenger. Some of us are confrontational about intellectual issues, but we don't go after people or traditions: just ideas. The list serve NEVER has flame wars, and that includes toward others. We are just playing hard. Why not? It is fun and can be helpful. Not everyone inside CBS plays the same way. if you hate folks who like to argue, go to ACT talks (etc) by softer folks. As for mean humor, sometimes roast humor can slip across the line a bit, but we tease those we respect. In the ACT community we use humor to remind us all that this work is not about the muckity mucks (including those inside ACBS) ... it is a shared enterprise and everyone is part of it who wants to be part and is willing to bring science based values and caring to the table. If you come to an ACBS conference you will see that the ACT / RFT leadership is outright ridiculed in the "follies" and it is just great fun. Anyone has access to the stage. Even cognitive therapists! : ) - ACT is crazy (or my personal favorite variant since I'm writing this, Steve is crazy)
Ah, finally you are getting somewhere. But as that Time guy said in 2006 in the last line of the story on me and on ACT -- we may just be crazy enough to pull it off. If you are nutty enough to want to help us, come help us succeed!
Criticisms of ACT
Criticisms of ACTGiven the values of ACBS, there has been efforts from the beginning of the ACBS community to encourage responsible criticism, to give thoughtful critics a stage to speak to the group, of trying to respond thoughtfully in writing to knowledgeable critics, and of trying to resolve issues empirically where possible. Criticisms of ACT have appeared in published forms. The written criticisms of RFT (and to a lesser degree, functional contextualism) are extensive and in writing, as are the defenses. They can be found in the other sections of the website.
Self-Criticism
Part of the core of the ACT / RFT tradition is the openness to criticism, including self-criticism. At the LaSalle ACT Summer Institute (Philadelphia, 2005) James Herbert gave a really solid paper walking through many of the criticisms he knew about, under the title "Is ACT a fad?" He considers not just whether the criticisms are correct, but what those in the ACT / RFT community should do about them. You can look at that talk by clicking on the link below.
- Criticisms of ACT, ACT Summer Institute II (July 2005, PowerPoint file)
Published Criticisms and Responses: An Ongoing Conversation Below is a list of papers that have been published criticizing ACT as well as replies that have been published when available. If you know of other criticisms or replies please email us or add a child page to this page.
- Corrigan, P. (2001). Getting ahead of the data: A threat to some behavior therapies. The Behavior Therapist, 24(9), 189-193.
This was the first strong criticism of ACT published. Corrigan argued that the ratio of non-empirical to empirical articles could be used to argue that third-wave CBT was ahead of its data.
A reply: Hayes, S. C. (2002). On being visited by the vita police: A reply to Corrigan. The Behavior Therapist, 25, 134-137.
The reply argued that the ratio of non-empirical to empirical articles could not be meaningfully used as a measure of getting ahead of data since there were many good reasons to write theoretical discussion pieces. Instead, actual claims that got ahead of the data had to be identified and none have been. Pat has been helpful to ACT researchers in various capacities over the years since that article.
- Corrigan, P. (2002). The data is still the thing: A reply to Gaynor and Hayes. The Behavior Therapist, 25, 140.
- Asmundson, G. J. G., & Hadjistavropolous, H.D. (2006). Acceptance and Commitment Therapy in the Rehabilitation of a Girl With Chronic Idiopathic Pain: Are We Breaking New Ground? Cognitive and Behavioral Practice, 13, 178–181.
- Hofmann, S. G., & Asmundson, G. J. G. (2008). Acceptance and mindfulness-based therapy: New wave or old hat? Clinical Psychology Review, 28, 1-16.
- Hofmann, S. G. (2008). Acceptance and Commitment Therapy: New Wave or Morita Therapy? Clinical Psychology, Science and Practice, 5, 280-285.
The theme of these two articles is that ACT and other mindfulness-based treatments is the same as CBT, and that ACT is the same as Morita Therapy. After these articles were written Stefan Hofmann was invited and funded to speak to the ACBS community in Chicago (2007). We had a great time in respectful dialogue. Read more about this criticism in non-peer-reviewed settings and the ensuing dialogue, click on the child page"ACT is Outright Taken from Morita Therapy" below.
- Öst, L. (2008). Efficacy of the third wave of behavioral therapies: A systematic review and meta-analysis. Behaviour Research and Therapy, 46(3), 296-321.
This article is in part based on proactive efforts by the ACBS community to encourage knowledgeable criticism. Lars-Goran Öst has been invited and funded to come to several ACT conferences beginning even before he was knowledgeable of ACT work, given that he was asked to play the role of an outside critic at the first World Conference in Linkoping, Sweden (2003). He was later also invited to London (2006), and Enschede, The Netherlands (2009), that last invitation coming after the article itself was available.
The theme of Lar-Goran's criticisms have been that ACT research has methodological weaknesses, and that it is not as well done as mainstream CBT research. The latter was based on a comparison of ACT studies with a matched set of traditional CBT studies. His conclusion is that ACT is not an evidence-based treatment.
Gaudiano reply: Gaudiano, B. A. (2009). Öst's (2008) methodological comparison of clinical trials of acceptance and commitment therapy versus cognitive behavior therapy: Matching apples with oranges? Behaviour Research and Therapy, 47, 1066-1070.
Öst reply: Öst, L. -G. (2009). Inventing the wheel once more or learning from the history of psychotherapy research methodology: Reply to Gaudiano's comments on Öst's (2008) review. Behaviour Research and Therapy, 47, 1071-1073.
Gaudiano rejoinder: Gaudiano, B. (2009b) Reinventing the Wheel Versus Avoiding Past Mistakes when Evaluating Psychotherapy Outcome Research: Rejoinder to Öst (2009). Brandon has replied again in a piece self-published online (in an attempt to keep the conversation flowing without the confines of the lengthy peer-review process).
The theme of the replies was that errors were made in Lar-Goran's matching and coding process, resulting in a distorted comparison, and that ACT studies are not weaker when resulting differences in population and funding are weeded out. Further, it is noted that ACT is already listed by APA as an evidence-based treatment. Lars-Goran admits that the two sets of studies are not matched in areas such as funding, and that APA lists ACT as evidence-based, but holds to his original views.
- Arch, J. J., & Craske, M. G. (2008). Acceptance and commitment therapy and cognitive behavioral therapy for anxiety disorders: Different treatments, similar mechanisms? Clinical Psychology: Science & Practice, 5, 263-279.
A reply: Hayes, S. C. (2008). Climbing our hills: A beginning conversation on the comparison of ACT and traditional CBT. Clinical Psychology: Science and Practice, 5, 286-295.
The theme of the response was that ACT is part of the CBT tradition, but it is not possible to compare intellectual similarities until CBT says what it is. Efforts of the authors to do so were argued to change long standing mainstream views, which explain some of why the two could be argued to be very similar. Both the critical article and response agreed that there were good empirical issues to be explored.
Reflective of the tone of this dialogue, several ACT researchers (Georg Eifert, John Forsyth, Steve Hayes, Mike Twohig) are doing work with Michelle Craske and her colleagues trying to study the issues raised. Michelle has been invited to speak at an ACBS World Conference. She was not able to come in 2009 but we hope to hear her in the future.
- Powers, M.B., Vörding, M.B., & Emmelkamp, P. (2009). Acceptance and commitment therapy: A meta-analytic review. Psychotherapy and Psychosomatics, 8, 73-80.
A reply: Levin, M., & Hayes, S.C. (2009). Is Acceptance and commitment therapy superior to established treatment comparisons? Psychotherapy & Psychosomatics, 78, 380.
Author response: Powers, M. B., & Emmelkamp, P. M. G. (2009). Response to ‘Is acceptance and commitment therapy superior to established treatment comparisons?’ Psychotherapy & Psychosomatics, 78, 380–381.
ACT researchers have critically examined the method of the meta-analysis and have published a response to the study, with a revised analysis. A counter response by Powers and colleagues is also available. We invited Paul Emmelkamp to come to Enschede but he could not ... we hope to get him to an ACBS conference in the future.
Replies to Critiques in General: Articles Describing the CBS Strategy Extensive reviews of the issued raised in this article are out or in press, but they are too extensive to simply call them "replies." The theme of the articles (which you can read by clicking the link above) has been to describe the ACT approach, its knowledge development strategy and to show its distinctive features.
Criticism: "ACT is Outright Taken from Morita Therapy"
Criticism: "ACT is Outright Taken from Morita Therapy"Getting Beyond the Way of the Guru and Other Scientific Deadends
Getting Beyond the Way of the Guru and Other Scientific DeadendsBooks
BooksThere are many books, audiobooks, and other materials to help you learn more about ACT, RFT, Contextual Behavioral Science, and related topics such as mindfulness and other third wave interventions.
There may seem like a lot of choices in some areas. And there are, which is a testament to how quickly the ACT/RFT/CBS work has grown.
ACT Books: General Purpose
ACT Books: General Purpose(The following list of books is from the LEARNING ACT RESOURCE GUIDE: The complete guide to resources for learning Acceptance & Commitment Therapy by Jason Luoma, Ph.D. Updated July 2020 learningact.com)
BOOKS FOR LEARNING ACT
- LEARNING ACT
- Acceptance and Commitment Therapy (Theories of Psychotherapy)
- Acceptance and Commitment Therapy, Second Edition: The Process and Practice of Mindful Change
- Acceptance and Commitment Therapy: 100 Key Points and Techniques
- Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change
- Acceptance and Commitment Therapy: Contemporary Theory Research and Practice
- Acceptance and commitment Therapy: The CBT distinctive features series
- Acceptance and Commitment Therapy For Dummies
- The ACT Approach: A Comprehensive Guide for Acceptance and Commitment Therapy
- The Act in Context: The Canonical Papers of Steven C. Hayes
- ACT in Practice: Case Conceptualization in Acceptance and Commitment Therapy
- ACT in Steps: A Transdiagnostic Manual for Learning Acceptance and Commitment Therapy
- ACT Made Simple: An Easy-To-Read Primer on Acceptance and Commitment Therapy (The New Harbinger Made Simple Series)
- The ACT Matrix: A New Approach to Building Psychological Flexibility Across Settings and Populations
- The ACT Practitioner’s Guide to the Science of Compassion: Tools for Fostering Psychological Flexibility
- ACT Questions and Answers: A Practitioner’s Guide to 150 Common Sticking Points in Acceptance and Commitment Therapy
- The Art and Science of Valuing in Psychotherapy: Helping Clients Discover, Explore, and Commit to Valued Action Using Acceptance and Commitment Therapy
- The Big Book of ACT Metaphors: A Practitioner’s Guide to Experiential Exercises and Metaphors in Acceptance and Commitment Therapy
- Interventions for Radical Change: Principles and Practice of Focused Acceptance and Commitment Therapy
- A CBT Practitioner’s Guide to ACT: How to Bridge the Gap Between Cognitive Behavioral Therapy and Acceptance and Commitment Therapy
- Committed Action in Practice: A Clinician’s Guide to Assessing, Planning, and Supporting Change in Your Client (The Context Press Mastering ACT Series)
- A Contextual Behavioral Guide to the Self: Theory and Practice
- Contextual Schema Therapy: An Integrative Approach to Personality Disorders, Emotional Dysregulation, and Interpersonal Functioning
- The Essential Guide to the ACT Matrix: A Step-by-Step Approach to Using the ACT Matrix Model in Clinical Practice Essentials of Acceptance and Commitment Therapy
- Evolution and Contextual Behavioral Science: An Integrated Framework for Understanding, Predicting, and Influencing Human Behavior
- Experiencing ACT from the Inside Out: A Self-Practice/Self-Reflection Workbook for Therapists (Self-Practice/Self-Reflection Guides for Psychotherapists)
- The Heart of ACT: Developing a Flexible, Process-Based, and Client-Centered Practice Using Acceptance and Commitment Therapy
- Innovations in Acceptance and Commitment Therapy: Clinical Advancements and Applications in ACT
- Inside This Moment: A Clinician’s Guide to Promoting Radical Change Using Acceptance and Commitment Therapy
- Introduction to ACT: Learning and Applying the Core Principles and Techniques of Acceptance and Commitment Therapy
- Learning Acceptance and Commitment Therapy: The Essential Guide to the Process and Practice of Mindful Psychiatry
- Learning ACT for Group Treatment: An Acceptance and Com-mitment Therapy Skills Training Manual for Therapists
- A Liberated Mind: How to Pivot Toward What Matters
- The Little ACT Workbook
- Metaphor in Practice: A Professional’s Guide to Using the Science of Language in Psychotherapy
- Mindfulness, Acceptance, and the Psychodynamic Evolution: Bringing Values into Treatment Planning and Enhancing Psychodynamic Work with Buddhist Psychology (The Context Press Mindfulness and Acceptance Practica Series)
- Mindfulness, Acceptance, and Positive Psychology: The Seven Foundations of Well-Being (The Context Press Mindfulness and Acceptance Practica Series)
- Mindfulness- and Acceptance-Based Behavioral Therapies in Practice (Guides to Individualized Evidence-Based Treatment)
- Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition
- Mindfulness and Acceptance in Social Work: Evidence-Based Interventions and Emerging Applications (The Context Press Mindfulness and Acceptance Practica Series)
- The Mindfulness-Informed Educator: Building Acceptance and Psychological Flexibility in Higher Education
- A Practical Guide to Acceptance and Commitment Therapy
- Talking ACT: Notes and Conversations on Acceptance and Commitment Therapy
- Values in Therapy: A Clinician’s Guide to Helping Clients Explore Values, Increase Psychological Flexibility, and Live a More Meaningful Life
- The Wiley Handbook of Contextual Behavioral Science
- ADVANCED PRACTICE IN ACT
- ACT Questions and Answers: A Practitioner’s Guide to 150 Common Sticking Points in Acceptance and Commitment Therapy
- ACT Verbatim for Depression and Anxiety: Annotated Transcripts for Learning Acceptance and Commitment Therapy
- Advanced Acceptance and Commitment Therapy: The Experienced Practitioner’s Guide to Optimizing Delivery
- Advanced Training in ACT: Mastering Key In-Session Skills for Applying Acceptance and Commitment Therapy
- Cognitive Defusion in Practice: A Clinician’s Guide to Assessing, Observing, and Supporting Change in Your Client (The Context Press Mastering ACT Series)
- Getting Unstuck in ACT: A Clinician’s Guide to Overcoming Common Obstacles in Acceptance and Commitment Therapy
- Inside This Moment: A Clinician’s Guide to Promoting Radical Change Using Acceptance and Commitment Therapy
- Learning ACT: An Acceptance and Commitment Therapy Skills Training Manual for Therapists
- Learning ACT for Group Treatment: An Acceptance and Com-mitment Therapy Skills Training Manual for Therapists
- Metaphor in Practice: A Professional’s Guide to Using the Science of Language in Psychotherapy
- Mindfulness for Two: An Acceptance and Commitment Therapy Approach to Mindfulness in Psychotherapy
ACT in Practice
ACT in Practice
Welcome to the companion website for the book!
Case conceptualization is an important part of any psychotherapeutic approach, and the ACT in Practice book helps therapists learn how to take clinically useful ideas from Acceptance and Commitment Therapy, and actually put them into practice and formulate treatments for a wide variety of clinical concerns.
The first section of the book offers an introduction to Acceptance and Commitment Therapy, an overview of the impact of ACT, and a brief introduction to the ACT's "hexaflex" model. The book also describes how to accomplish case conceptualizations in general and offers review of the literature on the importance and value of case conceptualization.
The first section closes with synopsis of the first, second, and third wave of behavior therapy with explanations of how the different waves would have treated hypothetical clients in specific situations.
The second section of the book covers ways that different ACT approaches can be applied to actual practice.
Quizzes at the end of each chapter help the reader evaluate the information they have just learned.
Please click on the links below for additional information and resources!
ACT Training and Supervision by the Authors
ACT Training and Supervision by the AuthorsPatty and D.J. have been training therapists in ACT and providing supervision in clinical behavior analysis since 2001.
If you are interested in having clinical tapes and videos reviewed for “distance supervision,” or would like to organize an ACT training workshop, we would be happy to assist you.
Please contact us for further details: [email protected]
About the Authors
About the AuthorsPatricia A. Bach, Ph.D.
Patty received her doctorate from the University of Nevada in 2000. She is an assistant professor of psychology at the Illinois Institute of Technology in Chicago, where she does ACT and RFT research and trains students of clinical psychology.
Daniel J. Moran, Ph.D., BCBA
D.J. received his doctorate in clinical and school psychology from Hofstra University in 1998. He began his training in acceptance and commitment therapy in 1994 and practices clinical behavior analysis with victims of abuse and individuals with obsessive-compulsive disorder. He is the founder of the MidAmerican Psychological Institute, and director of the Family Counseling Center, a division of Trinity Services, in Joliet, IL.
D.J. is also the host of Functionally Speaking – A 21st Century Behavior Therapy podcast. Listen here!
Case Conceptualization Worksheet
Case Conceptualization WorksheetThis “Inflexahex” model for case conceptualization can assist the clinician in charting and rating clinically relevant concerns in their clients’ lives. Dr. Patty Bach and Dr. D.J. Moran have made the ACT Case Conceptualization form available for download in pdf form, free to paid ACBS members. The form is also below for your convenience. You may select the image below and save it to your computer by right clicking on it and choosing "Save Image As".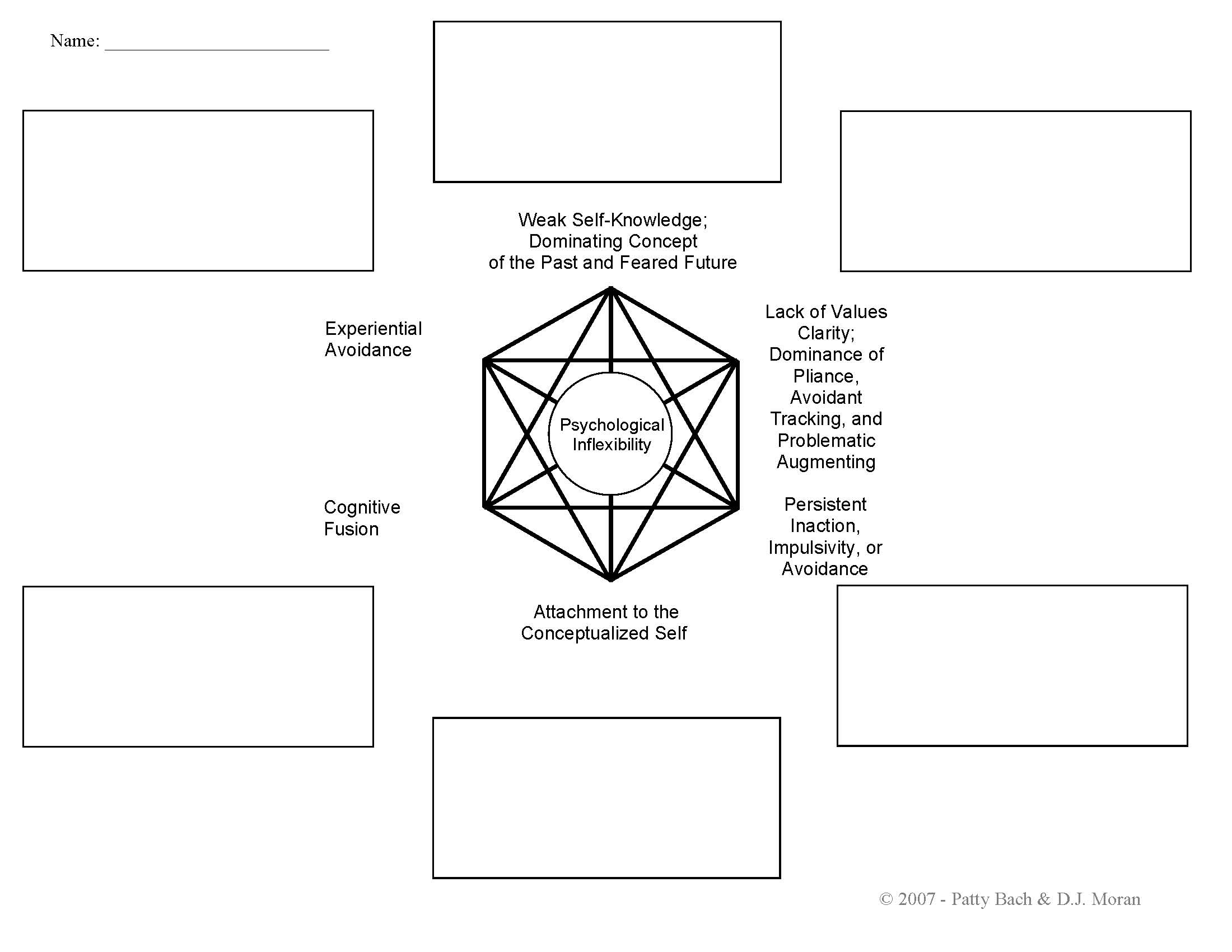
If you would like a free, full-sized pdf copy of the form and are not a paid ACBS member, please email the authors for a copy at [email protected].
ACT Books: Specific Populations
ACT Books: Specific PopulationsACT Books: Specific Populations |
(The following list of books is from the LEARNING ACT RESOURCE GUIDE: The complete guide to resources for learning Acceptance & Commitment Therapy by Jason Luoma, Ph.D. Updated July 2020 learningact.com)
- ANGER
Therapist guides
- Contextual Anger Regulation Therapy: A Mindfulness and Acceptance- Based Approach (Practical Clinical Guidebooks)
Client books
- Act on Life Not on Anger: The New Acceptance & Commitment Therapy Guide to Problem Anger
- The Moral Injury Workbook: Acceptance and Commitment Therapy Skills for Moving Beyond Shame, Anger, and Trauma to Reclaim Your Values
- ANXIETY
Therapist guides
- Acceptance and Commitment Therapy: The Ultimate Guide to Using ACT to Treat Stress, Anxiety, Depression, OCD, and More, Including Mindfulness Exercises and a Comparison with CBT and DBT
- Acceptance and Commitment Therapy for Anxiety Disorders
- Acceptance-Based Behavioral Therapy: Treating Anxiety and Related Challenges
- ACT-Informed Exposure for Anxiety: Creating Effective, Innovative, and Values-Based Exposures Using Acceptance and Commitment Therapy
- The Clinician’s Guide to Exposure Therapies for Anxiety Spectrum Disorders: Integrating Techniques and Applications from CBT, DBT, and ACT
- Trichotillomania: An ACT-Enhanced Behavior Therapy Approach Therapist Guide (Treatments That Work)
Client books
- The ACT on Anxiety Workbook
- The ACT Workbook for OCD: Mindfulness, Acceptance, and Exposure Skills to Live Well with Obsessive-Compulsive Disorder
- Anxiety Happens: 52 Ways to Find Peace of Mind
- Be Mighty: A Woman’s Guide to Liberation from Anxiety, Worry, and Stress Using Mindfulness and Acceptance
- Cognitive Behavioral Therapy: How to Use CBT to Overcome Anxiety, Depression and Intrusive Thoughts + A Guide to Acceptance and Commitment Therapy and ACT Techniques
- The Confidence Gap: A Guide to Overcoming Fear and Self-Doubt
- In This Moment: Five Steps to Transcending Stress Using Mindfulness and Neuroscience
- Living Beyond OCD Using Acceptance and Commitment Therapy: A Workbook for Adults
- The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy (2nd Edition)
- The Mindfulness and Acceptance Workbook for Social Anxiety and Shyness: Using Acceptance and Commitment Therapy to Free Yourself from Fear and Reclaim Your Life
- Outsmart Your Anxious Brain: Ten Simple Ways to Beat the Worry Trick
- Social Courage: Coping and thriving with the reality of social anxiety
- Things Might Go Terribly, Horribly Wrong: A Guide to Life Liberated from Anxiety
- Trichotillomania: An ACT-Enhanced Behavior Therapy Approach Workbook (Treatments That Work)
- The Worry Trap: How to Free Yourself from Worry & Anxiety Using Acceptance and Commitment Therapy
- CANCER
Client books
- Flying over Thunderstorms: Living Your Life with Cancer through Acceptance and Commitment Therapy
- CHILDREN/ADOLESCENTS/PARENTING
Therapist guides
- Acceptance and Commitment Therapy: The Clinician’s Guide for Supporting Parents
- Acceptance & Mindfulness Treatments for Children & Adolescents: A Practitioner’s Guide
- ACT for Adolescents: Treating Teens and Adolescents in Individual and Group Therapy
- ACT for Treating Children: The Essential Guide to Acceptance and Commitment Therapy for Kids
- Challenging Perfectionism: An Integrative Approach for Supporting Young People Using ACT, CBT and DBT
- Mindfulness and Acceptance for Counseling College Students: Theory and Practical Applications for Intervention, Prevention, and Outreach (The Context Press Mindfulness and Acceptance Practical Series)
- Teen Anxiety: A CBT and ACT Activity Resource Book for Helping Anxious Adolescents
- The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection
Client books
- Acceptance and Mindfulness Toolbox for Children and Adolescents: 75+ Worksheets & Activities for Trauma, Anxiety, Depression, Anger & More
- The ACT Workbook for Kids: Fun Activities to Help You Deal with Worry, Sadness and Anger Using Acceptance and Commitment Therapy
- The ACT Workbook for Teens with OCD
- Becoming Mum
- Dark Agents, Book One: Violet and the Trial of Trauma
- Get Out of Your Mind and Into Your Life for Teens: A Guide to Living an Extraordinary Life
- The Gifted Kids Workbook: Mindfulness Skills to Help Children Reduce Stress, Balance Emotions, and Build Confidence
- The Joy of Parenting: An Acceptance and Commitment Therapy Guide to Effective Parenting in the Early Years
- The Mental Health and Wellbeing Workout for Teens: Skills and Exercises from ACT and CBT for Healthy Thinking
- The Mindfulness and Acceptance Workbook for Teen Anxiety: Activities to Help You Overcome Fears and Worries Using Acceptance and Commitment Therapy (Instant Help Book for Teens)
- Nuna and the Fog
- Parenting a Troubled Teen: Manage Conflict and Deal with Intense Emotions Using Acceptance and Commitment Therapy
- Parenting Your Anxious Child with Mindfulness and Acceptance: A Powerful New Approach to Overcoming Fear, Panic, and Worry Using Acceptance and Commitment Therapy
- Stuff That Sucks: Accepting What You Can’t Change and Committing to What You Can
- DEPRESSION
Therapist guides
- ACT for Depression: A Clinician’s Guide to Using Acceptance & Commitment Therapy in Treating Depression
Client books
- The ACT Workbook for Depression and Shame: Overcome Thoughts of Defectiveness and Increase Well-Being Using Acceptance and Commitment Therapy
- The Mindfulness and Acceptance Workbook for Depression: Using Acceptance and Commitment Therapy to Move Through Depression and Create a Life Worth Living (2nd Edition)
- DEVELOPMENTAL DISABILITIES
- Derived Relational Responding Applications for Learners with Autism and Other Developmental Disabilities: A Progressive Guide to Change
- DIVERSE POPULATIONS
Therapist guides
- ACT for Gender Identity
- Mindfulness and Acceptance for Gender and Sexual Minorities: A Clinician’s Guide to Fostering Compassion, Connection, and Equality Using Contextual Strategies
- Mindfulness and Acceptance in Multicultural Competency: A Contextual Approach to Sociocultural Diversity in Theory and Practice (The Context Press Mindfulness and Acceptance Practica Series)
- EATING DISORDERS/BODY IMAGE
Therapist guides
- Acceptance and Commitment Therapy for Body Image Dissatisfaction: A Practitioner’s Guide to Using Mindfulness, Acceptance, and Values-Based Behavior Change Strategies
- Acceptance and Commitment Therapy for Eating Disorders: A Process-Focused Guide to Treating Anorexia and Bulimia
- A Clinician’s Guide to Acceptance-Based Approaches for Weight Concerns: The Accept Yourself! Framework
- ACT for Anorexia Nervosa: A Guide for Clinicians
- Mindfulness and Acceptance for Treating Eating Disorders and Weight Concerns: Evidence-Based Interventions
Client books
- The Anorexia Workbook: How to Accept Yourself, Heal Your Suffering, and Reclaim Your Life
- Living with Your Body and Other Things You Hate: How to Let Go of Your Struggle with Body Image Using Acceptance and Commitment Therapy
- The Diet Trap: Feed Your Psychological Needs and End the Weight Loss Struggle Using Acceptance and Commitment
- HEALTH/CHRONIC PAIN/INTEGRATED CARE
Therapist guides
- Acceptance and Commitment Therapy for Chronic Pain
- Behavioral Consultation and Primary Care: A Guide to Integrating Services
- Contextual Cognitive-Behavioral Therapy for Chronic Pain
- Mindfulness and Acceptance in Behavioral Medicine: Current Theory and Practice
- Psychological Treatment for Patients With Chronic Pain (Clinical Health Psychology)
- Real Behavior Change in Primary Care: Improving Patient Outcomes and Increasing Job Satisfaction
- Somatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy Perspectives
Client books
- Better Living With IBS: A step-by-step program to managing your symptoms so you can enjoy life to the full!
- The Diabetes Lifestyle Book
- End the Insomnia Struggle: A Step-by-Step Guide to Help You Get to Sleep and Stay Asleep
- Living Beyond Lyme: Reclaim Your Life From Lyme Disease and Chronic Illness
- Living Beyond Your Pain: Using Acceptance & Commitment Therapy to Ease Chronic Pain
- INTERPERSONAL/RELATIONSHIP ISSUES
Therapist guides
- Acceptance and Commitment Therapy for Couples: Using Mindfulness, Values, and Schema Awareness to Rebuild Relationships
- Acceptance and Commitment Therapy for Interpersonal Problems: Using Mindfulness, Acceptance, and Schema Awareness to Change Interpersonal Behaviors
- ACT and RFT in Relationships: Helping Clients Deepen Intimacy and Maintain Healthy Commitments Using Acceptance and Commitment Therapy and Relational Frame Theory
- The Interpersonal Problems Workbook: ACT to End Painful Relationship Patterns
Client books
- ACT with Love: Stop Struggling, Reconcile Differences, and Strengthen Your Relationship with Acceptance and Commitment Therapy
- The Mindful Couple: How Acceptance and Mindfulness Can Lead You to the Love You Want
- LOSS/GRIEF
Client books
- The Reality Slap: Finding Peace and Fulfillment When Life Hurts
- OCCUPATIONAL/COACHING
- Acceptance and Mindfulness at Work: Applying Acceptance and Commitment Therapy And Relational Frame Theory to Organizational Behavior Management
- Maximize Your Coaching Effectiveness with Acceptance and Commitment Therapy
- The Mindful and Effective Employee: An Acceptance and Commitment Therapy Training Manual for Improving Well-Being and Performance
- PSYCHOSIS
Therapist guides
- Acceptance and Commitment Therapy and Mindfulness for Psychosis
- ACT for Psychosis Recovery: A Practical Manual for Group- Based Interventions Using Acceptance and Commitment Therapy
- Incorporating Acceptance and Mindfulness into the Treatment of Psychosis: Current Trends and Future Directions
- Treating Psychosis: A Clinician’s Guide to Integrating Acceptance and Commitment Therapy, Compassion-Focused Therapy, and Mindfulness Approaches within the Cognitive Behavioral Therapy Tradition
- RELIGION/SPIRITUALITY
Therapist guides
- Acceptance and Commitment Therapy for Christian Clients: A Faith-Based Workbook
- ACT for Clergy and Pastoral Counselors: Using Acceptance and Commitment Therapy to Bridge Psychological and Spiritual Care
- Faith-based ACT for Christian clients: An integrative treatment approach
- SOCIAL WORK
- Mindfulness and Acceptance in Social Work
- SPORTS/HUMAN PERFORMANCE
- The Psychology of Enhancing Human Performance: The Mindfulness-Acceptance-Commitment Approach
- The Winner’s Mind: Strengthening Mental Skills in Athletes
- SUBSTANCE ABUSE/ADDICTION
Therapist guides
- Acceptance and Commitment Therapy for Pathological Gamblers
- Acceptance and Commitment Therapy for Substance Abuse: A Clinician’s Guide to Using Practical Mindfulness and Acceptance- Based Interventions for Alcoholism and Drug Addiction
- Investigating Acceptance and Commitment Therapy within Addictions
- Mindfulness and Acceptance for Addictive Behaviors: Applying Contextual CBT to Substance Abuse and Behavioral Addictions
- Mindfulness-Based Sobriety: A Clinician’s Treatment Guide for Addiction Recovery Using Relapse Prevention Therapy, Acceptance and Commitment Therapy, and Motivational Interviewing
Client books
- Power Over Addiction: A Harm Reduction Workbook for Changing Your Relationship with Drugs
- The Wisdom to Know the Difference: An Acceptance and Commitment Therapy Workbook for Overcoming Substance Abuse
- TRAUMA/PTSD
Therapist guides
- Acceptance and Commitment Therapy for the Treatment of Post-Traumatic Stress Disorder and Trauma-Related Problems: A Practitioner’s Guide to Using Mindfulness and Acceptance Strategies
Client books
- Dark Agents, Book One: Violet and the Trial of Trauma
- Finding Life Beyond Trauma: Using Acceptance and Commitment Therapy to Heal from Post-Traumatic Stress and Trauma-Related Problems
- The PTSD Survival Guide for Teens: Strategies to Overcome Trauma, Build Resilience, and Take Back Your Life (The Instant Help Solutions Series)
- WORK/COACHING/BUSINESS
- Acceptance and Commitment Coaching (Coaching Distinctive Features)
- Acceptance and Mindfulness at Work: Applying Acceptance and Commitment Therapy And Relational Frame Theory to Organizational Behavior Management
- Maximize Your Coaching Effectiveness with Acceptance and Commitment Therapy
- Prosocial: Using Evolutionary Science to Build Productive, Equitable, and Collaborative Groups
- The Mindful and Effective Employee: An Acceptance and Commitment Therapy Training Manual for Improving Well-Being and Performance
- The psychology of enhancing human performance: The Mindfulness-Acceptance-Commitment (MAC) approach
- YOGA
- Mindful Yoga-Based Acceptance and Commitment Therapy: Simple Postures and Practices to Help Clients Achieve Emotional Balance
ACT Books: Self Help
ACT Books: Self HelpSelf-Help and Life Enhancement Resources |
Please note that not all ACT self help books have been specifically empirically validated. A list of such studies is here and you can search for additional RCT studies here.
The World Health Organization also distributes an extensively validated free ACT self-help book Doing What Matters in Times of Stress: An Illustrated Guide and audio recordings to go with it: https://www.who.int/publications-detail/9789240003927
(The following list of books is from the LEARNING ACT RESOURCE GUIDE: The complete guide to resources for learning Acceptance & Commitment Therapy by Jason Luoma, Ph.D. Updated July 2020 learningact.com)
Self-Help, Self-Improvement, and Skills Workbooks
- ACT SELF HELP BOOKS
- Acceptance and Commitment Therapy: Principles of Becoming More Flexible, Effective, and Fulfilled
- The ACT Deck: 55 Acceptance & Commitment Therapy Practices to Build Connection, Find Focus and Reduce Stress
- ACTivate Your Life: Using acceptance and mindfulness to build a life that is rich, fulfilling and fun
- Break Free: Acceptance and Commitment Therapy in 3 Steps: A Workbook for Overcoming Self-Doubt and Embracing Life
- Cognitive Behavioral Therapy: A Guide to Self-Empowerment with CBT, DBT, and ACT: How to Build Brain Strength and Reshape Your Life with Behavioral Therapy
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous Life
- The Diet Trap: Feed Your Psychological Needs and End the Weight Loss Struggle Using Acceptance and Commitment Therapy
- Escaping the Emotional Roller Coaster: ACT for the emotionally sensitive
- Get Out of Your Mind and Into Your Life: The New Acceptance and Commitment Therapy
- Get the Life You Want: Finding Meaning and Fulfillment through Acceptance and Commitment Therapy
- The Happiness Trap: How to Stop Struggling and Start Living
- How to Be Nice to Yourself: The Everyday Guide to Self Compassion: Effective Strategies to Increase Self-Love and Acceptance
- The Illustrated Happiness Trap: How to Stop Struggling and Start Living
- Learning to Thrive: An Acceptance and Commitment Therapy Workbook
- The Mindfulness and Acceptance Workbook for Self Esteem
- The Mindfulness and Acceptance Workbook for Stress Reduction: Using Acceptance and Commitment Therapy to Manage Stress, Build Resilience, and Create the Life You Want (A New Harbinger Self-Help Workbook)
- The Power of Small: Making Tiny Changes When Everything Feels Too Much
- Reclaim Your Life: Acceptance and Commitment Therapy in 7 Weeks
- Sex ACT: Unleash the Power of Your Sexual Mind with Acceptance & Commitment Therapy
- Stress Less, Live More: How Acceptance and Commitment Therapy Can Help You Live a Busy yet Balanced Life
- Therapy Quest: An Interactive Journey Through Acceptance And Commitment Therapy
- Your Life on Purpose: How to Find What Matters and Create the Life You Want
Self Help Books for Specific Populations
- ANGER
- Act on Life Not on Anger: The New Acceptance & Commitment Therapy Guide to Problem Anger
- The Moral Injury Workbook: Acceptance and Commitment Therapy Skills for Moving Beyond Shame, Anger, and Trauma to Reclaim Your Values
- ANXIETY
- The ACT on Anxiety Workbook
- The ACT Workbook for OCD: Mindfulness, Acceptance, and Exposure Skills to Live Well with Obsessive-Compulsive Disorder
- Anxiety Happens: 52 Ways to Find Peace of Mind
- Be Mighty: A Woman’s Guide to Liberation from Anxiety, Worry, and Stress Using Mindfulness and Acceptance
- Cognitive Behavioral Therapy: How to Use CBT to Overcome Anxiety, Depression and Intrusive Thoughts + A Guide to Acceptance and Commitment Therapy and ACT Techniques
- The Confidence Gap: A Guide to Overcoming Fear and Self-Doubt
- In This Moment: Five Steps to Transcending Stress Using Mindfulness and Neuroscience
- Let Go of Anxiety: Climb Life’s Mountains with Peace, Purpose, and Resilience
- Living Beyond OCD Using Acceptance and Commitment Therapy: A Workbook for Adults
- The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy (2nd Edition)
- The Mindfulness and Acceptance Workbook for Social Anxiety and Shyness: Using Acceptance and Commitment Therapy to Free Yourself from Fear and Reclaim Your Life
- Outsmart Your Anxious Brain: Ten Simple Ways to Beat the Worry Trick
- Social Courage: Coping and thriving with the reality of social anxiety
- Ten Little Ways to Beat the Worry Trick: Outsmart Anxiety, Fear, and Panic
- Things Might Go Terribly, Horribly Wrong: A Guide to Life Liberated from Anxiety
- Trichotillomania: An ACT-Enhanced Behavior Therapy Approach Workbook (Treatments That Work)
- The Worry Trap: How to Free Yourself from Worry & Anxiety Using Acceptance and Commitment Therapy
- CANCER
- Flying over Thunderstorms: Living Your Life with Cancer through Acceptance and Commitment Therapy
- CHILDREN/ADOLESCENTS/PARENTING
- Acceptance and Mindfulness Toolbox for Children and Adolescents: 75+ Worksheets & Activities for Trauma, Anxiety, Depression, Anger & More
- The ACT Workbook for Teens with OCD
- Becoming Mum
- Dark Agents, Book One: Violet and the Trial of Trauma
- Get Out of Your Mind and Into Your Life for Teens: A Guide to Living an Extraordinary Life
- The Gifted Kids Workbook: Mindfulness Skills to Help Children Reduce Stress, Balance Emotions, and Build Confidence
- The Joy of Parenting: An Acceptance and Commitment Therapy Guide to Effective Parenting in the Early Years
- The Mental Health and Wellbeing Workout for Teens: Skills and Exercises from ACT and CBT for Healthy Thinking
- The Mindfulness and Acceptance Workbook for Teen Anxiety: Activities to Help You Overcome Fears and Worries Using Acceptance and Commitment Therapy (Instant Help Book for Teens)
- Nuna and the Fog
- Parenting a Troubled Teen: Manage Conflict and Deal with Intense Emotions Using Acceptance and Commitment Therapy
- Parenting Your Anxious Child with Mindfulness and Acceptance: A Powerful New Approach to Overcoming Fear, Panic, and Worry Using Acceptance and Commitment Therapy
- Stuff That Sucks: Accepting What You Can’t Change and Committing to What You Can
- DEPRESSION
- The Mindfulness and Acceptance Workbook for Depression: Using Acceptance and Commitment Therapy to Move Through
- Depression and Create a Life Worth Living (2nd Edition)
- EATING DISORDERS/BODY IMAGE
- The Anorexia Workbook: How to Accept Yourself, Heal Your Suffering, and Reclaim Your Life
- Living with Your Body and Other Things You Hate: How to Let Go of Your Struggle with Body Image Using Acceptance and Commitment Therapy
- HEALTH/CHRONIC PAIN/INTEGRATED CARE
- Better Living With IBS: A step-by-step program to managing your symptoms so you can enjoy life to the full!
- The Diabetes Lifestyle Book
- End the Insomnia Struggle: A Step-by-Step Guide to Help You Get to Sleep and Stay Asleep
- Living Beyond Lyme: Reclaim Your Life From Lyme Disease and Chronic Illness
- Living Beyond Your Pain: Using Acceptance & Commitment Therapy to Ease Chronic Pain
- INTERPERSONAL/RELATIONSHIP ISSUES
- ACT with Love: Stop Struggling, Reconcile Differences, and Strengthen Your Relationship with Acceptance and Commitment Therapy
- The Mindful Couple: How Acceptance and Mindfulness Can Lead You to the Love You Want
- Saying The Wrong Thing: How to Speak Up in Difficult, Controversial, or Emotionally Charged Conversations
- LOSS/GRIEF
- The Reality Slap: Finding Peace and Fulfillment When Life Hurts
- SPORTS/HUMAN PERFORMANCE
- The Psychology of Enhancing Human Performance: The Mindfulness-Acceptance-Commitment Approach
- The Winner’s Mind: Strengthening Mental Skills in Athletes
- SUBSTANCE ABUSE/ADDICTION
- Power Over Addiction: A Harm Reduction Workbook for Changing Your Relationship with Drugs
- The Wisdom to Know the Difference: An Acceptance and Commitment Therapy Workbook for Overcoming Substance Abuse
- TRAUMA/PTSD
- Dark Agents, Book One: Violet and the Trial of Trauma
- Finding Life Beyond Trauma: Using Acceptance and Commitment Therapy to Heal from Post-Traumatic Stress and Trauma-Related Problems
- The PTSD Survival Guide for Teens: Strategies to Overcome Trauma, Build Resilience, and Take Back Your Life (The Instant Help Solutions Series
RFT/Behavior Analysis Books
RFT/Behavior Analysis Books- Dixon, M.R., Hayes, S.C., & Belisle, J. (2023). Acceptance and Commitment Therapy for Behavior Analysts. New York: Routledge.
- Ming, S., Gould, E., & Fiebig, J. (2023). Understanding and Applying Relational Frame Theory: Mastering the Foundations of Complex Language in Our Work and Lives as Behavior Analysts. Context Press.
- Fryling, M., Rehfeldt, R. A., Tarbox, J., & Hayes, L. J. (Eds.). (2020). Applied Behavior Analysis of Language and Cognition: Core Concepts and Principles for Practitioners. New Harbinger Publications.
- Villatte, M., Villatte, J. L., & Hayes, S. C. (2019). Mastering the clinical conversation: Language as intervention. New York: The Guilford Press.
- Törneke, N., Luciano, C., Barnes‐Holmes, Y., & Bond, F. W. (2015). RFT for clinical practice: Three core strategies in understanding and treating human suffering. Chapter in The Wiley handbook of contextual behavioral science, 254-272.
- Dahl, J., Stewart, I., Martell, C., Kaplan, J. (2014) ACT and RFT in Relationships: Helping Clients Deepen Intimacy and Maintain Healthy Commitments Using Acceptance and Commitment Therapy and Relational Frame Theory.
- Dymond, S., & Roche, B. (Eds.) (2013). Advances in relational frame theory: Research and application. New Harbinger Publications.
- McHugh, L., & Stewart, I. (2012). The self and perspective taking: Contributions and applications from modern behavioral science. Oakland: New Harbinger Publications.
- Törneke, N. (2010). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Reno, NV: Context Press.
- German Translation: Törneke, N. (2012). Bezugsrahmentheorie : Eine Einführung. Paderborn: Junfermann Verlag. (translated by Guido Plata)
- Korean translation: Törneke, N. (2019). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Hakjisa (translated by Lee, S.).
- Spanish Transation: Törneke, N. (2016). Aprendiendo TMR : una introducción a la Teoría del Marco Relacional y sus aplicaciones clínicas. Úbeda, Jaén: Didacbook. - Rehfeldt, R. A., Barnes-Holmes, Y. (2009). Derived relational responding: Applications for learners with autism and other developmental disabilities. Oakland, CA: New Harbinger Publications, Inc.
- Derived Relational Responding offers a series of revolutionary intervention programs for applied work in human language and cognition targeted at students with autism and other developmental disabilities. It presents a program drawn from derived stimulus relations that you can use to help students of all ages acquire foundational and advanced verbal, social, and cognitive skills. The first part of Derived Relational Responding provides step-by-step instructions for helping students learn relationally, acquire rudimentary verbal operants, and develop other basic language skills. In the second section of this book, you'll find ways to enhance students' receptive and expressive repertoires by developing their ability to read, spell, construct sentences, and use grammar. Finally, you'll find out how to teach students to apply the skills they've learned to higher order cognitive and social functions, including perspective-taking, empathy, mathematical reasoning, intelligence, and creativity. This applied behavior analytic training approach will help students make many substantial and lasting gains in language and cognition not possible with traditional interventions. - Dahl, J. C., Plumb, J. C., Stewart, I., & Lundgren, T. (2009). The Art and Science of Valuing in Psychotherapy: Helping Clients Discover, Explore, and Commit to Valued Action Using Acceptance and Commitment Therapy. Oakland, CA; New Harbinger Publications, Inc.
- The Art and Science of Valuing in Psychotherapy is an applied volume in purpose, but includes an RFT account of each of the ACT processes, and in particular an in depth RFT perspective on personal values and the clinical interventions employed to enhance them and promote committed action. - Ramnero, J., & Törneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- The ABCs of Human Behavior offers the practicing clinician a solid and practical introduction to the basics of modern behavioral psychology. The book focuses both on the classical principles of learning as well as more recent developments that explain language and cognition in behavioral and contextual terms. These principles are not just discussed in the abstract—rather the book shows how the principles of learning apply in a clinical context. Practical and easy to read, the book walks you through both common sense and clinical examples that will help you use behavioral principles to observe, explain, and influence behavior in a therapeutic setting. - Miltenberger, R.G., (2008). Behavior modification: Principles and procedures (4th Ed.). Pacific Grove, CA: Thomson/Wadsworth.
- Woods, D. W., & Kanter, J. W. (Eds.). (2007). Understanding behavior disorders: A contemporary behavioral perspective. Reno, NV: Context Press.
- Understanding behavior disorders presents a contemporary behavioral model of behavior disorders that incorporates the findings of current RFT and ACT research. Rich in possibilities for clinical work, this view of disordered behavior is an important milestone in clinical psychotherapy - an opportunity for behavioral clinicians to reintegrate their clinical practice with an experimental analysis of behavior. - Cooper, J.O., Heron, T.E. & Heward, W.L. (2007). Applied Behavior Analysis (2nd Edition). Prentice Hall.
- Applied Behavior Analysis (2nd Edition) is great resource to get you ready for the BCBA exam and to understand basic principals. - Baum, W. M. (2004). Understanding Behaviorism: Behavior, Culture, and Evolution (2nd edition). Wiley-Blackwell.
- Pierce, W.D. & Cheney, C.D. (2003). Behavior Analysis and Learning, 3rd edition.Lawrence Erlbaum.
- The "focus on research" and "on the applied side" sections in various chapters add an excellent generalization of concepts into interesting areas. There is a section on Bandura and the Bobo doll, review of Sidman's comments on coercion, review of the intrinsic/extrinsic reinforcement debates, a creativity section, respondent conditioning and heroin overdose, medical conditioning, and much more. - Barnes-Holmes, Y., Hayes, S. C., Barnes-Holmes, D., & Roche, B. (2001). Relational frame theory: A post-Skinnerian account of human language and cognition. In H. W. Reese & R. Kail (Eds.), Advances in Child Development and Behavior, Volume 28 (pp. 101-138). New York: Academic.
- Baldwin, J.D. & Baldwin, J.I. (2000). Behavior Principles in Everyday Life (4th Edition). Prentice Hall.
- Behavior Principles in Everyday Life (4th Edition) is a really accessible account of behavioral principles. Great accompaniment to ABCs of Human Behavior. - Dougher, M. J. (Ed.). (2000). Clinical Behavior Analysis. Reno, NV: Context Press.
- Chiesa, M. (1994). Radical Behaviorism: The philosophy and science. Cambridge Center.
- Leigland, S. (1992). Radical behaviorism: Willard Day on psychology and philosophy. Reno, NV: Context Press.
Puts Skinner's work in context; links history/philosophy and the battles of minds as a background to RFT/ACT. - Catania, C. (1992). Learning. Prentice Hall.
- Hayes, S. C. (Ed.). (1989/2004). Rule Governed behavior: Cognition, contingencies, and instructional control. New York: Plenum / reprinted in 2004 by Context Press.
- One of the first full-length presentations of the ACT / RFT model is in three chapters in this book on the topic. - Skinner, B.F. (1965). Science and Human Behavior. Free Press.
ACT Books in 20+ Languages
ACT Books in 20+ Languages CommunityGeneral Purpose Books on Contextual Behavioral Science
General Purpose Books on Contextual Behavioral ScienceGeneral Purpose Books on Contextual Behavioral Science |
- McHugh, L., Stewart, I., & Almada, P. (2019). A Contextual Behavioral Guide to the Self: Theory and Practice. Oakland, CA: New Harbinger.
- Wilson, D.S., Hayes, S.C. (2018) Evolution and Contextual Behavioral Science: An Integrated Framework for Understanding, Predicting, and Influencing Human Behavior. Context Press.
- Zettle, R. D., Hayes, S.C., Barnes-Holmes, D., Biglan, A. (2016) The Wiley Handbook of Contextual Behavioral Science (Wiley Clinical Psychology Handbooks) Wiley-Blackwell.
Ramnero, J., & Torneke, N. (March 2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: Context Press / New Harbinger.
It's a basic behavior analysis book for clinicians/ M.D.s/ psychiatrists/ etc. who haven't had training in BA. Goes all the way up to RFT. Nice.
Woods, D. W., & Kanter, J. W. (Eds.). (2007). Understanding behavior disorders: A contemporary behavioral perspective. Oakland, CA: Context Press/New Harbinger.
This volume presents a contemporary behavioral model of behavior disorders that incorporates the findings of current RFT and ACT research. Rich in possibilities for clinical work, this view of disordered behavior is an important milestone in clinical psychotherapy - an opportunity for behavioral clinicians to reintegrate their clinical practice with an experimental analysis of behavior.
Biglan, A. (1995). Changing cultural practices: A contextualistic framework for intervention research. Oakland, CA: Context Press/New Harbinger.
This is begins to show how you might scale these issues to the level of cultural practices. If the ACT model is correct, we either alter the prevalence of psychological inflexibility or we fail to help the human condition. You can do that one at a time, or in formal prevention efforts, but either way it is the same bottom line. No change in prevalence = failure. So we need to think about how to measure this and approach this wisely throughout the work we are doing.
Hayes, S. C., Hayes, L. J., Reese, H. W., & Sarbin, T. R. (Eds.). (1993). Varieties of scientific contextualism. Oakland, CA: Context Press/New Harbinger.
If you get interested in the philosophical foundations of ACT, this will help you understand them.
Leigland, S. (1992). Radical behaviorism: Willard Day on psychology and philosophy. Oakland, CA: Context Press/New Harbinger.
Puts Skinner's work in context; links history/philosophy and the battles of minds as a background to RFT/ACT.
Hayes, S. C. (Ed.). (1989/2004). Rule Governed behavior: Cognition, contingencies, and instructional control. New York: Plenum / reprinted in 2004 by Context Press and currently sold by Oakland, CA: Context Press/New Harbinger..
One of the first full-length presentations of the ACT / RFT model is in three chapters in this book on the topic. This book is now available in paperback from Context Press.
FAP and CFT Books
FAP and CFT Books- FAP Books
- Gareth Holman PhD, Jonathan Kanter PhD, Mavis Tsai PhD, Robert Kohlenberg PhD, Steven C. Hayes (2017) Functional Analytic Psychotherapy Made Simple.
- Mavis Tsai, Robert J. Kohlenberg, Jonathan W. Kanter, Gareth I. Holman, Mary Plummer Loudon (2012) Functional Analytic Psychotherapy (CBT Distinctive Features)
- Mavis Tsai, Robert J. Kohlenberg, Jonathan W. Kanter, Barbara Kohlenberg, William C. Follette, Glenn M. Callaghan. (2008) The Practice of Functional Analytic Psychotherapy.
- Mavis Tsai, Robert J. Kohlenberg, Jonathan W. Kanter, Barbara Kohlenberg, William C. Follette, Glenn M. Callaghan (2008) A Guide to Functional Analytic Psychotherapy: Awareness, Courage, Love, and Behaviorism.
- Mavis Tsai, Robert J. Kohlenberg. (2007) Functional Analytic Psychotherapy: Creating Intense and Curative Therapeutic Relationships. (Published in 1991 and republished in 2007)
- Translations of FAP Books
- Italian: Tsai, M. Kohlenberg, R., Kanter, J. W., Holman, G., Plummer Loudon, M. (2013). La psicoterapia analitico-funzionale (FAP). Caratteristiche distintive. (Ed. C. Orsini) Franco Angeli Edizioni.
- Portuguese: Holman, G., Kanter, J. W., Tsai, M., & Kohlenberg, R. (2022). Psicoterapia Analítica Funcional Descomplicada: Guia Prático Para Relações Terapêuticas (Rolim de Moura, P., Bastos Oshiro, C. K., & Villas-Bôas, A., Trans). Sinopsys Editora.
- Spanish: Kanter, J. W., Tsai, M., & Kohlenberg, R. J. (2021). La práctica de la psicoterapia analítico-funcional. (Ed J. Virues-Ortega) ABA Espanay.
- Spanish: Kohlenberg, R. J. & Tsai, M. (2021). FAP. Psicoterapia Analítico Funcional: Creación de relaciones terapéuticas intensas y curativas. Editociones Psara
- Compassion Focused Therapy Books for Therapists
- Gilbert, P. & Simos, G. (Editors) (2022). Compassion Focused Therapy: Clinical Practice and Applications. Routledge.
- Kolts, R.L., Bell, T., Bennett-Levy, J., Irons, C. (2018) Experiencing Compassion Focused Therapy from the Inside Out.
- Kolts, R.L. (2016) CFT Made Simple - An excellent and very readable introduction to compassion-focused therapy, with a fantastic chapter showing how to use chair-work with highly self-critical clients.
- Tirch, D., Schoendorff, B., Silberstein, L.R. (2014) The ACT Practitioner's Guide to the Science of Compassion - This is the first book on the market to provide an in-depth discussion of compassion in the context of ACT and other behavioral sciences. It offers case conceptualization, assessments, and direct clinical applications that integrate ACT, functional analytic psychotherapy, and compassion focused therapy to enhance your clinical practice.
- Gilbert, P. (2010) Compassion-Focused Therapy: Distinctive Features - A key reference source for learning compassion-focused therapy. It's concise, filled with clinical wisdom, and a handy reference for thinking through how to work with shame and self-criticism.
- Gilbert, P. (2009). The Compassionate Mind. London: Constable.
- Books based on Compassion-Focused Therapy for Clients
- How to Be Nice to Yourself: The Everyday Guide to Self Compassion by Laura Silberstein-Tirch (2019)
- The Mindful Self-Compassion Workbook: A Proven Way to Accept Yourself, Build Inner Strength, and Thrive by Kristin Neff and Christopher Germer (2018)
- Self-Compassion: The Proven Power of Being Kind to Yourself by Kristin Neff
- Compassion Focused Therapy for Dummies - From the publisher: Compassion Focused Therapy For Dummies is a wonderful resource if you are seeing—or thinking about seeing—a therapist who utilizes compassion techniques, or if you would like to leverage the principles of compassion focused therapy to manage your own wellbeing.
- Mindful Compassion: How the Science of Compassion Can Help You Understand Your Emotions, Live in the Present, and Connect Deeply with Others. This book by Paul Gilbert (creator of compassion-focused therapy) and Choden (a Buddhist monk) presents the principles of compassion-focused therapy in an accessible manner. A great book for people wanting to develop a kinder, more compassionate way of related to themselves and others.
- The Power of Self-Compassion: Using Compassion-Focused Therapy to End Self-Criticism and Build Self-Confidence by Welford and Gilbert. This book uses tools from Compassion-Focused Therapy to guide increased self-compassion and self-confidence.
- An Open-Hearted Life: Transformative Methods for Compassionate Living from a Clinical Psychologist and a Buddhist Nun is written in short chapters that make it easy to consume. Each chapter can be read in one sitting, each has a brief exercise to put to use the concepts therein, and each covers one topic that is important to living a more compassionate life.
- The Compassionate Mind Guide to Overcoming Anxiety - This book is written primarily from the perspective of compassion-focused therapy, but also integrates techniques from acceptance and commitment therapy. This might be a particularly relevant book for people who are both anxious and highly self-critical.
- The Mindful Path to Self-Compassion: Freeing Yourself from Destructive Thoughts and Emotions. By C.K. Germer
- The Compassionate-Mind Guide to Managing Your Anger – A book based on compassion-focused therapy on how to bring compassion to the pain of anger and feeling threatened.
- The Compassionate-Mind Guide to Recovering from Trauma and PTSD - A book based on compassion-focused therapy on how to bring compassion to people who have survived trauma and abuse.
- The Compassionate-Mind Guide to Ending Overeating - A book based on compassion-focused therapy for people who binge or suffer from disordered eating.
- The Compassionate-Mind Guide to Building Social Confidence - A book based on compassion-focused therapy for people who are shy or suffer from social anxiety.
- Mindfulness and other Third Generation Books
- Jonathan Feiner (2020). Mindfulness: A Jewish Approach. Mosaica Press.
- Christopher Germer, Ronald D. Siegel, and Paul R. Fulton, Editors (2016) Mindfulness and Psychotherapy, Second Edition.
- Ann F. Haynos, Evan Forman, Meghan Butryn, and Jason Lillis, Editors (2016) Mindfulness and Acceptance for Treating Eating Disorders and Weight Concerns: Evidence-Based Interventions
- Matthew D. Skinta and Aisling Curtin (2016) Mindfulness and Acceptance for Gender and Sexual Minorities: A Clinician's Guide to Fostering Compassion, Connection, and Equality Using Contextual Strategies
- Dennis Tirch, Laura R. Silberstein-Tirch, Russell L. Kolts (2015) Buddhist Psychology and Cognitive-Behavioral Therapy: A Clinician's Guide
- Paul Gilbert and Choden. (2014). Mindful Compassion: How the Science of Compassion Can Help You Understand Your Emotions, Live in the Present, and Connect Deeply with Others.
- Matthew S. Boone, Editor (2014) Mindfulness and Acceptance in Social Work: Evidence-Based Interventions and Emerging Applications
- Jason M. Stewart, Editor (2014) Mindfulness, Acceptance, and the Psychodynamic Evolution: Bringing Values into Treatment Planning and Enhancing Psychodynamic Work
- Jacqueline Pistorello, Editor (2013) Mindfulness and Acceptance for Counseling College Students: Theory and Practical Applications for Intervention, Prevention, and Outreach
- Todd B. Kashdan and Joseph Ciarrochi, Editors (2013) Mindfulness, Acceptance, and Positive Psychology: The Seven Foundations of Well-Being
- Steven C. Hayes and Michael Levin, Editors (2012) Mindfulness and Acceptance for Addictive Behaviors: Applying Contextual CBT to Substance Abuse and Behavioral Addictions
- Lance McCracken (2011) Mindfulness and Acceptance in Behavioral Medicine: Current Theory and Practice
- Steven C. Hayes, Victoria M. Follette, and Marsha M. Linehan, Editors (2011) Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition
- Richard W. Sears, Dennis D. Tirch, Robert B. Denton (2011) Mindfulness in Clinical Practice
- Lizabeth Roemer and Susan M. Orsillo (2010) Mindfulness- and Acceptance-Based Behavioral Therapies in Practice (Guides to Individualized Evidence-Based Treatment)
- Ruth Baer, Editor (2010) Assessing Mindfulness and Acceptance Processes in Clients: Illuminating the Theory and Practice of Change
- Kelly G. Wilson PhD and Troy DuFrene (2009) Mindfulness for Two: An Acceptance and Commitment Therapy Approach to Mindfulness in Psychotherapy
- Kashdan, T. (2009). Curious? Discover the missing ingredient to a fulfilling life. New York, NY: Harper Collins.
- Flowers, S.H. (2009). The Mindful Path Through Shyness: How Mindfulness and Compassion Can Free You From Social Anxiety, Fear, and Avoidance. Oakland, CA: New Harbinger.
- Vieten, C. (2009). Mindful Motherhood: Practical Tools for Staying Sane During Pregnancy and Your Child’s First Year. Oakland, CA: New Harbinger.
- Greco, L., & Hayes, S. C. (Eds.). (2008). Acceptance and mindfulness treatments for children and adolescents: A practitioner's guide. Oakland, CA: New Harbinger. Shows how the work in acceptance and mindfulness is impacting the treatment of children and adolescents. Several ACT chapters; also includes DBT, MBCT, MBSR etc
- Baer, R. A. (Ed.). (2005). Mindfulness-based treatment approaches: Clinician's guide to evidence base and applications. New York: Academic Press. This book discusses the conceptual foundation, implementation, and evidence base for the four best-researched mindfulness treatments: mindfulness-based stress reduction (MBSR), mindfulness-based cognitive therapy (MBCT), dialectical behavior therapy (DBT) and acceptance and commitment therapy (ACT). All chapters were written by researchers with extensive clinical experience. Each chapter includes the conceptual rationale for using a mindfulness-based treatment and a review of the relevant evidence base.
- Orsillo, S. M., & Roemer, L. (Eds). (2005). Acceptance and mindfulness-based approaches to anxiety: New directions in conceptualization and treatment. New York: Kluwer Academic/Plenum. Includes conceptual and practical applications of ACT and other third-wave therapies to the anxiety disorders, with chapters covering ACT, DBT skills, and MBSR, as well as specific anxiety disorders, anxiety in children and basic research in anxiety and acceptance.
- Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2004). Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition. New York: Guilford Press. Meet most of the major approaches in the third wave. Shows that ACT is not alone. Lots of good ideas for expanding your clinical work inside a third wave model. More theoretical though than immediately practical.
- Dougher, M. J. (Ed.). (2000). Clinical Behavior Analysis. Oakland, CA: Context Press/NewHarbinger. Situates ACT, Behavioral Activation, and other approaches in clinical behavior analysis. That is the tradition where this work comes from.
- Hayes, S. C., Jacobson, N. S., Follette, V. M., & Dougher, M. J. (Eds.). (1994). Acceptance and change: Content and context in psychotherapy. Oakland, CA: Context Press/New Harbinger. The first comprehensive third wave book. It carved out the domain we are now busy filling. Still relevant, despite its age.
Books (Archives)
Books (Archives) CommunityACT Study Group for Beginners
ACT Study Group for BeginnersHow This Came About
In February 2004 several beginners, interested but little experienced with ACT, found themselves on the ACT listserve. The idea arose for launching an on-line study group for beginners. Very soon 30 or more folks signed in, and the “ACT study group for beginners” was born.
We began reading the book chapter by chapter, and discussing it on the listserve. The first, theoretical part was tough. Kate Partridge raised the idea of starting each discussion with a summary of a section of the book. The summarizing began on 04/13/04, when we reached the clinical part of the book.
What you find below is a uncensured, uncorrected collection of the summaries. They’re meant for discussion, not for teaching purposes per se, but we are allowing them to become part of this website simply because we hope they might be useful to other beginners. People from 7 countries did parts of it: Australia, Belgium, Canada, Netherlands, Spain, United Kingdom, and the USA. (More countries participated in the discussion: Germany, Israel, Sweden, …) It was fun to participate, and very inspiring, … but sometimes hard too: we chose a fixed schedule of weekly reading, discussing, and sometimes summarizing … but we were willing and committed.
Part of the value in doing this probably cannot be achieved just by reading these products. This way we structured it beginners, hesitatant to take part in discussions between more experienced ACT-ors, had unique learning opportunities by taking part in the beginners’ discussion. The “masters” could watch us and interfered when helpful, which also was stimulating. I can recommend the formula to other beginners and hesitating “lurkers”. It might be worth while to start a second round. But that’s up to others. Meanwhile, here are our written products.
Thanks to all beginners who participated, and to the listserve for the opportunity!
ACT Book Summary: Pages 81-86
ACT Book Summary: Pages 81-86Contributed by: Francis De Groot Part II: The clinical methods of ACT Chapters 3 to 9 present the ACT concepts and strategies. ACT = Acceptance and Commitment Therapy = Accept, Choose and Take action Goal: to move in the direction of chosen values, and accept the automatic effects of life's difficulties. Barriers: experiential avoidance & cognitive fusion Source of these barriers: verbal Act stages focus on shift from content of experience to context of experience Why?: to enable clients to pursue valued goals in life. During treatment metaphors, paradoxes, and experiential exercises are frequently used to undermine the traps of literal language and pliance. Metaphors:
- are not specific & proscriptive (less pliance)
- are more like pictures (more experiential)
- are easily remembered
Therapeutic paradox:
- not the classic therapeutic paradox to eliminate certain sympoms: e.g. "don't obey me". They rely on pliance
- = inherent paradox: functional contradictions between literal and functional properties of a verbal event: e.g. "try to be spontaneous"
Experiential exercises: To help contact potentially troublesome thoughts, feelings, memories, ...
- experience in a different context
- allows experience to be observed & studied experientially
- superior to discussing
Summary: More:
- pursuing of valued goals
- direct experience
- acceptance of negative experiences (thoughts, feelings, memories, bodily sensations, ...)
Less:
- literal language
- pliance
Use of: less "literalizing" verbal modalities: metaphors, paradoxes, experiential exercises Focus on: WHAT DOES YOUR EXPERIENCE TELL YOU? This also goes for therapists? Let's go for some tracking, not for pliance!
ACT Book Summary: Pages 87 - 91
ACT Book Summary: Pages 87 - 91Contributed by Kate Partridge Creative Hopelessness: Challenging the Normal Change Agenda [Comments in square brackets are from me. I know this summary is almost as long as the section itself, but doing it has really helped me understand it. Kate] Theoretical Focus Resistance to Change: Clients enter therapy because they have already struggled for a long time with "the problem", in many different ways (contemplation, planning, discussion, praying, reading, tapes, etc.) In spite of so much effort having been exerted, no solution to the problem has arisen. In this sense, the client is resistant to change. There are [at least] two reasons for this: 1) The client has not found the right way to fix the problem. 2) There is a fundamental flaw in the model for change, which is based on culturally sanctioned, language-based rules for solving problems. Culturally Sanctioned [Unconscious] Problem-Solving Rules:
- Psychological problems = the presence of unpleasant inner experiences (feelings, thoughts, sensations, etc.). The presence of these unpleasant experiences signal that "something is wrong and must be changed".
- "Healthy living" = the absence of these negative experiences.
- These experiences need to be eliminated by the correction of inner deficits (e.g., lack of confidence), through the understanding or modification of their causes (e.g., overcritical parents).
The underlying metaconcept is: "The problem is one of bad content; change the content and the problem will go away." ACT Assumption [Message of Hope and Liberation]: The Change Agenda Is Not Workable: The culturally sanctioned problem solving rules are like water to fish - they are taken so much for granted that to challenge them seems nonsensical. The ACT therapist works to undermine the sense of normality surrounding these rules, by showing that efforts based on these rules can actually be the source of problems, not their solution. The therapist asks: • "Which will you believe, your 'mind' or your actual experience of the unworkability of these rules?" [Not expressed in these words, naturally.] The therapist takes apart for the client the underlying logical assumption: 1) Identify the problem: "bad" thoughts and feelings. 2) Eliminate the problem: " " " " 3) Life will then improve. By drawing out multiple examples from the client's own history, the client can become experientially connected to what is often a long series of unsuccessful attempts to use this strategy. This can be quite painful. The therapist aims to organize most of the client's solutions into a general class of events that can be described as: "Control of private experience = Successful living." The client is (gently) encouraged to confront the reality of their multiple experiences of the unworkability of this assumption. This leaves the client often not knowing what to do next, in a state of "creative hopelessness". The state is "creative" because entirely new strategies can be developed with being overwhelmed by the old and previously unconscious rule system. Clinical Focus In this phase of ACT, the therapist focuses on the following issues:
- Client has tried everything, but the problem remains.
- The problem is not one of motivation, nor of specific tactics. The client is not to blame for being stuck.
- There is a paradox here: Working hard to solve the problem makes the problem seem worse. The solution is part of the problem. [I need some concrete examples here of how the solution makes things worse - KAP]
- The logic of the problem-solving system is flawed. A more valid and reliable source of problem-solving is the client's own direct experience and their feedback from life.
TABLE 4.1: ACT Goals, Strategies, and Interventions Regarding Creative Hopelessness. [There is no point in summarizing this useful table. It is on Page 91]. Informed Consent ACT interventions can be intense, and the client must be prepared for this by being provided with:
- general descriptions of operating principles [How general?]
- frank discussion of areas of ambiguity [What does this mean?]
- alternative forms of therapy that could be followed instead of ACT
Treatment involves the client in having to face previously avoided experiences. When this occurs, the client can start to question his/her commitment to treatment. Therefore, the client should be committed to meeting for a certain number of sessions, to expect ups and downs, and to hang in until a progress review occurs at a specified session. In this way, the client is guided away from impulsively dropping out of treatment.
ACT Book Summary: Pages 92 - 98
ACT Book Summary: Pages 92 - 98ACT Book Summary: Pages 98 - 105
ACT Book Summary: Pages 98 - 105- Begins by noting that engendering creative hopelessness is the first ACT intervention (following thorough assessment of the client's 'presenting problem', change agenda, and strategies that have been tried to resolve it.
- Also notes (or warns) that doing this inevitably involves the use of human language, which is part of the trap the client is in anyway - the conundrum of attempting to side- step the trap of language, but needing to use language to deliver interventions. The therapist is thus just as susceptible as the client to the trap of literal language, and must be careful about too strongly believing or becoming fixed on the logic of words.
- This highlights the equality of therapist and client, with the therapist's only advantage that of having an outside perspective (the client would also have this advantage were the therapist's problems the topic of discussion).
- The therapist confronts the system by working outside it, using language only to meet certain ends, not to change beliefs or model more "rational" beliefs and thoughts. If those ends are not met, then the words are not true, no matter how logical. So this takes us from the typical reliance on logic to relying on workability - this become our metric. The question for both clients and therapists is "does that work for you?".
- In the beginning of this section, the authors provide a caveat that it is written with severely affected clients in mind (although the tools are still useful in less severe circumstances).
- The work starts with confrontation, although of a different sort than typically thought. The confrontation is between the client's change agenda and the client's experience of the workability of that system. The message of the therapist and client being in the same boat as far as confronting this system (i.e. the therapist is not some expert who has all the answers) can be powerfully conveyed by the therapist sitting next to the client, with the system imagined as out in front, being confronted by both people together.
- The therapist is armed at this point with information related to strategies the client has tried in the past that haven't worked.
- Unworkability is gently suggested - the therapist highlights how hard the client has been thinking and working at the change agenda, and that consulting a therapist is another attempt to find a solution. Another powerful intervention here is to highlight that usually when we work this hard, things get accomplished, but that this situation seems different. All this effort has not resolved the issue.(this is a subtle way to highlight the role of the client's experience)
- This moves into a discussion of the notion that perhaps looking for solutions is part of the problem. That the client is stuck, and it's not because they are not clever enough to figure it out or are not trying. Perhaps it is because it can't work. The authors suggest that a way to make this more tangible to the client is to suggest that the client doesn't actually believe there is a solution - that anything offered by the therapist would likely just be refuted by the client based on the client' s experience that it would not work. So here, the idea that experience and mind tell the client different things, and that experience is more accurate is brought to the discussion.
- The authors break from the therapeutic dialogue here to discuss the importance of framing creative hopelessness as a positive thing. Being careful not to suggest that the client is hopeless or to engender hopeless feelings. But rather to introduce this idea as a starting point for giving up unworkable strategies and opening up for new possibilities to emerge.
- Several metaphors are provided, including the Man in the Hole metaphor, p. 101, to side-step the trap of language. This metaphor is flexible and can be used to address many issues a client might raise, such as:
- giving up
- belief in the need to delve into the past
- responsibility
- blame
- continuing to look for solutions - this one actually seems really important and I think best highlights the goals of this part of therapy. The therapist really seems to stay away from promising solutions, but takes on a role of saying "I don't know". The goal at this point is batter down the tendency toward sense-making and to stay with the importance of the client giving up unworkable strategies, even without any promise of what will come next. This is a leap of faith and should be noted as such, since clients (like the rest of us) are definitely not used to not trying to make sense of things when there are problems in our lives.
- illustrating the opportunity suffering presents for us to learn to disentangle ourselves from our own minds.
ACT Book Summary: Pages 105 - 110
ACT Book Summary: Pages 105 - 110ACT Book Summary: Pages 110 - 114
ACT Book Summary: Pages 110 - 114ACT Book Summary: Pages 115 - 118
ACT Book Summary: Pages 115 - 118- "Deliberate control works well for me in the external world."
- "I was taught it should work with personal experiences (e.g., 'Don't be afraid...')."
- "It seems to work for other people around me (e.g., 'Daddy never seemed scared...')."
- "It even appears to work with certain experiences I've struggled with (e.g., relaxation works for a while to reduce my anxiety symptoms)." It is emphasized that the examination of control strategies is based entirely on the clients experience, with workability as the unit of analysis, and that the therapist needs to be extremely careful not to dictate or demand that the client evaluate their control strategies as unworkable. Therapist techniques that are mentioned include using metaphors and experiential exercises to help the client develop increasing sensitivity to directly experienced contingencies. Also, the authors mention that asking questions rather than stating conclusions can be helpful in reducing pliance on the part of the client.
ACT Book Summary: Pages 119 - 125
ACT Book Summary: Pages 119 - 125- If I'm not willing to have it (e.g., anxiety), I have it
- If I don't get so uptight about being anxious, I will be less anxious
- If I am willing to have it in order to get rid of it, I am not willing to have it and I will have it again
- contrast between controllable behaviors (i.e., paint the wall or I will shoot you) versus behavior that is not regulated successfully by verbal rules (relax or I'll shoot you)
- People carry their own polygraph with them all the time (their nervous system) and their own gun (self-esteem, self-worth). They are constantly monitoring for symptoms (e.g., anxiety) and firing the gun at themselves
- How seemingly successful attempts to make situation work, don't work in the long term. For example, taking valium may help you relax initially but what about when it wears off?
- either it is particularly difficult not to think about it (me included in this group)
- or attempts to not think about it (e.g., "I thought about something else") actually require you to think about chocolate cake (you have to know what you are not thinking about)
ACT Book Summary: Pages 125 - 132
ACT Book Summary: Pages 125 - 132ACT Book Summary: Pages 132 - 135
ACT Book Summary: Pages 132 - 135- designed to look at concept of control and its relationship to distress
- Should be linked to clients' experience of their own futile effort to control distress, can link it to more mundane or less meaningful examples for the client (for example, trying to sleep during a bout of insomnia. The harder you try to fall asleep the less sleep you get. In supervision, we often use the Chinese finger trap example-the harder you try to get out of it, the less out of it you are- you get stuck.)
- Want to undermine the client's confidence in the control strategy and depathologize the struggle over control
- Not crazy, just using the wrong strategy
ACT Book Summary: Pages 136 - 141
ACT Book Summary: Pages 136 - 141- willingness is appearing spontaneously in situations that used to elicit control
- clients report spontaneous examples of feeling feelings differently
ACT Book Summary: Pages 141 - 147
ACT Book Summary: Pages 141 - 147- personal work for the clinician
- a clinical vignette
- appendices containing daily experiences diary, identifying programming exercise, feeling good exercise, rules of the game exercise and clean versus dirty discomfort diary. I'll deal with each of these in turn:
ACT Book Summary: Pages 148 - 154
ACT Book Summary: Pages 148 - 154Building Acceptance by Defusing Language
Here are some nuts and bolts followed by questions and critiques:
1. The distinction between process and content: language is a learned set of derived stimulus relations, while languaging is the action of deriving those relations.
2. Humans (therapists, clients, etc.) often don't make this distinction and often relate on (and become connected to) the content level. Taking these contents at "face value" (i.e., literally, tangibly) in turn, leads to powerful and predictable behavior patterns (that are often destructive) on the part of the client.
3. One of the main paradoxes in ACT is that language cannot be weakened by more language; however the essence of deliteralization is to take advantage of loopholes in the way language functions (by teaching the client to see that thoughts and feelings are just that-thoughts and feelings).
4. Page 152 contains a table (6.1) of ACT goals, strategies, and interventions to use regarding deliteralization.
5. One of the ways to begin addressing the paradox and function of language is to demonstrate to the client the limits of language in deciphering human experience (and to elicit their own examples). For example, there are two metaphors (found on page 153) that communicate how describing something is different from experiencing it. One metaphor is "finding a place to sit," which essentially describes how talking about a chair (its features, uses) does not help when one wants to actually sit down. In other words, one cannot "sit" in a description of a chair. One can only sit IN an actual chair. A corollary of this metaphor is that one can describe the experience of swimming (how the water feels moving through it, its temperature, etc.). However, one cannot learn to swim in or by a description.
6. There is an assumption in ACT that "your mind is not your friend." Extrapolating from pre-human experience, one can see that the (human) mind was not developed to make humans or "prehumans" feel good. It was developed to keep humans from danger and was mostly comprised of negative content. Explain to clients the paradox "your mind is not your friend AND you cannot live without it."
7. Another assumption is that language is arbitrary and that once it is learned, it becomes relatively independent of immediate environmental support. This reminds me of my nanny's (successful) efforts to train my 20 month-old son to say "bling-bling" when he sees jewelry-now without her having to label it.
8. There is a provocative quote related to the usefulness of nonverbal (experiential?) knowledge at the end of this section on page 154: "If we suddenly had all nonverbal knowledge removed from our repertoires-we would fall to the floor quite helpless."
Comments/questions:
9. It has been my experience that, while clients appear "fused" to a lot of different ideas/contents, a great share of them come to my office without having specific terms/language to describe their experience. In fact they come ONLY with experience, which they have a difficult time describing in words. For example, an extremely anxious patient I had (with Posttraumatic Stress Disorder) wouldn't ever label himself as "anxious," rather he just knows he feels bad.
10. I don't know if behavior patterns follow from the premise that one does not make a distinction between the process of thinking and actual thought, and becomes fused with actual thought content, thereby leading directly to ingrained behavior patterns. I suppose one could explain this as troublesome behavior patterns becoming automatic due to conditioning (i.e., not being aware of the interaction pattern itself); however, I'm not sure if this is because one is fused to a verbal event.
11. Have any of these hypotheses been evaluated using individuals with various types of brain injuries (resulting in apraxia, aphasia, acquired deficits in language versus acquired deficits in motor ability, etc.)?
ACT Book Summary: Pages 154 - 158
ACT Book Summary: Pages 154 - 158- Thoughts are used to structure our perception of the world. We don't even notice that we look at the world from our thoughts, because we believe them in literal way. To look at the process of language involves focusing attention on language as language, cryptic as this may sound. A bit of defusion from literal 'understanding' can be achieved by watching the direct stimulus functions of language like sound, the feeling of your muscles, the sight, etc.
- An elegant way to watch your attention switch from the symbolic function of a word to some of its direct stimulus functions is by repeating a word over and over again for one or two minutes. This is the classic milk, milk, milk exercise (Titchener, 1916). Present it as an experiment or experiential exercise and help the client notice how the literal meaning of the word disappears and one can see the word as an instant of the language process.
- I like the notion of skill learning here. Deliteralization is a skill you can practice, it's not another rule to follow. One can play with direct stimulus properties and thereby loosen the 'grand illusion of language' by realizing that the symbolized thing is not there at all. The only thing that's there is sound, movement, breathing and so on. And this is not a fact, but a skill, something you do.
- You, the driver of the bus. You want to go places and do your job.
- The passengers are your thoughts and all kinds of inner states. Some are nice, some ugly, scary, nasty.
- The scary ones threat you and want to come up front where you'll see them.
- You take this very serious and stop the bus (you don't go anywhere anymore) and try to make a deal with them: they'll keep quiet in the back of the bus, only when you do exactly what they tell you.
- This means your route plan is greatly impaired and you're always on the watch inside the bus.
- What happens is that you let these passengers control the whereabouts of the bus. You, the driver, are not in control at all.
- Even though these passengers look scary, nasty, threatening etc. they can't take control (unless you let them). They can't make you do something against your will.
ACT Book Summary: Pages 158 - 168
ACT Book Summary: Pages 158 - 168ACT Book Summary: Pages 168 - 174
ACT Book Summary: Pages 168 - 174ACT Book Summary: Pages 174 - 179
ACT Book Summary: Pages 174 - 179ACT Book Summary: Pages 180 - 187
ACT Book Summary: Pages 180 - 187- Int: So, we've talked a lot about what your critics think of you and your work, what your wife and ex-wives and children think. I have to ask, what do you think about Clint Eastwood?
- CE: I tend not to think about him very much.
- When I am x and I and my community do much better when I am x, I am pretty invested in remaining x, because if I act as Y there are consequences
- Our history has taught us to see and maintain patterns.
- We have equivalency statements that may not be equivalent "I am 5'10" (maybe 9") becomes the same as "I am alcoholic."
- If I try to act outside of "who I think I am," it seems almost life (or self?) threatening. Note: I wonder about this with the "guys" I work with. Many are domestic violence offenders, and even though their physicality is usually not threatened, many lash out when their sense of "self" is threatened, the "manly man syndrome." OR "Eliminate conceptualization = eliminate me."
ACT Book Summary: Pages 187 - 192
ACT Book Summary: Pages 187 - 192We're looking at the first part of the 'Clinical Focus' section of chapter 7 'Discovering Self, Defusing self'.
As will have been outlined earlier, this is an important part of ACT. The section begins with a brief outline of the core perspectives that are introduced here. Table 7.1 (p.188) provides the ACT goals, strategies and interventions regarding self.
Initially, it is helpful to 'Undermine Attachment to a Conceptualized Self'. Clients may vary in readiness to work on this area. The timeless struggle between content and context is presenting itself here. ACT promotes the idea that the problem may lie in attachment to beliefs, rather than in the beliefs themselves. This may be seen as a reversal of some views in which self-conceptualization and performance are linked. The 'Mental Polarity Exercise' can be used here to demonstrate the effects of attachment to evaluative thoughts. The description of the exercise also describes the etymology of the word 'perfect'. This is also a powerful and important point, that, in my view is worthy of detailed attention.
Next we have a section on 'Building Awareness of the Observing Self', that aims to help the client notice the process of consciousness and sense of perspective. A 'central ACT intervention', the Chessboard Metaphor, is then described in detail, and a helpful brief therapist/client transcript provided. The Chessboard metaphor can be physically acted out in therapy. Issues such as willingness can be demonstrated through observing how little effort it takes for the board to hold the pieces. An important phrase - " The point is that thoughts, feelings, sensations, memories etc are pieces on the board, they are not you" (p.192).
A couple of notes from a beginner: As p.189 notes, 'therapists and clients are in this language stew together'. It is therefore as important for therapists to work on attachment to their own conceptualized self(-ves), as for the client (a theme of the book). I especially like the brief paragraph on perfect (p.190). In this sense, who is not 'thoroughly made'? This perspective may also carry over to the judgments and evaluations we make of others.
The Chessboard Metaphor is very useful - although I have had one or two clients wanting to sweep all of the pieces from the board (wipe the slate clean). John Billing gave us alternative metaphor on 16.06.04 (or 06.16.04, depending on which side of the pond you're on)
ACT Book Summary: Pages 192 - 198
ACT Book Summary: Pages 192 - 198ACT Book Summary: Pages 198 - 203
ACT Book Summary: Pages 198 - 203ACT Book Summary: Pages 205 - 212
ACT Book Summary: Pages 205 - 212ACT Book Summary: Pages 212 - 219
ACT Book Summary: Pages 212 - 219ACT Book Summary: Pages 219 - 229
ACT Book Summary: Pages 219 - 229These pages concern how to differentiate goals from values, methods to clarify values, ways to elicit actions related to values and how to evaluate barriers to valued action.
Outcome is the Process through which Process Becomes the Outcome
This section relates how needing to attain goals creates motivation and direction for action, but does not provide vitality in life. Attaining goals does not equal happiness or life satisfaction, as one is forced to live in a constant state of deprivation (interestingly, it is pointed out that the etymology of the word "want" is "missing").
The Gardening Metaphor describes how to stick it out with an initial choice (i.e., value) to see what happens (without believing that the "grass is greener on the other side," no pun intended). Another "goal" in this phase of therapy is to help clients see that the process of living equals the outcome of interest. The Skiing Metaphor describes this well. Your stated "goal" may be to get down to the lodge and you are planning to ski there. If someone whisks you off in a helicopter to bring you to the lodge, that would make you mad. It is the process of getting to the lodge (i.e., skiing) that is what is to be enjoyed.
Finally, process cannot be measured from moment to moment like goals. If one continually monitors progress toward specific goals, they may miss the " big picture" (i.e., what they have accomplished to date). Here the Path up the Mountain Metaphor comes into play. It highlights what is wrong with monitoring only "snapshots" of life. If you are hiking up a mountain, you may notice twists and turns, circling around (perhaps even going down the path in parts) ultimately to get up the mountain. You may think at any given time: "I'm doing well" (for instance on an up-path) or conversely: "I'm doing poorly" (on a down-path). Yet, an observer with binoculars across the way (looking down at the hikers) may notice steady, continuous progress toward the overall goal.
Values Clarification: Setting the Compass Heading
In this section, values work is further elaborated. The authors point out that doing values work can be an intimate experience between therapist and client, as oftentimes values are not something the client has ever articulate before to someone else. One of the "values" of "values work" is in the fact that values may help point out to clients what IS working in their lives (i.e., they may be leading valued lives in certain areas they hadn't even recognized). There are some values worksheets on page 224. There are three forms, including a values narrative form, values assessment rating form, and goals, actions, barriers form you can use with clients. The goal is to review the worksheets together and build on them. Values work may be a helpful assessment tool as well. In doing the values work, therapists can uncover possible "ulterior motives" for certain values. The authors give three examples:
- when values statements are controlled by the presence of the therapist, the consequence can be therapist approval or lack of disapproval.
- when values statements are controlled the presence of the culture more generally, the consequence can be the absence of cultural sanctions, broad social approval, or prestige.
- when values statements are controlled by stated or assumed values of the client's parents, the consequence can be parental approval
This is not to say that these factors don't affect EVERYONE'S values, but the extent to which the client takes ownership of their values is important to assess. When a client is wedded to the consequences mentioned above, the therapist can ask the client what would happen if the stated consequences were not there (i.e., "What if your parents did not know you received a Ph.D.?"). Another point the authors make is that it is not uncommon for values to change in valence over the course of therapy. Sometimes (oftentimes) clients may leave certain (or many) domains completely empty. In this situation it can be helpful for the therapist to ask the client what values he/she held earlier in life.
Assessing Goals and Actions
After values work is underway, the focus is on developing goals and specifying the actions that can be taken to achieve those goals. A goal is define as a specific achievement, accomplished in the service of a particular value. Clients do homework in acting according to values either as a one-time deal or from a commitment to repeated and regular acts in the service of a given value. The therapist and client monitor for a close connection between action, goal, and value and try to "accumulate small positives." The authors assert that little steps consistently taken are more useful than heroic steps taken inconsistently. What to do about barriers? The authors mention that engaging in valued action almost always provokes a psychological reaction (often in the form of barriers). At these times, clients may get stuck because they avoid taking values actions as a means of avoiding painful emotional barriers. The therapist then helps the client examine:
- the type of barrier
- ask if the barrier is something they can make room for and still act
- find out what aspect of the barrier may actually help reducing your willingness to have it without defense
- assess whether barriers are a form of emotional control or avoidance
Question
Although I am a big proponent of values work (or I wouldn't be doing this therapy), I am still struck by the similarity of values homework to "monitoring progress toward a goal," not noticing the process itself. In other words, the question "How well did you move toward this goal this week by these actions" seems like the very "snapshot" that is proposed as problematic in the initial part of this section. Any reactions?
ACT Book Summary: Pages 229 - 234
ACT Book Summary: Pages 229 - 234Willingness to have barriers and barriers to willingness: willingness is a value-based action, a choice: see the "Bubble in the road" metaphor p. 230. Therapeutic do's and don'ts:
- coercive use of choice: conflicts are possible between the therapist's and the client's values. Take care not to use "choice" as a way to blame the client.
- confusing values and goals: "I want to be happy" is not a value. It's no direction. It's something you can have or not have, like an object. Values cannot be achieved and maintained. Helping question: "What would you be able to do if that was accomplished?" Values are no means to an end.
ACT Book Summary: Pages 235 - 238
ACT Book Summary: Pages 235 - 238ACT Book Summary: Pages 238 - 244
ACT Book Summary: Pages 238 - 244ACT Book Summary: Pages 244 - 249
ACT Book Summary: Pages 244 - 249ACT Book Summary: Pages 249 - 254
ACT Book Summary: Pages 249 - 254Primary barriers to committed action:
When a client resists committed action, often the client is struggling with how the action will alter his (or her) personal history; how the client has created in his own mind his place in his world. The client may also be grappling with the impact this history has had on his conceptualized self. The client has constructed a self perception of who he is. If he has been subjected to an abusive or otherwise harmful environment, his self perception embraces how he has been victimized by others.
Not surprisingly, the client is threatened with the possibility of positive change. This threat challenges both the client's self perception and the hope that an abuser may someday validate the client's self perception and make amends. For example, a client was physically abused as a child. He now perceives himself as a victim of physical abuse; the perception is intertwined with his identity. If he makes positive change, he may no longer appear as a victim to himself or his abuser. He loses his self perceived identity (as a victim).
Clients with history of painful events (especially in childhood) may have learned that life can be unpredictable and punitive. By limiting their exposure to painful thoughts, they mistakenly believe they can curb their sense of trauma. The opposite is often true. Psychological pain hurts but does not damage; whereas psychological trauma is pain without the willingness to experience the pain. This unwilling causes damage; the effect of the pain persist.
An exercise to teach the difference between psychological pain and trauma:
- Ask the client to describe past painful and traumatic events in detail.
- distinguish between the original pain and,
- the client's reaction to the events.
2. Inventory the area of responses (i.e. physical reactions, emotional reactions, memories, thoughts, etc.)
3. Note the sense of trauma
4. As the client becomes aware of the reaction, ask the client to let go of the struggle with the reaction.
The client's willingness will shift the context of the events; this change will often reduce the client's tension related to the event. As a consequence, the client will be begin to distinguish between trauma and pain. The pain will remain; the trauma will disappear; positive change may occur. A client's reluctance and resistance can be expected. If so, the clinician should:
- point out to the client the burdened caused by resisting the avoided content
- have the client notice physical, emotional and cognitive responses that attach to the unwillingness
- prompt the client to let go of the struggle with unwillingness and be willing to be unwilling
- if the client is able to do this, ask the client to notice the difference between struggle and letting go
- encourage the client to continue the process of letting go and bringing up avoided material.
Things to remember:
- The therapist must identify the functional connection between failing to be "right" about being a victim and remaining a victim who demands redress.
- If the client believes he must remain "broken" in order to prove someone else wrong, the client is stuck, not broken.
- Intervention is delicate.
- The events in question are not being disputed.
- What is being disputed is the necessity of living in a self defeating life in the service of waiting for the recognition and redress that seldom, if ever, comes.
ACT Book Summary: Pages 254 - 259
ACT Book Summary: Pages 254 - 259ACT Book Summary: Pages 259 - 264
ACT Book Summary: Pages 259 - 264ACT Book Summary: Pages 267 - 271
ACT Book Summary: Pages 267 - 271ACT Book Summary: Pages 271 -275
ACT Book Summary: Pages 271 -275ACT Book Summary: Pages 275 - 288
ACT Book Summary: Pages 275 - 288- some useful rules are given (esp. for beginners): no more than 20% explanation, back to exercise, ...
- excessive focus on emotional processing: I was exactly doing this the very moment I read this piece. Back to values and behavior!
- remaining questions: what about clients not seeking help, but needing it (involuntary treatment); how to integrate RFT with other problems (not having to do with avoidance): impulsivity, aggression, ...
Book Translations (Archives)
Book Translations (Archives) CommunityTranslated ACT and RFT Books
Translated ACT and RFT BooksThis list is no longer being updated. Please click here for a list of ACT Books in 20+ Languages.
Translated ACT Books Organized by Language Community
(see below for list by English title)
- Chinese
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Chinese translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2016). 接纳承诺疗法(ACT)--正念改变之道 (Translators: Zhu Zhuzhuohong, Zhang Qi). Bejing: 知识产权出版社 (Intellectual Property Press).
- Hayes, S. C., & Lillis, J. (2012). Acceptance and Commitment Therapy. Washington, DC: American Psychological Association.
- Chinese translation: Hayes, S. C., & Lillis, J. (2016). 接纳承诺疗法(ACT). Translators: Zhu zhuohong, Cao Jing, & Wang Shujuan. Chongqing: 重庆大学出版社 (Chongqing University Press)
- Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004) (Eds.). Mindfulness and acceptance: Expanding the cognitive behavioral tradition. New York: Guilford Press.
- Chinese translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2005.) Mindfulness and acceptance: Expanding the cognitive behavioral tradition. Shanghi: Ewen Publishers. [2011]
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Chinese translation: 羅斯.哈里斯(2009)。快樂是一種陷阱。台北:張老師文化。
- Bach, P., & Moran, D. (2008). ACT in practice: Case conceptualization in Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Chinese translation: 帕特里夏·A.巴赫(Patricia A.Bach)、(美國)丹尼爾·J.莫蘭(2011)。接受與實現療法:理論與實務。重慶:重慶大學出版社。
- John P. Forsyth, & Georg H. Eifert. (2008). The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Chinese translation: 約翰.福賽思(John.P.Forsyth)、格奧爾格.艾弗特(Georg H.Eifert)(2010)。晚安,我的不安:緩解焦慮自助手冊。四川:四川人民出版社。
- Patricia J. Robinson, & Kirk D. Strosahl. (2008). The Mindfulness and Acceptance Workbook for Depression. Oakland, CA: New Harbinger.
- Chinese translation: 科尔克.斯特尔萨拉,派翠西娅.罗宾逊(2010)。抑郁的自我疗法:用接受与实现疗法走出抑郁。华东:华东师范大学出版社。
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Chinese translation: Hayes, S. C., & Smith, S. (2010). Zǒuchū nǐ de tàidù, zài nǐ de shēnghuó: Xīn Acceptance and Commitment Therapy. Chongqing, China: Chongqing University Press.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Danish
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Danish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2013). Acceptance en Commitment Therapy: Psykologisk fleksibilitet og mindfulnessprocessor (2nd edition). Translator: Bjorn Nake. Copenhagen, Denmark: Hans Reitzel Publishers).
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Danish translation: Hayes, S. C., & Smith, S. (2008). Slip tanketyrraniet – tag fat på livet. (Trans. T. Bøgeskov). Copenhagen: Dansk Psykologisk Forlag.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Dutch
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Dutch translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance en Commitment Therapie: Veranderingen door mindfulness, het process en de praktijk. (2nd edition). Amsterdam: Pearson Education Publishers.
- Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- Dutch translation: Luoma, J., Hayes, S. C., & Walser, R. (2009). Leer ACT. Vaardigheden voor therapeuten (Trans. L. Berkhuizen, P. van der Kaaij, & J. A-Tjak). Houten, The Netherlands: Bohn Stafleu van Loghum.
- Hayes, S. C., Strosahl, K. & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
- Dutch translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2006). ACT. Een experiëntiële weg naar gedragsverandering. Nederlandse bewerking (trans. By Ando Rokx). ISBN 90 265 1758 0 Verschijnt zomer 2006 Prijs: C.a. € 50, -
- Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004) (Eds.). Mindfulness and acceptance: Expanding the cognitive behavioral tradition. New York: Guilford Press.
- Dutch translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2006). Mindfullnes en acceptatie. De derde generatie gedragstherapie . (Trans. By Ando Rokx). Nederlandse bewerking. ISBN 90 265 1759 9 Verschijnt zomer 2006 Prijs: C.a. € 50, -
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Dutch translation: Hayes, S. C., Smith, S. (2006). Uit je hoofd, in het leven. Een werkboek voor een waardevol leven met mindfulness en Acceptatie en Commitment Therapie. (Trans. A. Rokx). Amsterdam: Uitgeverij Nieuwezijds.
- Eifert, G. H., McKay, M., & Forsyth, J. P. (2006). Act on life not on anger: The new Acceptance and Commitment Therapy guide to problem anger. Oakland, CA: New Harbinger.
- Dutch translation: Eifert, G. H., Forsyth, J., & McKay, M. (2006). Boosheid de bass: ACT: een nieuwe methode om ergernis en frustratie in de hand te houden. The Netherlands: Thema.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Dutch translation: (2010): De valstrik van het geluk. Bohn Stafleu van Loghum.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Finnish
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Finnish translation: Hayes, S. C., & Smith, S. (2008). Vapaudu mielesi vallasta ja ala elää. (Trans. Päivi and Raimo Lappalainen). Tampere, Finland: Suomen Käyttäytymistieteellinen.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- French
- Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2016). The essential guide to the ACT matrix: A step-by-step approach to Using the ACT matrix model in clinical practice. Oakland, CA: New Harbinger Publications.
- French translation: Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2017) Guide de la matrice ACT. De Boeck Sup.
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- French translation: Villatte, M., Villatte, J., & Hayes, S. C. (2019). Maîtriser la conversation clinique: Le langage en therapie. Malakoff: Dunod Editeur.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- French translation (2009): Le piège du bonheur. Montréal : Éditions de l’Homme.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- French translations: Hayes, S. C., & Smith, S. (2013). Penser moins pour etre heureux: Ici et maintenant, accepter so passé, ses peurs et sa tristesse. Paris, France: Groupe Eyrolles.
- Hayes, S. C., & Smith, S. (2019). Penser moins pour etre heureux: Vicure pleinement, ici et mainenant. Paris, France: Editions Eyrolles.
- Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2016). The essential guide to the ACT matrix: A step-by-step approach to Using the ACT matrix model in clinical practice. Oakland, CA: New Harbinger Publications.
- German
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- German translation: Hayes, S. C. (2020). Kurswechsel im Kopf: Von der Kunst anzunehmen, was ist, und innerlich frei zu werden. Beltz Verlag
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- German translation: Villatte, M., Villatte, J., & Hayes, S. C. (2020). Beherrschung der klinischen Konversation: Sprache als Intervention. Stuttgart: W. Kohlhammer GmbH.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- German translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Akzeptanz & Commitment Therapie: Achtsamkeitsbasierte Veranderungen in Theorie und Praxis (2nd edition). Paderborn, Germany: Junfermann Verlag
- Greco, L., & Hayes, S. C. (Eds.). (2008). Acceptance and mindfulness treatments for children and adolescents: A practitioner’s guide. Oakland, CA: New Harbinger.
- German translation: Greco, L., & Hayes, S. C. (Eds.). (2011). Akzeptanz und achtsamkeit in der kinder - und jugendlichenpsychotherapie. Wienheim, Germany: Beltz Verlag.
- Hayes, S. C., Strosahl, K. & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
- German translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2004). Akzeptanz- und Commitment-Therapie: Ein erlebnisorientierter Ansatz zur Verhaltensänderung. München: CIP-Medien. (transl. by Rainer F. Sonntag & Danielle Tittelbach)
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- German translation: Hayes, S. C., & Smith, S. (2007). In abstand zur inneren wortmaschine: Ein selbsthilfe- und therapiebegleitbuch aud der grundlage der Akzeptanz- und Commitment-Therapie. (Trans. G. Kluger). Tübingen, Germany: dgvt-Verlag.
- Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- German translation (2009): ACT-Training. Reihe Fachbuch, ACT für die klinische Praxis; Acceptance & Commitment Therapie: ein Handbuch. Ein Lernprogramm in zehn Schritten. Translators:Theo Kierdorf, Hildegard Höhr. (ISBN: 978-3-873877-00-9).
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Hebrew
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Hebrew translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). תרפיית קבלה ומחויבות: תהליך ועבודה מעשית ליצירת שינוי קשוב (2nd edition). Haifa, Israel: Ach Publishers.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Italian
- Luoma, J., Hayes, S. C., & Walser, R. (2017). Learning ACT: An Acceptance & Commitment Therapy skills-training manual for therapists (2nd ed). Oakland, CA: Context Press / New Harbinger Publications.
- Italian translation: Luoma, J., Hayes, S. C., & Walser, R. (2019). Il manuale del terapeuta ACT: Apprendere e allenare le abilita dell’ Acceptance & Commitment Therapy (2nd ed). Rome, Italy: Giovanni Fioriti Editore.
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Italian translation: Villatte, M., Villatte, J., & Hayes, S. C. (2020). Il dialogo clinic: Funzione, valore e centralita del linguaggio in psicoterapia. Milan: Franco Angeli.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Italian translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2013). Teoria e pratica del l'Acceptance and Commitment Therapy. (2nd edition). Translation edited by Cesare Maffei. Translators: Nidia Morra and Nicolò Gaj. Milan, Italy: Rafaello Cortina Editore.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Italian translation (2010): Hayes, S. C., & Smith, S. (2010). Smetti di Soffrire, Inizia a Vivere. (ed. IT P. Moderato trans. ACT-Italia) Milano: Franco-Angeli. Visit the ACT-Italia site for information on how to purchase this book. Translators: Ilaria Balasini, Sara Borelli, Katia Covati Katia Manduchi, Giovambattista Presti, Anna Bianca Prevedini, Elisa Rabitti, Massimo Ronchei, Francesca Scaglia, Giovanni Zucchi, Silverio Zucchi, Giovanni Miselli.
- Luoma, J., Hayes, S. C., & Walser, R. (2017). Learning ACT: An Acceptance & Commitment Therapy skills-training manual for therapists (2nd ed). Oakland, CA: Context Press / New Harbinger Publications.
- Japanese
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Japanese translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Juyō to komittomentoserapī. Suginami City, Japan: Seiwa Shoten.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Japanese translation:幸福になりたいなら幸福になろうとしてはいけない: マインドフルネスから生まれた心理療法ACT入門 (単行本) (Japanese) Tankobon Hardcover – December 17, 2015
- Greco, L., & Hayes, S. C. (Eds.). (2008). Acceptance and mindfulness treatments for children and adolescents: A practitioner’s guide. Oakland, CA: New Harbinger.
- Japanese translation: Greco, L., & Hayes, S. C. (Eds.). (2013). Shōni oyobi seinen no tame no ukeire to maindofurunesu ryōhō: jitsumu sha no tame no gaido (Translation Supervisor: T. Muto). Tokyo, Japan: Akashi Shoten.
- Bach, P., & Moran, D. (2008). ACT in practice: Case conceptualization in Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Japanese translation (2009): ACT wo jissenn-suru. (Trans. T. Muto, M. Yoshioka, K. Ishikawa, & A. Kumano) Tokyo: Seiwa-shoten. www.seiwa-pb.co.jp/
- Ramnero, J., & Torneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: Context Press / New Harbinger.
- Japanese translation (2009): Rinshou-koudou-bunnseki no ABC. (Trans. T. Muto, N. Yoneyama, & J. Tanaka-Matsumi) Tokyo: Nihon-Hyoron-sha. www.nippyo.co.jp
- Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- Japanese translation (2009): ACT wo manabu. (Trans. H. Kumano, F. Takahashi, & T. Muto) Tokyo: Seiwa-shoten. www.seiwa-pb.co.jp
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Japanese translation (2008): Anata no Jinsei wo Hajimeru tameno Workbook: Kokoro tono Atarashii Tsukiai kata, Acceptance and Commitment (Trans. T. Muto, H. Harai, M. Yoshioka, & M. Okajima). Tokyo: Brain Shuppan.
- Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004) (Eds.). Mindfulness and acceptance: Expanding the cognitive behavioral tradition. New York: Guilford Press.
- Japanese translation (2005): Maindofurunesu ando akuseputansu; Ninchikodo-ryoho no shinjigen. (Trans. by Y. Haruki, T. Muto, Y. Ito, & Y. Sugiura). Tokyo: Brain-shuppan.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Korean
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Korean translation: Villatte, M., Villatte, J., & Hayes, S. C. (in press). Imsang daehwa maseuteohagi : Gaeib-euloseoui eon-eo. Seoul: Life and Knowledge Publishing
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Korean translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2018). Acceptance and Commitment Therapy: The process and practice of mindful change. Soule, Korea: Sigma Press.
- Greco, L., & Hayes, S. C. (Eds.). (2008). Acceptance and mindfulness treatments for children and adolescents: A practitioner’s guide. Oakland, CA: New Harbinger.
- Korean translation: Greco, L., & Hayes, S. C. (Eds.). (2012). Eo-ri-ni-wa cheong-so-nyeo-neu-rwi-han su-yong mit mindfulness teu-ri-teu. Soule, Korea: Sigma Press.
- Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- Korean translation: Luoma, J., Hayes, S. C., & Walser, R. (2012). Bae-u-gi ACT. Soule, Korea: Hakjisa Publishers.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Korean translation: Hayes, S. C., & Smith, S. (2010). 마음에서 빠져나와 삶 속으로 들어가라 새 수용전념치료. Seoul: Hakjisa Publishers.
- Hayes, S. C., Strosahl, K. & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
- Korean translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2009). 수용과 참여의 심리치료. Sigmapress (translated by Moon, S-W & Kim, E.). Click here to buy this book.
- Hayes, S. C., & Strosahl, K. D. (2004) (Eds.). A practical guide to Acceptance and Commitment Therapy. New York: Springer-Verlag.
- There is a Korean translation in press from Hakjisa Publisher
- McCurry, C. (2011). Parenting your anxious child with mindfulness. Oakland, CA: New Harbinger.
- Korean translation: McCurry, C. (2011). 불안한 아이 수용과 마음챙김으로 키우기. Sigmapress (translated by Lee, S.).
- Forsyth, J. P. & Eifert, G. H. (2008). The Mindfulness and Acceptance Workbook for Anxiety Workbook: A guide to breaking free from anxiety, phobias, & worry using Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Korean translation: Forsyth, J. P. & Eifert, G. H. (2008). 마음챙김과 수용중심 불안장애 치료의 실제. Sigmapress (translated by Lee, S., Han, H., Jung, E.).
- Törneke, N. (2010). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Reno, NV: Context Press.
- Korean translation: Törneke, N. (2019). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Hakjisa (translated by Lee, S.).
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Norwegian
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Norwegian Translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2018) Aksept og verdibasert adferdsterapi (ACT) Mindfull endring - prosess og praksis. Oslo: Arneberg Forlag.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Norwegian translation: Hayes, S. C., & Smith, S. (2015). Slutt å gruble begynn å leve. Oslo: Arneberg Forlag.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Persian
- Vowles, K. E., & Sorrell, J. T. (2008). Life with chronic pain: an acceptance-based approach (therapist guide and patient workbook).
- Persian translation: Vowles, K. E., & Sorrell, J. T. (2008). زندگی با درد مزمن: رویکرد مبتنی بر پذیرش. zendegi ba darde mozmen: roykarde mobtani bar paziresh (rahnamaye darmangar va ketabe kare bimar). translated by F. Mesgarian. Tehran: Arjmand.
- Vowles, K. E., & Sorrell, J. T. (2008). Life with chronic pain: an acceptance-based approach (therapist guide and patient workbook).
- Polish
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Polish translation: Hayes S. C. (2020). Umysł Wyzwolony. Zakończ wewnętrzną walkę i żyj w zgodzie ze sobą. Sopot: Gdańskie Wydawnictwo Psychologiczne.
- Hayes, L. L., & Ciarrochi, J. (2015). The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection. Oakland, CA: New Harbinger.
- Polish translation: Hayes, L., Ciarrochi, J. (2019). TRUDNY CZAS DOJRZEWANIA. Jak pomóc nastolatkom radzić sobie z emocjami, osiągać cele i budować więzi, stosując terapię akceptacji i zaangażowania oraz psychologię pozytywną. Gdańsk: GWP.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Polish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2015). Terapia akceptacji i zaangażowania (2nd edition). Krakow, Poland: Jagiellonian University Press.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Polish translation: Hayes, S. C., & Smith, S. (2014). W pulapce mysli: Jak skutecznie poradzic sobie z depresja, stresem I lekiem. Gdansk: Gdanskie Wydawnictwo Psychologizne.
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Portuguese
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Portuguese translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2021). Terapia de aceitacao e compromisso: a processo e a practica da mundanca consciente (2a editcao). Translation edited by Sandra Maria Mallmann da Rosa. Porto Alegre, Brazil: Artmed.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Romanian
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Romanian translation: Hayes, S. C., & Smith, S. (2013). Ieși din scenariile minții și trăiește-ți viața. (Trans. K. Szabo). Lași, Romania: Editura Poliram.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Russian
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Russian translation: Hayes S. C. (2021). Освобождённый разум. Moscow: Бомбора (Bombora).
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Serbian / Bosnian / Croatian / Montenegrin
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Serbian / Bosnian / Croatian / Montenegrin translation: Hayes, S. C., & Smith, S. (2017). Centar za Kongnitivno-Bohejvioralnu Terapiju. Banja Luka, Bosnia Hercegovina: My Books / Centar za kognitivno-bihejvioralnu terapiju.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Spanish
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Spanish translation: Villatte, M., Villatte, J., & Hayes, S. C. (2019). Gerente la conversación clínica: El lenguaje como intervención. Madrid: Madrid Institute of Contextual Psychology.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Spanish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Terapia de aceptacion y compromise: Proceso y practica del cambio (2nd edition). Translation edited by Ramiro Alvarez. Bilbao, Spain: Desclee de Brouwer.
- Twohig, M., & Hayes, S. C. (2008). ACT verbatim: Depression and Anxiety. Oakland, CA: New Harbinger; Reno, NV: Context Press.
- Spanish translation: Twohig, M., & Hayes, S. C. (2019). ACT en la practica clinica para le depression y la ansiedad. Bilbao, Spain: Desclee de Brouwer.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Spanish translation (2008): Las Trampas De La Felicidad. Grupo Editorial Patria.
- Harris, R. (2011). The Confidence Gap. Boston, MA: Trumpeter.
- Spanish translation (2012): Cuestión de Confianza. Santander. Sal Terrae.
- Hayes, S.C. (2005). Get Out of Your Mind and Into Your Life. Oakland, CA: New Harbinger Publications.
- Spanish translation (May 2013): Sal de tu mente, entra en tu vida. Bilbao. Desclée de Brouwer.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Spanish translation (2014) Terapia de aceptacion y compromise: Proceso y practica del cambio (2nd edition). Translation edited by Ramiro Alvarez. Bilbao, Spain: Desclee de Brouwer.
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Swedish
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Swedish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). ACT – Acceptance and Commitment Therapy i teori och tillamping: Vagen till psykologisk flexibilitet (2nd edition). Stockholm, Sweden: Natur Och Kulture.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Swedish translation: Hayes, S. C., & Smith, S. (2007). Sluta grubbla Borja leva. (Trans. A. Ghaderi). Stockholm: Natur och Kultur.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Swedish translation: (2009): Lykofallan. Stockholm, Sweden.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
Translated ACT Books by English Title
Translations of Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- German Translation: Hayes, S. C. (2020). Kurswechsel im Kopf: Von der Kunst anzunehmen, was ist, und innerlich frei zu werden. Beltz Verlag.
- Polish Translation: Hayes S. C. (2020). Umysł Wyzwolony. Zakończ wewnętrzną walkę i żyj w zgodzie ze sobą. Sopot: Gdańskie Wydawnictwo Psychologiczne.
- Russian Translation: Hayes S. C. (2021). Освобождённый разум. Moscow: Бомбора (Bombora).
Translations of Luoma, J., Hayes, S. C., & Walser, R. (2017). Learning ACT: An Acceptance & Commitment Therapy skills-training manual for therapists (2nd ed). Oakland, CA: Context Press / New Harbinger Publications.
- Italian translation: Luoma, J., Hayes, S. C., & Walser, R. (2019). Il manuale del terapeuta ACT: Apprendere e allenare le abilita dell’ Acceptance & Commitment Therapy (2nd ed). Rome, Italy: Giovanni Fioriti Editore.
Translations of Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2016). The essential guide to the ACT matrix: A step-by-step approach to Using the ACT matrix model in clinical practice. Oakland, CA: New Harbinger Publications.
- French translation: Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2017) Guide de la matrice ACT. De Boeck Sup.
Translations Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- French translation: Villatte, M., Villatte, J., & Hayes, S. C. (2019). Maîtriser la conversation clinique: Le langage en therapie. Malakoff: Dunod Editeur.
- German translation: Villatte, M., Villatte, J., & Hayes, S. C. (2020). Beherrschung der klinischen Konversation: Sprache als Intervention. Stuttgart: W. Kohlhammer GmbH.
- Italian translation: Villatte, M., Villatte, J., & Hayes, S. C. (2020). Il dialogo clinic: Funzione, valore e centralita del linguaggio in psicoterapia. Milan: Franco Angeli.
- Korean translation: Villatte, M., Villatte, J., & Hayes, S. C. (in press). Imsang daehwa maseuteohagi : Gaeib-euloseoui eon-eo. Seoul: Life and Knowledge Publishing.
- Spanish translation: Villatte, M., Villatte, J., & Hayes, S. C. (2019). Gerente la conversación clínica: El lenguaje como intervención. Madrid: Madrid Institute of Contextual Psychology.
Translations of Hayes, L. L., & Ciarrochi, J. (2015). The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection. Oakland, CA: New Harbinger.
- Polish translation: Hayes, L., Ciarrochi, J. (2019). TRUDNY CZAS DOJRZEWANIA. Jak pomóc nastolatkom radzić sobie z emocjami, osiągać cele i budować więzi, stosując terapię akceptacji i zaangażowania oraz psychologię pozytywną. Gdańsk: GWP.
Translations of Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance and Commitment Therapy: The process and practice of mindful change (2nd edition). New York: Guilford Press.
- Dutch translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance en Commitment Therapie: Veranderingen door mindfulness, het process en de praktijk. (2nd edition). Amsterdam: Pearson Education Publishers.
- Danish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2013). Acceptance en Commitment Therapy: Psykologisk fleksibilitet og mindfulnessprocessor (2nd edition). Translator: Bjorn Nake. Copenhagen, Denmark: Hans Reitzel Publishers).
- Italian translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2013). Teoria e pratica del l'Acceptance and Commitment Therapy. (2nd edition). Translation edited by Cesare Maffei. Translators: Nidia Morra and Nicolò Gaj. Milan, Italy: Rafaello Cortina Editore.
- Spanish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Terapia de aceptacion y compromise: Proceso y practica del cambio (2nd edition). Translation edited by Ramiro Alvarez. Bilbao, Spain: Desclee de Brouwer.
- Swedish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). ACT – Acceptance and Commitment Therapy i teori och tillamping: Vagen till psykologisk flexibilitet (2nd edition). Stockholm, Sweden: Natur Och Kulture.
- German translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Akzeptanz & Commitment Therapie: Achtsamkeitsbasierte Veranderungen in Theorie und Praxis (2nd edition). Paderborn, Germany: Junfermann Verlag;
- Norwegian translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2018) Aksept og verdibasert adferdsterapi (ACT) Mindfull endring - prosess og praksis. Oslo: Arneberg Forlag.
- Japanese translation: (Suginami City, Japan: Seiwa Shoten
- Chinese translation
- Polish translation: (Krakow, Poland: Jagiellonian University Press)
- Hebrew translation: (Haifa, Israel: Ach Publishers)
- Korean translation: (Soule, Korea: Sigma Press)
- Portuguese translation: (Porto Alegre, Brazil: Artmed)
Translations of Hayes, S. C., Strosahl, K. & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
- German translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2004). Akzeptanz- und Commitment-Therapie: Ein erlebnisorientierter Ansatz zur Verhaltensänderung. München: CIP-Medien. (transl. by Rainer F. Sonntag & Danielle Tittelbach)
- Dutch translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2006). ACT. Een experiëntiële weg naar gedragsverandering. Nederlandse bewerking (trans. By Ando Rokx). ISBN 90 265 1758 0 Verschijnt zomer 2006 Prijs: C.a. € 50, -
- Korean translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2009). 수용과 참여의 심리치료. Sigmapress (translated by Moon, S-W & Kim, E.). Click here to buy this book.
Translations of Hayes, S. C., & Strosahl, K. D. (2004) (Eds.). A practical guide to Acceptance and Commitment Therapy. New York: Springer-Verlag.
- There is a Korean translation in press from Hakjisa Publisher
- Japanese translation (in press). Akashi Shoten Co.
Translations of Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004) (Eds.). Mindfulness and acceptance: Expanding the cognitive behavioral tradition. New York: Guilford Press.
- Dutch translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2006). Mindfullnes en acceptatie. De derde generatie gedragstherapie . (Trans. By Ando Rokx). Nederlandse bewerking. ISBN 90 265 1759 9 Verschijnt zomer 2006 Prijs: C.a. € 50, -
- Japanese translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (2005.) Maindofurunesu ando akuseputansu; Ninchikodo-ryoho no shinjigen. (Trans. by Y. Haruki, T. Muto, Y. Ito, & Y. Sugiura). Tokyo: Brain-shuppan.
- Korean translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2005.) Mindfulness and acceptance: Expanding the cognitive behavioral tradition. Seoul: Meditation Counseling Research Institute. [2009]
- Chinese translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2005.) Mindfulness and acceptance: Expanding the cognitive behavioral tradition. Shanghi: Ewen Publishers. [2011]
Translations of Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger. (Winner of the Association for Behavioral and Cognitive Therapies Self-Help Book of Merit Award, 2010)
- Danish translation: Hayes, S. C., & Smith, S. (2008). Slip tanketyrraniet – tag fat på livet. (Trans. T. Bøgeskov). Copenhagen: Dansk Psykologisk Forlag.
- Dutch translation: Hayes, S. C., Smith, S. (2006). Uit je hoofd, in het leven. Een werkboek voor een waardevol leven met mindfulness en Acceptatie en Commitment Therapie. (Trans. A. Rokx). Amsterdam: Uitgeverij Nieuwezijds.
- Finnish translation: Hayes, S. C., & Smith, S. (2008). Vapaudu mielesi vallasta ja ala elää. (Trans. Päivi and Raimo Lappalainen). Tampere, Finland: Suomen Käyttäytymistieteellinen.
- German translation: Hayes, S. C., & Smith, S. (2007). In abstand zur inneren wortmaschine: Ein selbsthilfe- und therapiebegleitbuch aud der grundlage der Akzeptanz- und Commitment-Therapie. (Trans. G. Kluger). Tübingen, Germany: dgvt-Verlag.
- Italian translation (2010): Hayes, S. C., & Smith, S. (2010). Smetti di Soffrire, Inizia a Vivere. (ed. IT P. Moderato trans. ACT-Italia) Milano: Franco-Angeli. www.act-italia.org
- French translation: Hayes, S. C., & Smith, S. (2013). Penser Moins pour etre heureux: Ici et maintenant, accepter so passé, ses peurs et sa tristesse. Paris, France: Groupe Ayrolles.
- Chinese translation: Hayes, S. C., & Smith, S. (2010). Zǒuchū nǐ de tàidù, zài nǐ de shēnghuó: Xīn Acceptance and Commitment Therapy. Chongqing, China: Chongqing University Press.
- Korean translation: Hayes, S. C., & Smith, S. (2010). 마음에서 빠져나와 삶 속으로 들어가라 새 수용전념치료. Seoul: Hakjisa Publishers.
- Japanese translation: Hayes, S. C., & Smith, S. (2008). Anata no Jinsei wo Hajimeru tameno Workbook: Kokoro tono Atarashii Tsukiai kata, Acceptance and Commitment (Trans. T. Muto, H. Harai, M. Yoshioka, & M. Okajima). Tokyo: Brain Shuppan.
- Second Japanese translation: Hayes, S. C., & Smith, S. (2010). Anata no Jinsei wo Hajimeru tameno Workbook: Kokoro tono Atarashii Tsukiai kata, Acceptance and Commitment (Trans. T. Muto, H. Harai, M. Yoshioka, & M. Okajima). Tokyo: Seiwa Shoten Publishers.
- Swedish translation: Hayes, S. C., & Smith, S. (2007). Sluta grubbla Borja leva. (Trans. A. Ghaderi). Stockholm: Natur och Kultur.
- Romanian translation: Hayes, S. C., & Smith, S. (2013). Ieși din scenariile minții și trăiește-ți viața. (Trans. K. Szabo). Lași, Romania: Editura Poliram.
- Bosnian translation: Hayes, S. C., & Smith, S. (in press). Centar za Kongnitivno-Bohejvioralnu Terapiju.
- Croatian translation: Hayes, S. C., & Smith, S. (in press). Centar za Kongnitivno-Bohejvioralnu Terapiju.
- Montenegrin translation: Hayes, S. C., & Smith, S. (in press). Centar za Kongnitivno-Bohejvioralnu Terapiju.
- Serbian translation: Hayes, S. C., & Smith, S. (in press). Centar za Kongnitivno-Bohejvioralnu Terapiju.
- Polish translation: Hayes, S. C., & Smith, S. (n press). Gdansk: Gdanskie Wydawnictwo Psychologizne.
- Spanish translation: Hayes, S. C., & Smith, S. (2013). Sal de tu mente entra en tu vida: La nueva Terapia de Aceptación y Compromiso. Bilbao, Spain: Editorial Desclée De Brouwer.
- For the visually impaired (or just those who like audio books) there is an Audio book version: New York: Tantor Audio (2012)
Translation of Eifert, G. H., McKay, M., & Forsyth, J. P. (2006). Act on life not on anger: The new Acceptance and Commitment Therapy guide to problem anger. Oakland, CA: New Harbinger.
- Dutch translation: Eifert, G. H., Forsyth, J., & McKay, M. (2006). Boosheid de bass: ACT: een nieuwe methode om ergernis en frustratie in de hand te houden. The Netherlands: Thema.
Translation of Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Spanish translation (2008): Las Trampas De La Felicidad. Grupo Editorial Patria.
- Chinese translation: 羅斯.哈里斯(2009)。快樂是一種陷阱。台北:張老師文化。
- French translation: (2009): Le piège du bonheur. Montréal : Éditions de l’Homme.
- Japanese translation: 幸福になりたいなら幸福になろうとしてはいけない: マインドフルネスから生まれた心理療法ACT入門 (単行本) (Japanese) Tankobon Hardcover – December 17, 2015
- Dutch translation: (2010): De valstrik van het geluk. Bohn Stafleu van Loghum.
- Swedish translation: (2009): Lykofallan. Stockholm, Sweden.
Translation of Harris, R. (2011). The Confidence Gap. Boston, MA: Trumpeter.
- Spanish translation (2012): Cuestión de Confianza. Santander. Sal Terrae.
Translations of Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- German translation (2009): ACT-Training. Reihe Fachbuch, ACT für die klinische Praxis; Acceptance & Commitment Therapie: ein Handbuch. Ein Lernprogramm in zehn Schritten. Translators:Theo Kierdorf, Hildegard Höhr. (ISBN: 978-3-873877-00-9).
- Japanese translation (2009): ACT wo manabu. (Trans. H. Kumano, F. Takahashi, & T. Muto) Tokyo: Seiwa-shoten. www.seiwa-pb.co.jp
- Dutch translation: Luoma, J., Hayes, S. C., & Walser, R. (2009). Leer ACT. Vaardigheden voor therapeuten (Trans. L. Berkhuizen, P. van der Kaaij, & J. A-Tjak). Houten, The Netherlands: Bohn Stafleu van Loghum.
- Korean translation: Luoma, J., Hayes, S. C., & Walser, R. (20012). Bae-u-gi ACT. Soule, Korea: Hakjisa Publishers.
Translations of Bach, P., & Moran, D. (2008). ACT in practice: Case conceptualization in Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Japanese translation (2009): ACT wo jissenn-suru. (Trans. T. Muto, M. Yoshioka, K. Ishikawa, & A. Kumano) Tokyo: Seiwa-shoten. www.seiwa-pb.co.jp
- Chinese translation: 帕特里夏·A.巴赫(Patricia A.Bach)、(美國)丹尼爾·J.莫蘭(2011)。接受與實現療法:理論與實務。重慶:重慶大學出版社
Translation of Ramnero, J., & Torneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: Context Press / New Harbinger.
- Japanese translation (2009): Rinshou-koudou-bunnseki no ABC. (Trans. T. Muto, N. Yoneyama, & J. Tanaka-Matsumi) Tokyo: Nihon-Hyoron-sha. www.nippyo.co.jp
Translations of Hayes, S. C., Barnes-Holmes, D., & Roche, B. (2001). Relational Frame Theory: A Post-Skinnerian account of human language and cognition. New York: Plenum Press.
- Japanese translation: Hayes, S. C., Barnes-Holmes, D., & Roche, B. (2009). Relational Frame Theory: A Post-Skinnerian account of human language and cognition. Tokyo: Seiwa Shoten.
Translation of Forsyth, J. P. & Eifert, G. H. (2008). The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Chinese translation: 約翰.福賽思(John.P.Forsyth)、格奧爾格.艾弗特(Georg H.Eifert)(2010)。晚安,我的不安:緩解焦慮自助手冊。四川:四川人民出版社。
Translation of Robinson, P. J. & Strosahl, K. D. (2008). The Mindfulness and Acceptance Workbook for Depression. Oakland, CA: New Harbinger.
- Chinese translation: 科尔克.斯特尔萨拉,派翠西娅.罗宾逊(2010)。抑郁的自我疗法:用接受与实现疗法走出抑郁。华东:华东师范大学出版社。
Examples of Books on ACT and RFT
Examples of Books on ACT and RFTThis is a partial list as of 2014
General ACT Books: Professionals
Luoma, J., Hayes, S. C. & Walser, R. (2007). Learning ACT. Oakland, CA: New Harbinger. [A step by step learning companion for the main ACT book below. Very practical and helpful]
Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance and Commitment Therapy: The process and practice of mindful change (2nd edition). New York: Guilford Press. [This is still the heart of the ACT literature. It is where it started]
Wilson, K. G. & Dufrene, T. (2009). Mindfulness for two: An Acceptance and Commitment Therapy approach to mindfulness in psychotherapy. Oakland, CA: New Harbinger. [A book on ACT that emphasizes mindfulness and the therapeutic relationship]
Hayes, S. C. & Strosahl, K. D. (2005). A Practical Guide to Acceptance and Commitment Therapy. New York: Springer-Verlag. [Shows how to do ACT with a variety of populations]
Twohig, M., & Hayes, S. C. (2008). ACT verbatim: Depression and Anxiety. Oakland, CA: New Harbinger; Reno, NV: Context Press. [Good example of ACT in actual practice]
Chantry, D. (2007). Talking ACT: Notes and conversations on Acceptance and Commitment Therapy. Reno, NV: Context Press. [This is an edited version of the ACT listserv from July 2002 through August 2005 compiled by a therapist, for therapists. Functions as a quick reference on a wide range of ACT topics (acceptance, anxiety, behavior analysis, choice, clinical resources, contextualism, etc)]
Ciarrochi, J. V. & Bailey, A. (2008). A CBT practitioner’s guide to ACT. Oakland, CA: New Harbinger. [Does what the title says it does]
Batten, S. (2011). Essentials of Acceptance and Commitment Therapy. London: Sage. [Broad introduction to ACT]
Harris, R. (2009). ACT made simple. Oakland, CA: New Harbinger. [Easy place to start with ACT]
Hayes, S. C. & Lillis, J. (2012). Introduction to Acceptance and Commitment Therapy. Washington, DC: American Psychological Association. [Books specifically for students learning about ACT]
General ACT Books: Clients
Hayes, S. C. & Smith, S. (2005). Get out of your mind and into your life. Oakland, CA: New Harbinger. [A general purpose ACT workbook. RCTs show that it works as an aid to ACT or on its own, but it will also keep new ACT therapists well oriented]
Harris, R. (2008). The happiness trap. New York: Shambala. [Very accessible ACT book for the public]
Trauma: Professional book
Walser, R., & Westrup, D. (2007). Acceptance & Commitment Therapy for the Treatment of Post-Traumatic Stress Disorder & Trauma-Related Problems: A Practitioner's Guide to Using Mindfulness & Acceptance Strategies. Oakland, CA: New Harbinger. [A very practical and accessible approach to using ACT to treat post-traumatic stress disorder (PTSD) and acute trauma-related symptoms.]
Trauma: Client book
Follette, V. M., & Pistorello, J. (2007). Finding Life Beyond Trauma: Using Acceptance and Commitment Therapy to Heal from Post-Traumatic Stress and Trauma-Related Problems. Oakland, CA: New Harbinger. [Applies the principles of ACT to help readers cope with the after effects of traumatic experience. Straightforward, practical, and useful]
Depression: Professional book
Zettle, R. (2007). ACT for Depression: A Clinician's Guide to Using Acceptance & Commitment Therapy in Treating Depression. Oakland, CA: New Harbinger. [An solid book from one of the founders of ACT on one of the most pervasive problems human beings face.]
Depression: Client book
Strosahl, K. & Robinson, P. J. (2008). The Mindfulness & Acceptance Workbook for Depression: Using Acceptance & Commitment Therapy to Move Through Depression & Create a Life Worth Living. Oakland: New Harbinger. [Great workbook on ACT for depression]
Anxiety: Professional book
Eifert, G. & Forsyth, J. (2005). Acceptance and Commitment Therapy for anxiety disorders. Oakland: New Harbinger. [Good book with a protocol that shows how to mix ACT processes into a brief therapy for anxiety disorders].
Anxiety: Client book
Forsyth, J., & Eifert, G. (2007). The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy. Oakland: New Harbinger. [Solid workbook for anxiety]
Worry: Client book
Lejeune, C. (2007). The Worry Trap: How to Free Yourself from Worry & Anxiety using Acceptance and Commitment Therapy. Oakland, CA: New Harbinger. [A guide to the application of ACT to worry and generalized anxiety.]
Chronic pain: Professional books
Dahl, J., Wilson, K. G., Luciano, C., & Hayes, S. C. (2005). Acceptance and Commitment Therapy for Chronic Pain. Reno, NV: Context Press. [Describes an ACT approach to chronic pain. Very accessible and readable. One of the better clinical expositions on how to do ACT values work.]
McCracken, L. M. (2005). Contextual Cognitive-Behavioral Therapy for chronic pain. Seattle, WA: International Association for the Study of Pain. [[Describes an interdisciplinary ACT-based approach to chronic pain
Chronic pain: Client book
Dahl, J. C., & Lundgren, T. L. (2006). Living Beyond Your Pain: Using Acceptance and Commitment Therapy to Ease Chronic Pain. Oakland, CA: New Harbinger. [Uses ACT principles to help those suffering from pain transcend the experience by reconnecting with other, more valued aspects of their lives.]
Anger: Client book
Eifert, G. H., McKay, M., & Forsyth, J. P. (2006). ACT on life not on anger: The new Acceptance and Commitment Therapy guide to problem anger. Oakland, CA: New Harbinger. [The first book to adapt ACT principles to dealing with anger. It teaches readers how to change their relationship to anger by accepting rather than resisting angry feelings and learning to make values-based responses to provocation. Has been tested successfully in a small randomized trial.]
Caregivers: Client book
McCurry, S. M. (2006). When a family member has dementia: Steps to becoming a resilient caregiver. Westport, CT: Praeger Publishers. [Although not directly on ACT or mindfulness, this book for caregivers does include a significant emphasis on acceptance, as might make sense given that the author is on of the early ACT therapists from UNR.]
Eating disorders: Client book
Heffner, M., & Eifert, G. H. (2004). The anorexia workbook: How to accept yourself, heal suffering, and reclaim your life. Oakland, CA: New Harbinger. [An eating disorders patient workbook on ACT.]
Diabetes management: Client book
Gregg, J., Callaghan, G., & Hayes, S. C. (2007). The diabetes lifestyle book: Facing your fears and making changes for a long and healthy life. Oakland, CA: New Harbinger. [You cannot tell from the title but this is a book applying ACT to diabetes management.]
Organizational issues: Professional book
Hayes, S. C., Bond, F. W., Barnes-Holmes, D., & Austin, J. (2007). Acceptance and Mindfulness at Work: Applying Acceptance and Commitment Therapy and Relational Frame Theory to Organizational Behavioral Management. Binghamton, NY: Haworth Press. [This was a special issue of the Journal of Organizational Behavior Management that was bound into book form. Don't buy it expecting a smooth presentation of the applicability of ACT and RFT to organizational issues -- it is a collection of journal articles gather into a book. But it is still worthwhile if I/O is your area and you are wondering how ACT and RFT might apply.]
Human performance: Professional book
Gardner, F.L., & Moore, Z.E. (2007). The psychology of enhancing human performance: The Mindfulness-Acceptance-Commitment (MAC) approach. New York: Springer.
[This book provides theory and empirical background, and a structured step-by-step, protocol for the assessment, conceptualization, and enhancement of human performance with a variety of high-performing clientele including executives, athletes, artists, and emergency/military personnel].
Trichotillomania: Professional book
Woods, D. W., & Twohig, M. P. (2008). Trichotillomania: An ACT-enhanced Behavior Therapy Approach Therapist Guide. New York: Oxford University Press.
Trichotillomania: Client book
Woods, D. W., & Twohig, M. P. (2008). Trichotillomania: An ACT-enhanced Behavior Therapy Approach Workbook. New York: Oxford University Press.
Behavioral Medicine: Professional book
McCracken, L. (2011). Mindfulness and Acceptance in Behavioral Medicine. Oakland, CA: New Harbinger.
Assessment: Professional book
Baer, R. (2010). Assessing Mindfulness & Acceptance Processes in Clients: Illuminating the Theory & Practice of Change. Oakland, CA: New Harbinger.
Primary care settings: Professional book
Robinson, P. J., Gould, D. A., & Strosahl, K. D. (2011). Real behavior change in primary care. Oakland, CA: New Harbinger.
Irritable Bowel Syndrome: Client book
Ferreira, N. B. & Gillanders, D. T (2012) Better Living with IBS: A step-by-step program to managing your symptoms so you can enjoy life to the full! Exsile Publishing, New South Wales.
Psychosis: Professional book
Morris, E. M. J., Johns, L. C., & Oliver, J. E. (2013) (Eds). Acceptance and Commitment Therapy and mindfulness for psychosis. London: Wiley-Blackwell. ISBN: 978-1-1199-5079-0
Sleep: Client book
Meadows, G. (2014). The sleep book: How to sleep well every night. London, UK: Orion.
Persian
PersianThis list is no longer being updated. Please click here for a list of ACT Books in 20+ Languages.
Vowles, K. E., & Sorrell, J. T. (2008). Life with chronic pain: an acceptance-based approach (therapist guide and patient workbook).
Persian translation: Vowles, K. E., & Sorrell, J. T. (2008). زندگی با درد مزمن: رویکرد مبتنی بر پذیرش. translated by F. Mesgarian. Tehran: Arjmand.
Original Non-English ACT Books
Original Non-English ACT BooksThis list is no longer being updated. Please click here for a list of ACT Books in 20+ Languages.
Original Non-English ACT Books
- Danish (Dansk)
- Grønlund, C. & Møller Rasmussen, S. (2015). Rundt om ACT : muligheder og metode i acceptance and commitment therapy. Frydenlund.
- This first Danish-written anthology on ACT (Acceptance and Commitment Therapy) goes in depth with the method's many application possibilities - seen through the eyes of Danish therapists.
- Ramussen, S. & Taggaard Nielsen, O. (2010). Introduktion til ACT. Copenhagen: Dansk Psykologisk Forlag.
- Grønlund, C. & Møller Rasmussen, S. (2015). Rundt om ACT : muligheder og metode i acceptance and commitment therapy. Frydenlund.
- Dutch (Nederlandstalig)
- A-Tjak, J., & De Groot, F. (Eds.). (2008) . Acceptance and commitment therapy: Een inleiding voor hulpverleners. Houten: Bohn Stafleu van Loghum. (ISBN 978 90 313 5894 6. NUR 777)
- An original edited volume about ACT.
- Jansen, G. (2006). Denk wat I wilt doe wat I droomt: op weg naar waardevol leven. Amsterdam: Uitgeverij Nieuwezijds.
- An ACT-related book in Dutch. Some discussion between ACT and Cognitive Therapy in this book, but it is not possible to make such discrimination out of a language community. The book definitely puts a number of ACT concepts forward for consideration.
- A-Tjak, J., & De Groot, F. (Eds.). (2008) . Acceptance and commitment therapy: Een inleiding voor hulpverleners. Houten: Bohn Stafleu van Loghum. (ISBN 978 90 313 5894 6. NUR 777)
- Finnish (Suomi)
- Lappalainen, R., Lehtonen, T., Hayes, SC, Batten, S., Gifford, E., Wilson, K.G., Afari, N., & McCurry, S.M. (2004). Hyväksymis- ja omistautumisterapia käytännön terapiatyössä (Applying Acceptance and Commitment Therapy (ACT): A Clinical Manual). Tampere, Finland: Suomen Käyttäytymistieteellinen Tutkimuslaitos (The Finnish Institute for Behavioral Science).
- An ACT clinical manual in Finnish.
- Lappalainen, R., Lehtonen, T., Hayes, SC, Batten, S., Gifford, E., Wilson, K.G., Afari, N., & McCurry, S.M. (2004). Hyväksymis- ja omistautumisterapia käytännön terapiatyössä (Applying Acceptance and Commitment Therapy (ACT): A Clinical Manual). Tampere, Finland: Suomen Käyttäytymistieteellinen Tutkimuslaitos (The Finnish Institute for Behavioral Science).
- French (Français)
- Dionne, F., & Veillette, J. (2021). Apprivoiser la douleur chronique avec ACT: un guide de pratique en 10 modules. Paris, France : Dunod.
- La douleur chronique constitue un enjeu de santé publique important et pose plusieurs défis cliniques et personnels pour le praticien. La thérapie d’acceptation et d’engagement (ACT, Acceptance and Commitment Therapy) propose des stratégies thérapeutiques originales et efficaces pour améliorer la qualité de vie des gens souffrant de cette problématique.
- Son objectif n’est pas de modifier les symptômes, mais de faire évoluer le rapport du patient à leur égard, de la lutte vers l’acceptation active de la douleur, et l’engagement dans des activités en cohérence avec ses valeurs personnelles.
- Monestès, J. L. (2010). Changer grâce à Darwin. La théorie de votre évolution. Paris: Odile Jacob.
- Darwin nous a appris comment l’évolution avait façonné notre espèce. Mais sa théorie peut aussi être utile à chacun d’entre nous au quotidien !
- Cet ouvrage explique comment les mécanismes naturels qui ont fait leur preuve pour l’espèce humaine peuvent aider chacun de nous à évoluer dans sa vie : nous pouvons favoriser une sélection de nos comportements, et ne plus laisser le hasard gérer notre destin.
- Il propose de nombreux outils pratiques fondés sur la thérapie d’acceptation et d’engagement et les thérapies cognitives et comportementales : dépasser les obstacles au changement, créer de la variation, développer sa curiosité au monde, mais aussi, quand il le faut, accepter les choses comme elles viennent, ne rien changer, cesser de vouloir contrôler l’incontrôlable….
- Un « darwinisme personnel » pour faciliter votre propre évolution !
- This book presents a selectionist approach of behaviors. It proposes advice and tools to commit in direction of values and to walk through acceptance, by using concepts from Darwinism and ACT.
- Schoendorff, B. (2009). Faire Face à la Souffrance, Choisir la vie plutôt que la lutte avec la Thérapie d'Acceptation et d'Engagement.
- The first book on ACT in French. It is a bibliotherapy book based in part on the I-view model of Kevin Polk and Jerold Hambright.
- This is the first book on ACT in French. It's a self-help book based on Kevin Polk and Jerold Hambright's I-view.
- Monestès, J. L. (2009). Faire la paix avec son passé. Paris: Odile Jacob.
- Nos souvenirs, particulièrement les plus douloureux, nous incitent à la lutte pour éviter leur réapparition. Ce livre sur la mémoire développe de nombreux concepts de l’ACT et les applique aux souvenirs des événements que nous aurions préféré ne pas vivre.
- It is our natural tendency to struggle when we are confronted to hurting memories. We would prefer to erase them if we could. This book on memory uses ACT concepts to deal with memories of events we would rather not have lived.
- Dionne, F., & Veillette, J. (2021). Apprivoiser la douleur chronique avec ACT: un guide de pratique en 10 modules. Paris, France : Dunod.
- German (Deutsch)
- Wengenroth, M. (2008). Das Leben annehmen. So hile die Akzeptanz- und Commitmenttherapie (ACT). Bern, Germany: Huber.
- An original German, ACT-based self-help book. Very good buzz about this book by ACT experts.
- Wengenroth, M. (2008). Das Leben annehmen. So hile die Akzeptanz- und Commitmenttherapie (ACT). Bern, Germany: Huber.
- Polish (Polish)
- Baran, L., Hyla, M., Kleszcz, B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego.
- Portuguese (Português)
- Saban, M. T. (2015). Introdução à Terapia de Aceitação e Compromisso. Belo Horizonte: Ed. Artesã.
- Lucena-Santos, P., Pinto-Gouveia, J., & Oliveira, MS (Eds.) (2015). Terapias Comportamentais of Terceira Geração: Guia para profissionais. Novo Hamburgo: Sinopsys Editora
- An original book including but not limited to ACT. Specifically, this book is a professional guide on third-wave behavioral therapies (Mindfulness-based Cognitive Therapy, Functional Analytic Psychotherapy, Behavioral Activation Therapy, Behavioral Activation, Mindfulness-Based Stress Reduction and Compassion Focused Therapy)
- Boavista, R. (2012). Terapia of Aceitação e Compromisso (ACT): Purpose uma possibilidade para a clínica comportamental. Santo André: ESETec Editores Associados.
- In this book Rodrigo RC Boavista does a book review that contemplates philosophical assumptions, theoretical foundations, model of psychopathology and a few application scenarios of the ACT therapeutic approach.
- Japanese (日本語)
- Muto, T. (Ed.) (2017). 55歳からのアクセプタンス&コミットメント・セラピー(ACT)超高齢化社会のための認知行動療法の新展開 [Turning 55 years old in super-aging society: Living oldness with Acceptance and Commitment Therapy]. Kyoto: Ratik.
- Kumano, H. & Muto, T. (Eds.) (2009). Tokushuu-gou: Akuseputansu ando komittoment serapi. in the “Kokoro-no-Rinshou a la carte” Magazine for clinicians. Tokyo: Seiwa-shoten.
- Title translation: Special volume: Acceptance and Commitment Therapy.
- Kumano, H. (2009). 21 seiki no jibun sagashi project: kara no ori kara dete, machi ni dekakeyou. Tokyo: Sanga.
- Title translation: The “Pursuit of myself” project in 21 century: Breaking the prison of conceptualized myself.
- Muto, T. (Eds.) (2006). Akuseputansu ando komittoment serapi no bunmyaku: Rinshou-kudu-bunseki no maindofuru-na tenkai. Tokyo: Brain-shuppan.
- Title: Some contexts of Acceptance and Commitment Therapy: Mindfulness in Clinical Behavior Analysis .
- Korean (조선말, 한국어)
- Lee, Seonyoung (2017). 꼭 알고 싶은 수용-전념 치료의 모든 것: ACT와 친해지기. Soulmate. Seoul.
- Spanish (Español)
- García Higuera, JA (2007). Curso Teraperutico de Aceptación I y II. Madrid: Paradox.
- An ACT self help book with lots of exercises.
- Barraca, J. (Ed.). (2005). The mente o la vida. An aproximation to the Terapia of Acceptance and Compromise. Bilbao: Desclée de Brouwer.
- An original edited ACT book in Spanish.
- Wilson, KG, & Luciano, C. (2002). Acceptance and Commitment Therapy: A behavioral treatment focused on values. Madrid: Pirámide.
- An original ACT book in English ACT authors.
- García Higuera, JA (2003). Terapia psicológica en el tartamudeo, from Van Riper to the terapia of acceptance and compromiso.Barcelona: Editorial Ariel. Visit this site web para más información.
- An ACT book dedicated to stuttering and its psychological treatment.
- Luciano, C. (Ed.). (2001). Terapia of Acceptance and Compromise (ACT) and the Traastorno de Evitación Experiencial. A síntesis of casinos clinics. (Ed.) Valencia: Promolibro.
- An original ACT book in Spanish with a series of very creative single case studies.
- García Higuera, JA (2007). Curso Teraperutico de Aceptación I y II. Madrid: Paradox.
Samtaler som forandrer - behandlerens guide til ACT i teori og praksis
Samtaler som forandrer - behandlerens guide til ACT i teori og praksisDrømmer du om at lære de effektive, evidensbaserede og håndgribelige strategier, som skaber vilde og varige forandringer for dine klienter og for dig selv? Samtaler som forandrer er behandlerens guide til ACT i teori og praksis. Bogen er skrevet af Rikke Kjelgaard, en af Danmarks største kapaciteter inden for ACT (Acceptance and Commitment Therapy). Her får du som behandler en grundig introduktion til ACT med masser af kliniske eksempler og øvelser. Du bliver præsenteret for de grundlæggende begreber og for modellens bærende principper. Du får en gennemgang af kerneprocesserne i ACT samt eksempler på, hvordan disse processer udspiller sig i det terapeutiske møde. Du følger med i en række samtaler som netop demonstrerer kerneprocesserne. Du lærer at lave sagskonceptualisering, at skabe fleksibilitetsprofiler, og du lærer, hvordan du designer dine egne metaforer. Du får desuden en række generelle tips til, hvad du skal gøre – og hvad du skal undgå at gøre – for at skabe samtaler, som forandrer.
Self-Help Books in Non-English Languages
Self-Help Books in Non-English LanguagesThis list is no longer being updated. Please click here for a list of ACT Books in 20+ Languages.
Original Non-English Self-Help Books
German
- Waadt, M. (Author),& Acker, J. (2018). Das Selbsthilfebuch gegen Burnout: Mit Akzeptanz und Achtsamkeit den Teufelskreis durchbrechen. Berne, CHE: Hogrefe AG.
- Wengenroth, M. (2008). Das Leben annehmen. So hilft die Akzeptanz- und Commitmenttherapie (ACT). Bern, Germany: Huber.
Danish
- Ramussen, S. & Taggaard Nielsen, O. (2010) Introduktion til ACT. Copenhagen: Dansk Psykologisk Forlag. 2nd printing (2012).
Dutch
- Bohlmeijer, E., & Hulsbergen, M. (2009). Voluit leven. Amsterdam, NLD: Boom.
French
Schoendorff, B. (2009). Faire face à la souffrance, choisir la vie plutôt que la lutte avec la Thérapie d'Acceptation et d'Engagement. Paris: Retz.
Le premier livre sur l'ACT en français. C'est un ouvrage de bibliothérapie qui se base en partie sur le modèle I-view de Kevin Polk et Jerold Hambright.
Portuguese
- Bittar, E. (2011). Nao sou feliz … e agora? O que fazer quando todas as formulas fracassem? Uberlândia, Brazil: Imagine.
Spanish
García Higuera, J. A. (2007).Curso Terapéutico de Aceptación I y II. Madrid: Paradox.
An ACT self help book with 4 audio CDs with lots of exercises.
Other Self Help Books (2006-2009)
Other Self Help Books (2006-2009)OTHER SELF HELP BOOKS
- Kashdan, T. (2009). Curious? Discover the missing ingredient to a fulfilling life. New York, NY: Harper Collins.
- Flowers, S. H. (2009). The Mindful Path Through Shyness: How Mindfulness and Compassion Can Free You From Social Anxiety, Fear, and Avoidance. Oakland, CA: New Harbinger Publications.
- Vieten, C. (2009). Mindful Motherhood: Practical Tools for Staying Sane During Pregnancy and Your Child’s First Year. Oakland, CA: New Harbinger Publications.
- McKay, M., & Sutker, C. (2007). Leave Your Mind Behind. Oakland, CA: New Harbinger.
- McCurry, S. M. (2006). When a family member has dementia: Steps to becoming a resilient caregiver. Westport, CT: Praeger Publishers. - Although not directly on ACT or mindfulness, this book for caregivers does include a significant emphasis on acceptance (the author is one of the early ACT therapists from the University of Nevada, Reno and studied with Steve Hayes).
ACT /RFT Reader's Update 2008 - 2011 (Archives)
ACT /RFT Reader's Update 2008 - 2011 (Archives)The ACT/RFT Reader's Update was published from 2008 - 2011. For up-to-date lists of ACT/RFT publications, go to the ACT Randomized Controlled Trials page, the State of the ACT Evidence page, the list of ACT Books, and the Publications section.
The ACT /RFT Reader's Update is an electronic newsletter provided for your information and perusal. This online newsletter provides summaries of recent, ACT and RFT articles (or related articles) published in peer-reviewed journals. In addition, citations for the latest books, book chapters, and unpublished dissertations will be listed.
Our main aim with this update is to keep the ACT/RFT community informed. We hope to include information that is relevant, scientifically sound, and of interest in the ACT/RFT community. Our purpose is not to recreate the abstract of these articles, but to provide a broader summary of the article. However, are goal is to keep the "busy" reader in mind, and therefore, we will work to keep the summaries brief.
Reviewers include:
Robyn Walser, PhD
Christi Ulmer, PhD
Maggie Chartier, MPH, MS
Ian Stewart, PhD
Miguel Rodríguez Valverde, PhD
ACT/RFT Readers Update 2011
ACT/RFT Readers Update 2011Dear Contextual Science Community,
We are happy to be putting out our full 2011 ACT/RFT Reader’s Update. In this Update we review assessment, chronic pain, experiential avoidance, pilot studies, RCT’s, relational frame theory and several research reviews. We hope you find the information helpful. Please take a look at the attached and find what interests you.
It has been interesting times at the Update, with change in editorial/writer staff (a big welcome to Katherine Young, Jeannette Tappe, Tam Nguyen and Aimee Zhang) and other unanticipated delays with this issue, we have been pressed to finish up and post.
We are also looking forward to including and perhaps featuring articles found in the Journal of Contextual Behavioral Science. We hope everyone is enjoying the journal and finding it useful. What a great contribution to ACBS! http://contextualscience.org/JCBS
Lastly and importantly, we are looking forward to ACBS World Conference in Sydney, Australia, July 8-12. The World Conference is always exciting, engaging and fun! Many great ideas for projects, studies and papers are generated at the conference and it will be sure to provide ACT/RFT Reader’s Update staff with plenty more to review! http://contextualscience.org/wc11
Warm Regards,
Maggie Chartier, Psy.D., MPH
Barbara Mazina, B.A.
Tam Nguyen, Ph.D.
Katie Sears, Ph.D.
Ian Stewart, Ph.D.
Jeannette Tappe, M.A.
Thuy Tran, B.A.
Robyn Walser, Ph.D.
Katherine Young, M.S.
Aimee Zhang, B.S.
ACT/RFT Reader's Update 2010
ACT/RFT Reader's Update 2010Dear ACT Community,
We are excited….and relieved to put out two Reader’s Updates this round. Please log in to download the attachments from this webpage.
It is really great to see all of the work and writing that is being done in the areas of ACT, RFT and mindfulness. It is keeping us busy and energized as reviewers. Find in the Update, summaries designed to provide you with a quick overview of topics and issues, with links in the document to more detailed information.
In Update “10finalb” you will find summaries, references and abstracts on acceptance, addiction, assessment, case studies, children/adolescents, chronic pain, experiential avoidance and RFT.
In Update “10finalcd,” in addition to some of the same topics above, you will find summaries, references and abstracts on anxiety and depression, RCT’s and research reviews. In this issue we also wanted to feature RFT. It is the first summary presented in the Update. Ian Stewart has done an excellent job. He has thoughtfully put together information in a effort to keep us abreast of research this area. A big thanks to Ian!
We are diligently working on the next issue: Coming soon to a list-serve near you!
Finally, if you know of any articles, studies or other information that we should include in our next issue and may not be easily findable by regular search engines, please let us know. Also, be sure to let us know if we missed something.
Enjoy!
Reviewers and Editors
Maggie Chartier
Barbara Mazina
Katie Sears
Ian Stewart
Thuy Tran
Robyn Walser
ACT/RFT Reader's Update: Articles from early 2010 (November, 2011)
ACT/RFT Reader's Update: Articles from early 2010 (November, 2011)Dear Colleagues,
Welcome to this edition of the ACT/RFT Reader’s Update.
In this issue, as in all issues, we provide a summary of the literature published related to acceptance and commitment therapy, mindfulness and relational frame theory. We link summaries to particular topics and provide a review of the articles. Feel free to read the summaries and find the links to the references and abstracts related to the summaries right in the document. For a taste of what is in the Update, we summarize 3 articles on acceptance approaches to treatment, 3 on addiction that compare CBT to ACT, 1 on assessment by Wilson – the VLQ is alive and well -, 2 case study designs looking at the treatment of GAD and cancer, 3 articles on mindfulness based approaches with children and parents, 4 articles on experiential avoidance, 5 on mindfulness including how mindfulness works with managing emotions, intrusive thoughts, stress reduction and substance use. Finally, we have 3 on RFT reviewed by Ian – Thanks Ian!
We have sorted and distributed articles to our reviewers for the first half of 2011. We are looking forward to the next round.
Please let us know if we missed anything that we should include or inform us of dissertations, etc.
Thanks and Enjoy!
Kind Regards,
Robyn D. Walser, Ph.D.
ACT/RFT Reader's Update: Final 2009 Review (July, 2010)
ACT/RFT Reader's Update: Final 2009 Review (July, 2010)Science and Practice: ACT /RFT Reader’s Update: Final 2009 Review
Welcome to the ACT/RFT Reader’s update. This is the last issue reviewing the literature on ACT and RFT from 2009. We will be publishing updates for 2010 in late summer, fall and winter.
To kick off the issue, we want to extend a thank you to Dr. Chad Drake who has been with the Update since its inception. We thank Chad as he closes the “Update chapter of his life” and wish him much success in his new and fun endeavors. Thanks Chad!
In this issue, we summarize articles on assessment, ACT and diagnostic populations, experiential avoidance, behavioral health, RFT, mindfulness and “The Great Debate”.
The attached PDF includes a Table of Contents that allows you to “click” directly to the summary of multiple articles covering a topic and/or references and abstracts that you may be interested in. In addition, citations for the latest books, book chapters, editorials, and unpublished dissertations are listed.
Our aim with this update is to provide information that is clinically relevant, scientifically sound, and of interest in the ACT/RFT community. We have worked to keep the “busy” reader in mind and hope that you find the Update useful.
** If you are a graduate student working on an ACT/RFT study and would like to have us include your dissertation or thesis citation in this update,please send us an email backchannel.
**If you have published an editorial you would like us to include that citation, please send us an email back channel.
We hope you will find our e-mail updates of interest and value.
Our editors and reviewers include:
Robyn Walser, PhD
Maggie Chartier, PhD, MPH
Katie Sears, PhD
Thuy Tran, BS
Chad Drake, PhD
Elizabeth Gifford, PhD
Ian Stewart, PhD
Christi Ulmer, PhD
Miguel Rodríguez Valverde, PhD
Darrah Westrup, PhD
ACT/RFT Reader's Update (December, 2009)
ACT/RFT Reader's Update (December, 2009)| Science and Practice: ACT/RFT Reader’s Update December, 2009 |
___________________
Acceptance and Values-Based Action in Chronic Pain: A Study of Treatment Effectiveness and Process Cognitive-behavioral approaches to pain management have an established record of empirical support. However, as true with other behavioral problems, the mechanism by which improvement occurred is inconsistent with the theoretical underpinnings of CBT. In a recent paper, Vowles and McCracken add to their ongoing line of research in acceptance-based approaches to the treatment of chronic pain. In their paper, they present their findings of an inter-disciplinary treatment program based in Acceptance and Commitment Therapy, with a focus on acceptance and values-based action. One-hundred seventy-one participants completed the program which consisted of 3 to 4 weeks of inpatient treatment for about 30 hours per week. Participants improved across almost all domains, including pain, depression, pain-related anxiety, disability, medical visits, work status, and physical performance, and effect sizes for these improvements were medium to large. Analysis of reliable change revealed that 75.4% of participants improved in at least one key domain assessed. In contrast with CBT-based approaches to pain management, improvements across these domains were associated with ACT's proposed mechanisms of action, namely, acceptance of pain and values-based action. The authors conclude that these findings provide support for the ACT model of treatment for chronic pain, and the processes associated with improvement – acceptance and values-based action.
Vowles, K., & McCracken, L. (2008). Acceptance and values-based action in chronic pain: a study of treatment effectiveness and process. Journal of consulting and clinical psychology, 76(3), 397-407.
___________________
Rule-Governed Behavior and Psychological Problems Humans, uniquely among animals, can come to understand and respond to linguistic rules, both effective ones and not so effective ones. The effective ones help us to learn and adapt to our environment. The ineffective ones can cause maladaptive behavior and diminish our lives considerably. This paper presents a functional analysis of patterns of rule-governed behavior (RGB) and shows how rules can contribute to psychopathology. Rules have been described as antecedent stimuli that alter the functions of stimuli in our environment. They allow us to respond to that environment in complex and efficacious ways. But what are rules? Relational Frame theory suggests that we humans learn to respond in accordance with abstract relational patterns based on cues (e.g., SAME). Rules are essentially combinations of cues that specify particular relations between environmental stimuli and between environment and behavior and thus allow us to respond in new ways (‘transformation of function’). The paper describes three functional patterns of RGB. These are pliance, tracking and augmental rule following. Pliance is RGB under the control of a history of socially mediated reinforcement for coordination between behavior and antecedent verbal stimuli (rules). A typical example might be a child obeying the rule ‘Don’t touch my laptop’ because their parent has given them this rule and because their parent has previously provided consequences for following or not following rules. Tracking is RGB under the control of a history of coordination between the rule and the way the environment is arranged independently of the rule. An example might be a child obeying the parental rule ‘Eat your breakfast because it will give you more energy’ because in the past the child has experienced the effect of other rules that have been accurate in their description of the environment. If this rule also shows coordination (i.e., the child finds an increase in energy when they eat breakfast), then this will further strengthen tracking behavior. Augmenting is RGB due to relational networks that alter the degree to which events function as consequences. The example given is ‘Eat your vegetables to be a big strong boy’. If this rule makes vegetable eating more reinforcing then it might be described as augmenting. Each of these patterns has its advantages and its disadvantages, including maladaptive behavior. It’s useful for children to learn pliance since this allows them to acquire useful adaptive habits, but doing things just because one is told to can make one insensitive to one’s environment. Tracking allows independence from social whim, but tracking can also lead to ineffective behavior; for example, tracking short term reinforcement can mean one misses longer term reinforcement. Augmenting is the most advanced form of rule governed behavior and as such it can interact with and reinforce either of the other two functional patterns resulting in strongly adaptive or maladaptive patterns. Experiential avoidance can be a product of the latter while valuing, an important part of the antidote to EA, is an example of the former. Törneke, Luciano and Valdivia (2008) have provided an excellent description of RGB and its relationship to psychopathology.
Törneke, N. Luciano, C. & Valdivia Salas, S. (2008). Rule-Governed Behavior and Psychological Problems. International Journal of Psychology and Psychological Therapy, 8 (2), 141-156.
___________________
Brief Review: A Parametric Study of Cognitive Defusion and Believability The effects of the “Milk, milk, milk” exercise are dependent upon the length of the intervention: Reducing distress in respect to private events has been a major emphasis of traditional behavioral and cognitive behavioral therapies. The inclusion of mindfulness interventions in some contemporary therapies like ACT has shifted this focus from distress reduction to changing the behavior regulatory functions of distressing private events. One means of examining this change is by asking clients about the believability of their thoughts. Defusion interventions represent efforts to disrupt this behavior regulation, and the “milk, milk, milk” exercise is the intervention examined in this article. Two studies examined the effect of this exercise on the emotional discomfort and believability of a negative, self-relevant word identified by the participant as sufficiently problematic. Each study varied the amount of time spent repeating the word – 0, 3, or 20 seconds in study 1 and 1, 10, or 30 seconds in study 2. A rationale for the procedure and training with the word “milk” was provided before each intervention. Results showed that emotional distress reduced significantly within 3-10 seconds, while believability reduced significantly only after 20-30 seconds. The difference in timing for these reductions suggests that discomfort and believability are functionally distinct behaviors. The authors suggest extending defusion exercises until the believability of thoughts, rather than just emotional distress, diminishes.
Masuda, A., Hayes, S. C., Twohig, M. P., Drossel, C., Lillis, J., & Washio, Y. (2009). A parametric study of cognitive defusion and the believability and discomfort of negative self-relevant thoughts. Behavior Modification, 33, 250-262.
___________________
Brief Review: Relational Frame Theory and Social Categorization The Matching-to-Sample procedure can transform the functions of arbitrary stimuli in the Implicit Associations Test: This study examined the acquisition of obesity stigma to arbitrary stimuli. More specifically, the matching-to-sample (MTS) procedure was used to provide relational conditioning sufficient to generate a transformation of stimulus functions for stigma to images of either horizontal or vertical lines. The Implicit Associations Test (IAT) was used to detect this transformation of functions. Fifty undergraduate psychology students engaged in a series of five computerized tasks: (1) an IAT containing evaluative words and images of horizontal and vertical lines, to confirm a lack of pre-existing bias, (2) an established IAT for detecting implicit evaluative bias toward obesity, to confirm the presence of pre-existing bias, (3) two MTS tasks providing relational conditioning sufficient to generate the transfer of positive and negative evaluative functions to images of horizontal and vertical lines, (4) the same IAT used in step 1, to assess for the acquisition of bias, and (5) the same IAT used in step 2. Results confirmed no pre-existing bias at time 1, a large and significant predicted bias at time 2, and a small and significant predicted bias at time 4. The results of this study are discussed in respect to an RFT account of the development of stigma and social categorization and contrasted with a more mainstream, cognitive account known as the Social Knowledge Structure.
Weinstein, J. H., Wilson, K. G., Drake, C. E., & Kellum, K. K. (2008). A relational frame theory contribution to social categorization. Behavior and Social Issues, 17, 39-64.
| Revised/Reviewed by: Walser, R., Chartier, M., Sears, K., Drake, C., Valverde, M., Stewart, I., Ulmer, C., & Westrup, D. Read the ACT RFT Reader's Update: References & Abstracts, 2008 in an interactive PDF, attached below. |
ACT/RFT Reader's Update (Fall, 2008)
ACT/RFT Reader's Update (Fall, 2008)Science and Practice: ACT /RFT Reader's Update Fall, 2008
Welcome to ACT/RFT Reader's Update:
In our second issue we summarize 5 articles recently published in peer-reviewed journals. The references to full citations and whether they are available for download on the ACBS website is also included. Citations for the latest books, book chapters, and unpublished dissertations are listed at the end of the update. If you don't see your recently published article….hang on, we continue to work on future issues and have a fair number of articles that are being reviewed and summarized for our coming issues. However, if you are publishing or have recently published please make us aware by either sending us the reference or pdf. Thanks.
We hope you will find our e-mail updates of interest and value.
Enjoy your read!
Our editors and reviewers/writers:
Editors:
Robyn D. Walser, Ph.D.
Maggie Chartier, MPH, MS
Reviewers/Writers:
Chad Drake, MA
Miguel Rodríguez Valverde, PhD
Ian Stewart, PhD
Christi Ulmer, PhD
This issue of Science and Practice: ACT/RFT Readers Update contains 5 summaries:
ACT ARTICLES AND RELATED TOPICS
Acceptance and commitment training reduces prejudice and promotes diversity-oriented behaviors in college students
Despite increased efforts at promoting diversity in recent years, prejudice continues to result in diminished quality of life for ethnic, racial and religious minorities across numerous life domains. Interventions designed to reduce prejudice have been moderately successful with short-term improvements, but do not seem to promote sustained equitable attitudes and behavior. In fact, in some instances, the interventions actually result in an increased bias. ACT may be particularly applicable to prejudice due to its focus on intransigent and difficult cognitions. Luoma and Hayes compared a brief ACT Training protocol to an education-based prejudice awareness training intervention for reducing racial and ethnic prejudice in college students. Material was presented to students using a counterbalanced within-group design such that the impact of each approach could be evaluated independently. The outcome measure, developed for this study, consisted of items assessing the following: awareness of bias; acceptance and flexibility; thought control and defusion; and positive actions. Student responses suggest that the ACT training produced greater reductions in prejudice across most dimensions, and that only ACT training promoted greater intention to engage in diversity-oriented behaviors. Changes in these positive intentions were partially mediated by acceptance and flexibility, and defusion processes explained more variance in positive intention outcomes than acknowledgement of bias. The authors suggest that the combined findings of this study and a previous ACT-based study on prejudice lend preliminary support to an ACT-RFT based model of understanding and reducing prejudice. The findings are also consistent with the theory underlying acceptance-based approaches stating that it is the relationship with thought rather than the content of thought that matters. Limitations of the study include the use of an unvalidated outcome measure, the potential self-selection bias of students who choose to enroll in a class on the psychology of racial differences, the potential for bias of the interventionist in favor of ACT, and a short follow-up interval. Future studies are proposed using a more intensive intervention and assessing longer-term outcomes. Given the need for empirically supported approaches to address prejudice, the findings of the current study are promising. In terms of clinical application, the authors propose that similar processes are likely in play with regard to mental health stigma, and that cognitive processes that promote prejudice are themselves psychologically damaging.
Read the Article:
Lillis, J., & Hayes, S. C. (2007). Applying acceptance, mindfulness, and values to the reduction of prejudice: A pilot study. Behavior Modification, 31(4), 389-411.
________________
ACT and CT for anxiety and depression, a randomized controlled effectiveness trial
For some period of time there has been discussion and even argumentation between those who hold true to cognitive models of intervention (e.g. Beckian) and acceptance models of intervention (e.g. Hayesian). Forman and colleagues take a closer look. They explain that Cognitive Therapy (CT) has a mixed record of success in producing theoretically-consistent mediation of treatment outcomes while Acceptance and Commitment Therapy (ACT) has a relatively impressive, though preliminary record, of the same. Given that only a handful of studies have directly compared these treatments and that all contained methodological shortcomings the authors undertook that task of comparing each therapy's ability to produce mediation and positive outcomes among an outpatient sample of college students in a well-controlled trial. Services were provided by clinical psychology doctoral candidates working at a student counseling center. Outcome measures included self-reports of symptoms (BDI-II, BAI, OQ-45) and self-reports of quality of life (QOLI, SLS). Two mediational measures were administered (KIMS, AAQ). The study also included measures of treatment fidelity, therapist allegiance, and participant expectancies of treatment. Results showed that all measures were comparable between treatments, and that each treatment generated large effect sizes. Mediational analyses showed that the observing subscale of the KIMS more strongly (though nonsignificantly) predicted outcomes for CT, while the AAQ and the acting with awareness and acceptance subscales of the KIMS more strongly (and significantly) predicted outcomes for ACT. The authors reported that "changes in "observing" and "describing" one's experiences were more strongly associated with outcomes for those in the CT group relative to those in the ACT group, whereas experiential avoidance, acting with awareness, and acceptance were more strongly associated with outcomes for those in the ACT group" (p. 792). Although, the authors concluded that "these findings support the notion that CT and ACT are functionally distinct from one another" (p. 792), it was never explained why the capacity to observe and describe one's private experiences is a fundamental component of CT but not ACT.
Read the Article:
Forman, E. M., Herbert, J. D., Moitra, E., Yeomans, P. D., & Geller, P. A. (2007). A randomized controlled effectiveness trial of Acceptance and Commitment Therapy and Cognitive Therapy for anxiety and depression. Behavior Modification, 31, 772-799.
RFT ARTICLES
How does multiple-exemplar training and naming establish derived equivalence in an infant?
Stimulus equivalence at its simplest can be described as follows. Imagine I train someone in the following two relations between physically different arbitrary stimuli: Pick stimulus B when you see stimulus A, and pick stimulus C when you see stimulus B. If given the opportunity, a verbally able human might subsequently go on to demonstrate further relations, without being trained to do so, including picking A when he sees B, and picking B when he sees C (i.e., reversing the trained relations, referred to as symmetry), picking C when he sees A (i.e., combining the trained relations, referred to as transitivity) and picking A when he sees C (a combination of symmetry and transitivity). This pattern of derived responses has been called stimulus equivalence, because it appears that, suddenly and unexpectedly and without being trained to do so, the person is treating a number of physically different stimuli as mutually substitutable for or equivalent to each other. There is growing interest in stimulus equivalence research as only verbally able subjects seem to be able to show this pattern readily, suggesting a link between equivalence and language. But what is the nature of this link? How are the two connected? The present paper discusses two theoretical approaches that claim to account for this link - Relational Frame Theory (e.g., Hayes et al., 2001) and Naming Theory (Horne & Lowe, 1996). More importantly, however, the paper reports a series of experiments involving training an infant in relational responding that provide important additional evidence pertaining to the debate between these approaches. More specifically, the results add to evidence in favour of the RFT account, while demonstrating a phenomenon that directly contradicts Naming Theory. This study is a significant empirical contribution for a number of reasons (i) It demonstrates the use of multiple exemplar training to establish generalized contextually controlled receptive mutual entailed relational responding; (ii) it provides the youngest empirical example of coordinate (sameness) combinatorial entailed relational responding (equivalence) ever recorded; and (iii) it provides extremely important evidence vis-a-vis the Naming Theory / RFT debate by providing empirical evidence that directly contradicts a core tenet of Naming Theory while being consistent with RFT.
Read the Article:
Luciano, C., Becerra, I. G., & Valverde, M. R. (2007). The role of multiple-exemplar training and naming in establishing derived equivalence in an infant. Journal of the Experimental Analysis of Behavior, 87(3), 349-365.
________________
Can the Implicit Relational Assessment Procedure be faked? First evidence says no.
The Implicit Relational Assessment Procedure (IRAP) is a computer-based task for the assessment of implicit cognitions recently devised within the theoretical framework of RFT. It is a latency-based response measure that intends to assess the participants' existing verbal-relational networks (i.e. beliefs). It works by requiring participants to respond as quickly and accurately as possible across trials when presented with particular relations (among sample and target stimuli) that may be consistent or inconsistent with their beliefs (i.e. relational networks). The idea is that participants will be faster when required to respond to stimulus relations that are consistent (e.g. categorizing words like love or peace as pleasant, and words like vomit or death as unpleasant) than to stimulus relations that are inconsistent with their verbal histories (e.g. categorizing vomit or death as pleasant, and love or peace as unpleasant). This idea is supported by empirical evidence from several recent studies. As with other implicit measures, like the Implicit Association Test (IAT), one of the strengths of the IRAP is that it may be less sensitive than questionnaires and other explicit measures to assess deliberate attempts to conceal information about one's own socially sensitive attitudes. This study attempted to see to which extent this is the case (i.e. whether the IRAP can be faked). Three groups of participants underwent two consecutive exposures of the IRAP task with the same stimuli (the words pleasant and unpleasant as samples, the words similar and opposite as response options, one set of six pleasant target words, and one set of six unpleasant target words). Between both exposures, one group was informed about how the IRAP works. Another group received the same information and was told to fake the IRAP, without a specific strategy to do so. The third group received the same information and were also provided with a strategy, namely slowing down on consistent trials and going fast on inconsistent trials. Results showed no evidence of faking in any condition. All groups showed an IRAP effect in the second exposure regardless of the instructions or strategies received. According to a post-task questionnaire, only two participants in the third group reported using the specific strategy they had received. All in all, participants found it difficult to fake the IRAP, even if provided with specific strategies. This contrasts with previous findings with the IAT, which can be successfully faked when explicitly told how to do so. This observed resistance to deliberate attempts to fake performance renders the IRAP a solid procedure for the assessment of implicit cognitions.
Read the Article:
McKenna, I., Barnes-Holmes, D., Barnes-Holmes, Y., & Stewart, I. (2007). Testing the Fake-ability of the Implicit Relational Assessment Procedure (IRAP): The First Study. International Journal of Psychology and Psychological Therapy, 7, 253-268. (in English)
______________________
What can RFT add to the study of pain?
The current study focuses on an RFT interpretation of the way that pain takes part in complex behavioural episodes for humans. It is a theoretical/conceptual study that reviews functional-contextual approaches to the study of private events specifically related to pain and with a special emphasis in recent research in verbal behaviour, behaviour-behaviour relations, and transformation of psychological functions. The review is divided into four parts. The first summarizes the philosophical assumptions of functional-contextualism and its implications for the study of pain (e.g. the extent to which explanations of pain allow for effective action as the criterion against which these explanations should be tested). The second focuses on the classical behaviour-analytic point of view, where pain experiences have been conceptualized as private events that exert discriminative control over subsequent behaviours (e.g. abuse of pain-killers, inactivity, social isolation, etc.). This discriminative function (behaviour-behaviour relation) is the product of specific histories of reinforcement along the individual's development, in direct-contingency terms. This view is illustrated with the presentation of the contributions of Schoenfeld and, more specifically, of Fordyce. RFT is proposed as a more comprehensive framework for the behaviour ral study of pain, a framework where verbal (derived) histories can be included as part of the explanation. In line with this, pain-related clinical problems are conceptualized as a form of experiential avoidance disorder, where it is the verbal functions of pain, rather than pain itself, that limit the individual's life (i.e. the consideration of pain as a literal barrier for engaging in valued actions). This is described in the third part of the article. Finally, the last part of the article presents a general overview of ACT and describes its implications for the treatment of pain-related problems.
For more information, read the original article in Spanish:
Gutiérrez Martínez, O., & Luciano Soriano, C. (2006). Un studio del dolor en el marco de la conducta verbal. International Journal of Clinical and Health Psychology, 6, 169-188. [A study of pain in the framework of verbal behavior: from the contributions of W. E. Fordyce to Relational Frame Theory (RFT)]
(for correspondence and reprints): [email protected]
BOOKS
Ciarrochi, J. V., & Bailey, A. (2008). A CBT practitioner's guide to ACT. Oakland, CA: New Harbinger.
BOOK CHAPTERS
DISSERTATIONS
Barthold, C., & Hoffner, C. (2007). Factors affecting the generalization of 'wh-' question answering by children with autism. Dissertation Abstracts International Section A: Humanities and Social Sciences, Vol 68(4-A): 1403.
EDITORIALS AND COMMENTARIES
Hayes, S. (2007). Hello Darkness. Psychotherapy Networker, Sept/Oct. 46-52.
Hummelen, J. W., & Rokx, T. A. J. J. (2007). Individual-context interaction as a guide in the treatment of personality disorders. Bulletin of the Menninger Clinic, 71(1): 42-55.
Muran, J. C. (2007) Commentary: Language, Self, and Diversity. In S. C. Hayes (Ed.), Dialogues on difference: Studies of diversity in the therapeutic relationship ) pp. 275-279. Washington, DC, US: American Psychological Association.
ACT/RFT Reader's Update (Winter, 2007)
ACT/RFT Reader's Update (Winter, 2007)ACT with Special Populations or in Specific Settings
ACT with Special Populations or in Specific SettingsACT is a general model of the language and cognition processes involved in reducing psychological suffering and promoting human well-being. As such, it is not a specific set of techniques. Any ACT intervention is an instance of a general psychological strategy which is designed to be flexibly applied. ACT can be applied in short interventions done in minutes or hours, as well as in interventions which take many sessions. ACT can be used in groups, individual sessions, classroom settings, couples therapy, bibliotherapy, workplace trainings, and much more. Be sure to check out our collection of ACT treatment protocols and list of books for Specific Populations.
There are several Special Interest Groups (SIGs) focused on specific populations and settings. This is a partial list of SIG topics. To see the full list of Special Interest Groups, click here.
- Addictions
- Aging
- Asian Culture
- Autism
- Cancer
- Children, Adolescents & Families
- Coaching
- Educational Settings
- Forensic and Corrections
- Gender and Sexual Diversity
- Leadership and Organizational Behavior Management
- Military Personnel and Veterans
- OCD
- Pain
- Perinatal
- Primary Care
- Psychosis
- Sport and Human Performance
- Trauma
Fellow Travelers
Fellow TravelersThe third generation of cognitive behavior therapy (CBT) has been defined this way:
Grounded in an empirical, principle-focused approach, the third wave of behavioral and cognitive therapy is particularly sensitive to the context and functions of psychological phenomena, not just their form, and thus tends to emphasize contextual and experiential change strategies in addition to more direct and didactic ones. These treatments tend to seek the construction of broad, flexible and effective repertoires over an eliminative approach to narrowly defined problems, and to emphasize the relevance of the issues they examine for clinicians as well as clients. The third wave reformulates and synthesizes previous generations of behavioral and cognitive therapy and carries them forward into questions, issues, and domains previously addressed primarily by other traditions, in hopes of improving both understanding and outcomes. (Hayes, 2004)
The most unique characteristic of the third wave interventions is the degree of emphasis on contextual and experiential change strategies, including acceptance, defusion, mindfulness, relationship, values, emotional deepening, contact with the present moment, and the like. The purpose of experiential and contextual strategies of this kind is to rapidly alter the function of problematic psychological events, even if their form or frequency does not change or changes only slowly. Mindfulness-based and acceptance technologies show that focus quite clearly. For example, Segal, Teasdale, and Williams (2004) state: “Unlike CBT, there is little emphasis in MBCT on changing the content of thoughts; rather, the emphasis is on changing awareness of and relationship to thoughts.”
It is worth noting that this step is being taken both by techniques that are quite behavior analytic and thus philosophically contextualistic in their rationalization (e.g., Behavioral Activation, ICBT, DBT, ACT, FAP), and by techniques that are quite cognitive in their rationalization (e.g., MBCT, Metacognition).
This is important, because it means that the mainstream itself is changing and there are new opportunities for connection and communication across old boundaries. In a kind of dialectical synthesis of a previous thesis and antithesis, the new wave therapies seem to be healing old wounds and divisions between behavioral and cognitive perspectives. Evidence for this view can be found in the synergies between technologies across of the spectrum of third wave interventions, and in the ways that each of these new approaches has breadth across these divisions regardless of its home of origin. The third wave interventions are not a rejection of the first and second waves of behavioral and cognitive therapy so much as a transformation of these earlier phases into a new, broader, more interconnected form. Thus, while the implications may be revolutionary, the processes giving rise to these developments are evolutionary – as might be expected in an explicitly empirical tradition.
We invite child pages to be added in any of the methods and approaches that are part of a more contextual approach (simply click the "add child page" link at the bottom of the relevant page).
Fellow Travelers FAQ
Fellow Travelers FAQACBS Members: To suggest a question for someone to answer, click on the "add new comment" link at the bottom of this page and enter your question. To provide a question and an answer to this FAQ, click on the "add child page" link at the bottom of this page.
What characterizes the so-called third wave behavior therapies?
What characterizes the so-called third wave behavior therapies?”Grounded in an empirical, principle-focused approach, the third wave of behavioral and cognitive therapy is particularly sensitive to the context and functions of psychological phenomena, not just their form, and thus tends to emphasize contextual and experiential change strategies in addition to more direct and didactic ones. These treatments tend to seek the construction of broad, flexible and effective repertoires over an eliminative approach to narrowly defined problems, and to emphasize the relevance of the issues they examine for clinicians as well as clients. The third wave reformulates and synthesizes previous generations of behavioral and cognitive therapy and carries them forward into questions, issues, and domains previously addressed primarily by other traditions, in hopes of improving both understanding and outcomes.” (quote from Hayes, 2004).
These are very broad characterizations and there is no clear dividing line between various historical aspects of the behavior therapy tradition.
How does Relational Frame Theory (RFT) relate to traditional CBT-theories?
How does Relational Frame Theory (RFT) relate to traditional CBT-theories?That question is a huge one. RFT seeks a broad understanding of cognition. In the long run it could be more important than ACT because if it works the whole of psychology could change.
RFT is developmental, contextual, and behavioral. It gives you ideas about what to change to make things happen. It is so basic that it goes all the way down to animal behavior and human infants; and yet so broad in scope that it has clear implications for our understanding of social processes or such human activities as religion.
We have never had an empirically adequate behavioral, contextual account of cognition. Now we have at least the beginnings of one and it seems to be braking down the artificial barriers between cognitive and behavioral science.
The theories underlying CBT and CT are not like that. They have relatively low scope and they emerged typically from clinical concerns. They do not pretend to be the functional equivalent in cognition for what “behavioral principles” are in non-verbal behavior.
You have to be impressed with what the traditional behavior therapists were able to do with traditional behavioral principles, in part because these principles emphasized manipulable contextual variables. Imagine what we might do with a theory of cognition that emphasized manipulable contextual variables, if the theory was relatively adequate. Maybe a lot.
ACT, evolutionary biology and severe mental illness
ACT, evolutionary biology and severe mental illnessOriginally submitted by user dixonph on 7/30/2014:
Edward Hagen's paper: Delusions as Exploitative Behavior
http://bit.ly/1ppVlnu echoes themes of ACT theorists. ACT is held by the founders as a possible aid for even severe psychotic disorders. Contextual behavior theory is not mentioned as such in Hagen's paper. I don't know if Hagen is involved with mental illness treatments, or ACT specifically. The paper seems to be very much in line with ACT principles. That is why I mention it here. I see a connection.
If even severe mental illness is an evolutionary adaptive survival mechanism manifested as a result of a failed social context, then how can ACT help reintegrate the modern sufferer into more successful social connections?
Can there be communities where ACT functions to create an experience of acceptance and support for sufferers even outside the therapeutic setting?
I am looking to see if Edward Hagen is involved with ACBS/ACT. His paper states that he believes anti-psychotic medication will not really help someone with what is called delusional disorder (semi-plausible delusions, continued day to day routine functioning), which is distinct from the bizarre delusions of schizophrenia. He also mentions the harmful side effects of the medications.
I am interested in the potential for ACT in supportive community for mental health sufferers.
Any known efforts among ACT practioners?
Differences/Similarities between ACT/DBT
Differences/Similarities between ACT/DBTACT and DBT could be considered sister/brother technologies. Both have been described as part of the "third wave" of cognitive-behavioral therapies, which also includes therapies such as mindfulness-based cognitive therapy and integrative behavioral couples therapy (and potentially the new modern behavior analytic form of behavioral activitation by the deceased Jacobson and colleagues that seems to be outperforming cognitive therapy for depression in two trials). This new set of therapies, all of which have a commitment to empirical evaluation and science, tend to differ in important ways from traditional CBT. For example, the third wave tends to pay more attention to secondary change in the area of thoughts and feelings. Traditional CBT tries to help people directly change thoughts and feelings, sort of an in-with-the-good out-with-the-bad approach to cognitive and emotional content. These third wave approaches focus on helping people to change their relationship to these private experiences, rather than trying to change the form, situational sensitivity, or content of these experiences. Emphasis then tends to turn to being effective in one's life and away from working to feel GOOD. Another way to put this is that these therapies tend to help people learn how to FEEL good, rather than to try to feel GOOD. Anyways, there are papers written about this new set of therapies and their similarities and differences for those who want more info.
Here's a little about what I see as differences/similiarities between DBT and ACT, with the disclaimer that I am far from an expert on DBT. DBT and ACT both emerge from a behavioral tradition. Both share the similarity of emphasizing acceptance, mindfulness, and effectiveness of action. In at least those domains they are quite similar. In terms of the theory that underlies them, they are quite different. ACT is closely tied to a modern behavior analytic theory of language and cognition called Relational Frame Theory (RFT), which underlies the approach, and also to traditional behavior analytic principles such as reinforcement. The first clinical trials on ACT were published several years before DBT (in 1985-86 with depression), but then Steve Hayes decided that ACT needed a firmer theoretical foundation and this lead to about 15 years of research and dozens of studies on RFT before the next application of RFT (an ACT clinical trial on psychosis) was published in 1999. My experience with DBT is that its focus has been on developing a technology that is practical, pragmatic, and manualized, with less of an emphasis on developing a comprehensive theory of human behavior. ACT is very closely tied to the broader tradition of behavior analysis and could be considered a form of clinical behavior analysis while DBT seems to be more closely tied to traditional behavior therapy.
In terms of overlap in specific techniques between ACT and DBT, the overlap appears limited. There seems to be very little overlap in terms of the specific techniques, exercises, and metaphors used in session (with the exception of general mindfulness exercises).
In terms of the evidence base, DBT undoubtedly has a stronger evidence with more replication in the more limited areas that it has been tested (e.g., parasuicidality/substance abuse), while ACT has been examined in a wider variety of clinical trials, with less replication, with more disorders (e.g., chronic pain, substance abuse, depression, workplace settings, anxiety, and a dozen or so other), probably due to the broader scope of its underlying theory.
[this is exerpted from an email to a listserv in Oregon and I thought others might be interested in this. Feel free to modify or comment on any disagreement/inconsistencies/extensions]
Glossary
GlossaryGlossary of Terms
Cfunc
CfuncA context that controls the transformation of stimulus functions. Pronounced "cee funk." (Note: the "func" portion of this term typically appears as subscript, which is difficult to implement in HTML).
Crel
CrelA context that controls framing events relationally. While these can include nonarbitrary features of the relata in some circumstances, the same relational behavior must also be controlled by arbitrary contextual cues in other circumstances in order to define the response as arbitrarily applicable. Pronounced "cee rel." (Note: the "rel" portion of this term typically appears as subscript, which is difficult to implement in HTML).
acceptance
acceptanceAcceptance is defined in ACT as "actively contacting psychological experiences -- directly, fully, and without needless defense -- while behaving effectively." (Hayes, Wilson, Gifford, Follette, & Strosahl, 1996, p. 1163)
analytic-abstractive theory
analytic-abstractive theoryOrganized sets of behavioral principles emerging from coherent sets of functional analyses that are used to help predict and influence behaviors in a given response domain.
arbitrarily applicable relational responding
arbitrarily applicable relational respondingarbitrary
arbitraryaugmenting
augmentingbehavior analysis
behavior analysisbehavioral principles
behavioral principlescombinatorial entailment
combinatorial entailmentA defining feature of relational frames that refers to the ability to combine mutually related events into a relational network under forms of contextual control that can include arbitrary contextual cues. Combinatorial entailment applies when in a given context A is related in a characteristic way to B, and A is related to C, and as a result a relation between B and C is now mutually entailed. The specific form of the network does not matter. It would be as correct to say that combinatorial entailment applies when in a given context A is related in a characteristic way to B, and B is related to C, and as a result a relation between A and C is now mutually entailed. Combinatorial entailment can be represented by the formula below.
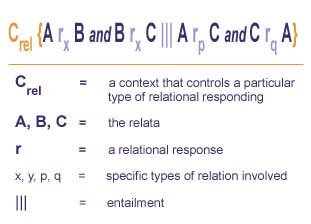
complete relational network
complete relational networkNetworks of events containing Crel terms that set the occasion for the relational activity necessary to specify a relation between the events in the network.
contextual psychology
contextual psychologycontextualism
contextualismcontinuity assumption
continuity assumptioncoordination
coordinationdeictic frames
deictic framesDeictic relations specify a relation in terms of the perspective of the speaker such as left/right; I/you (and all of its correlates, such as "mine"; here/there; and now/then. Some relations may or may not be deictic, such as front/back or above/below, depending on the perspective applied. For example, the sentence "The back door of my house is in front of me" contains both a spatial and deictic form of "front/back." Deictic relations seem to be a particularly important family of relational frames that may be critical for perspective-taking. An example is the three frames of I and YOU, HERE and THERE, and NOW and THEN. These frames are unlike the others mentioned previously in that they do not appear to have any formal or nonarbitrary counterparts. Coordination, for instance, is based on formal identity or sameness, and "bigger than" is based on relative size. In contrast, frames that depend on perspective cannot be traced to formal dimensions in the environment at all; instead, the relationship between the individual and other events serves as the constant variable upon which these frames are based.
depth
depthdistinction
distinctionfamilies of relational frames
families of relational framesRelational frames can be roughly organized into families of specific types of relations. This list is not exhaustive, but serves to demonstrate some of the more common frames and how they may combine to establish various classes of important behavioral events.
- frames of coordination
- frames of opposition
- frames of distinction
- frames of comparison
- hierarchical frames
- deictic frames
- other families: other families of relations include spatial relations such as over/under and front/back, temporal relations such as before/after, and causal/contingency relations such as "if...then"
The foregoing families of relational frames are not final or absolute. If RFT is correct, the number of relational frames is limited only by the creativity of the social/verbal community that trains them. Thus the foregoing list is to some degree tentative. For example, TIME and CAUSALITY can be thought of as one or two types of relations. It is not yet clear if thinking of them as either separate or related may be experimentally useful, relative to the goals of RFT. Thus, while the generic concept of a relational frame is foundational to RFT, the concept of any particular relational frame is not. The purpose in constructing a list of frames is to provide a set of conceptual tools, some more firmly grounded in data than others, that may be modified and refined as subsequent empirical analyses are conducted. To see some brief examples of common families of relational frames, please watch the video families below.
formative augmenting
formative augmentingA form of rule-governed behavior controlled by relational networks that establish given consequences as reinforcers or punishers.
frames of comparison
frames of comparisonThe family of comparative relational frames is involved whenever one event is responded to in terms of a quantitative or qualitative relation along a specified dimension with another event. Many specific subtypes of comparison exist (e.g., bigger/smaller, faster/slower, better/worse). Although each subtype may require its own history, the family resemblance may allow the more rapid learning of successive members. The different members of this family of relations are defined in part by the dimensions along which the relation applies (e.g., size; attractiveness; speed). Comparative frames may be made more specific by quantification of the dimension along which a comparative relation is made. For example, the statement "A is twice as fast as B and B is twice as fast as C" allows a precise specification of the relation within all three pairs of elements in the network.
frames of coordination
frames of coordinationframes of distinction
frames of distinctionThe frame of distinction also involves responding to one event in terms of the lack of a frame of coordination with another, typically also along a particular dimension. Like a frame of opposition, this frame implies that responses to one event are unlikely to be appropriate in the case of the other, but unlike opposition, the nature of an appropriate response is typically not defined. If I am told only, for example, "this is not warm water," I do not know whether the water is ice cold or boiling hot. When frames of distinction are combined, the combinatorially entailed relation is weak. For example, without additional disambiguating information, if two events are different than a third event, I do not know the relation between these two beyond the fact of their shared distinction.
frames of opposition
frames of oppositionOpposition is another early relational frame. In natural language use, this kind of relational responding involves an abstracted dimension along which events can be ordered and distinguished in equal ways from a reference point. Along the verbally abstracted dimension of temperature, for example, cool is the opposite of warm, and cold is the opposite of hot. The specific relational frame of opposition typically (but not necessarily) implicates the relevant dimension (e.g., "pretty is the opposite of ugly" is relevant to appearance). Opposition should normally emerge after coordination because the combinatorially entailed relation in frames of opposition includes frames of coordination (e.g., if hot is the opposite of freezing and cold is the opposite of hot, then cold is the same as freezing).
framing events relationally
framing events relationallyFraming events relationally (or "framing relationally" or "relational framing") refers to a specific type of arbitrarily applicable relational responding that has the defining features in some contexts of mutual entailment, combinatorial entailment, and the transformation of stimulus functions. Framing events relationally is due to a history of relational responding relevant to the contextual cues involved; and is not solely based on direct non-relational training with regard to the particular stimuli of interest, nor solely to nonarbitrary characteristics of either the stimuli or the relation between them. The action of framing events relationally is often referred to in the noun form of "relational frame." Various families of relational frames, or ways of framing events relationally, have been identified.
functional contextualism
functional contextualismgeneralized operant
generalized operanthierarchial frames
hierarchial framesHierarchical relations or hierarchical class memberships have the same diode-like quality of frames of comparison, but the combinatorially entailed relations differ because the hierarchical relation itself is the basis for a frame of coordination. For example, if Tom is the father of Simon and Jane, then Simon and Jane are known to be siblings. If Tom is taller than both Simon and Jane, however, the relative heights of Simon and Jane are unknown. Hierarchical relations are essential to many forms of verbal abstraction.
listening with understanding
listening with understandingThe responses of listeners that are based on framing events relationally.
motivative augmenting
motivative augmentingA form of rule-governed behavior controlled by relational networks that alter the degree to which previously established consequences function as reinforcers or punishers.
mutual entailment
mutual entailmentA defining feature of relational frames that refers to its fundamental bidirectionality under forms of contextual control that can include arbitrary contextual cues. Mutual entailment applies when in a given context A is related in a characteristic way to B, and as a result B is now related in another characteristic way to A. Mutual entailment can be represented by the formula below.
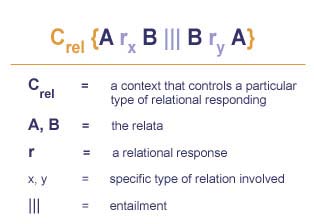
opposition
oppositionOpposition is another early relational frame. In natural language use, this kind of relational responding involves an abstracted dimension along which events can be ordered and distinguished in equal ways from a reference point. Along the verbally abstracted dimension of temperature, for example, cool is the opposite of warm, and cold is the opposite of hot. The specific relational frame of opposition typically (but not necessarily) implicates the relevant dimension (e.g., "pretty is the opposite of ugly" is relevant to appearance). Opposition should normally emerge after coordination because the combinatorially entailed relation in frames of opposition includes frames of coordination (e.g., if hot is the opposite of freezing and cold is the opposite of hot, then cold is the same as freezing).
pliance
plianceA form of rule-governed behavior under the control of a history of socially-mediated reinforcement for coordination between behavior and antecedent verbal stimuli (i.e., the relational network or rule), in which that reinforcement is itself delivered based on a frame of coordination between the rule and behavior. Stated another way, pliance requires both following a rule and detection by the verbal community that the rule and the behavior correspond. Mere social consequation does not define pliance. The rule itself is called a ply.
pragmatic verbal analysis
pragmatic verbal analysisFraming events relationally under the control of abstracted features of the nonarbitrary environment that are themselves framed relationally. Stated in other words, pragmatic verbal analysis involves acting upon the world verbally, and having the world serve verbal functions as a result.
See below for an illustration of RFT's interpretation of pragmatic verbal analysis/problem solving.
precision
precisionproblem solving
problem solvingAlthough problem-solving has both non-verbal and verbal connotations, in a verbal sense problem-solving refers to framing events relationally under the antecedent and consequential control of an apparent absence of effective actions. When the particular problem involves the stimulus functions of the nonarbitrary environment, verbal problem-solving can be said to be pragmatic verbal analysis that changes the behavioral functions of the environment under the antecedent and consequential control of an apparent absence of effective action.
See below for an illustration of RFT's interpretation of pragmatic verbal analysis/problem solving.
relata
relatarelational frame
relational frameA specific type of arbitrarily applicable relational responding that has the defining features in some contexts of mutual entailment, combinatorial entailment, and the transformation of stimulus functions. Relational frames are due to a history of relational responding relevant to the contextual cues involved; and is not solely based on direct non-relational training with regard to the particular stimuli of interest, nor solely to nonarbitrary characteristics of either the stimuli or the relation between them. While used as a noun, it is in fact always an action and thus can be restated anytime in the form "framing events relationally." Various families of relational frames have been identified.
relational network
relational networkA relational frame is the smallest relational network that can be defined, although the term network is usually used to refer to combinations of relational frames, such as A is more than B, B is the same as C, C is less than D. The term network is also used to describe relations between or among relational frames, such as, if A is more than B, and C is more than D, then the relation between A and B participates in a frame of coordination with the relation between C and D.
relational responding
relational respondingResponding to one event in terms of another. See below for an illustration depicting the difference between relational responding and non-relational responding.
rule-governed behavior
rule-governed behaviora.k.a., RGB
In its most general terms, behavior controlled by a verbal antecedent. However, behavior controlled by verbal antecedents is more likely to be termed "rule governed" if the verbal antecedent forms a complete relational network that transforms the functions of the nonarbitrary environment.
See below for an illustration of RFT's interpretation of rule-governed behavior.
scope
scopeScope means that a broad range of phenomena can be analyzed with a given set of analytic concepts (the broader the range the better, so long as precision is not compromised).
strategic problems
strategic problemsThose verbal problems in which the problem solver has placed the desired goal or purpose into a relational frame.
thinking
thinkingtracking
trackingA form of rule-governed behavior under the control of a history of coordination between the rule and the way the environment is arranged independently of the delivery of the rule. The rule itself is called a track.
transfer of stimulus functions
transfer of stimulus functionsA specific type of transformation of stimulus functions between two relata when they participate in a frame of coordination.
transformation of stimulus functions
transformation of stimulus functionsA defining feature of relational frames that refers to the modification of the stimulus functions of relata based on contextual cues that specify a relevant function (Cfunc) and the relational frame that these events participate in (Crel). The transformation of stimulus functions can be represented by the formula below.
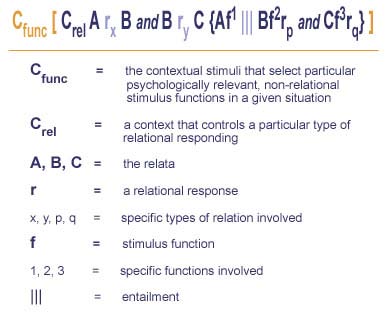
valuative problems
valuative problemsThose verbal problems in which the goal is to place a desired goal or purpose into a relational frame.
varieties of relational frames
varieties of relational framesRelational frames can be roughly organized into families of specific types of relations. This list is not exhaustive, but serves to demonstrate some of the more common frames and how they may combine to establish various classes of important behavioral events.
- frames of coordination
- frames of opposition
- frames of distinction
- frames of comparison
- hierarchical frames
- deictic frames
- other families: other families of relations include spatial relations such as over/under and front/back, temporal relations such as before/after, and causal/contingency relations such as "if...then"
The foregoing families of relational frames are not final or absolute. If RFT is correct, the number of relational frames is limited only by the creativity of the social/verbal community that trains them. Thus the foregoing list is to some degree tentative. For example, TIME and CAUSALITY can be thought of as one or two types of relations. It is not yet clear if thinking of them as either separate or related may be experimentally useful, relative to the goals of RFT. Thus, while the generic concept of a relational frame is foundational to RFT, the concept of any particular relational frame is not. The purpose in constructing a list of frames is to provide a set of conceptual tools, some more firmly grounded in data than others, that may be modified and refined as subsequent empirical analyses are conducted. To see some brief examples of common families of relational frames, click on the video below.
verbal behavior
verbal behaviorThe action of framing events relationally.
verbal stimuli
verbal stimuliStimuli that have their effects because they participate in relational frames.
The Three Earliest ACT Protocols
The Three Earliest ACT ProtocolsSleuthing exactly when the first ACT protocols were written is tricky due to the passage of time, and the fact that computers did not exist so duplicate records meant carbon paper copies on onion skin kept in files and packed in cardboard boxes as moves occurred or new jobs were secured. Thus the reasoning for dating is included below.
The first ACT protocol was likely written by Steve Hayes in late Spring of 1981. At that time the name was "Comprehensive Distancing". An attachment to this page contains that very first protocol ("1981 Big D Manual S C Hayes") which is only 3 pages long. But its clear from the "manual" (an outline really) that the students knew the metaphors and exercises. Steve thinks his "night on the carpet" (www.bit.ly/StevesFirstTED) was during the 1980-81 winter break and that he came back to the lab ready to push hard on studying what he had experienced. He thinks he remembers conducting a workshop in the lab soon after and the "manual" was written after that in the 1981 Spring semester.
The next protocol was written soon after in 1981. Here is how we know that: the study was an analogue study on pain tolerance and it was presented at the Association for the Advancement of Behavior Therapy (now AABT) in 1982:
Hayes, S. C., Korn, Z., Zettle, R. D., Rosenfarb, I., & Cooper, L. (November 1982). Rule‑governed behavior and cognitive behavior therapy: The effects of comprehensive cognitive distancing on pain tolerance. Paper presented at the meeting of the Association for Advancement of Behavior Therapy, Los Angeles.
That means the study was finished by about March of 1982 so it could be submitted.
But Rob Zettle (Steve Hayes's first doctoral student) thinks he likely used that pain manual to help write the manual for his dissertation on Cognitive Therapy vs ACT for depression. One reason to think that: the onion skin carbon copy of that pain protocol was only found in February 2024 (!) while looking for the first "Big D" manual, and Rob found it not in the files for the pain study, but in the cardboard box of files for his dissertation ... as if the protocol was relocated for his reference.
Rob recalls running two subjects for his dissertation project in Greensboro before he left for his internship at the Center for Cognitive Therapy in Philadelphia in the summer of 1982. For that reason he thinks he was writing that protocol in the Fall 1981. His dissertation was conducted with the cooperation and support of Aaron Beck (note, ACT was never "at war" with Tim Beck!) and was defended in 1984 under the title "Cognitive Therapy of Depression: A Conceptual and Empirical Analysis of Component and Process Issues" (ProQuest Dissertations Publishing, 1984, 8509189). Incidentally in the context of the recent move toward ACT as a form of "Process-Based Therapy" it is worth noting the title of this first randomized controlled clinical trial on ACT! ACT was always a form of process-based therapy -- it's just now we have a name for that view.
The pain study was put in a file drawer, not because it was bad but because it was good, and Steve thought it would be more prudent to work out the issues of process measures, components, basic principles of rule-governance and relational framing, and philosophy of science issues before emphasizing outcomes alone.
That took far longer than anyone thought at the time and thus the pain study was only published in 1999, 17 years after it was finished: Hayes, S. C., Bissett, R., Korn, Z., Zettle, R. D., Rosenfarb, I., Cooper, L., & Grundt, A. (1999). The impact of acceptance versus control rationales on pain tolerance. The Psychological Record, 49, 33-47.
An unfortunate historical note is that the pain manual was lost -- although Steve remembered seeing it more than once over the years, it was simply not in Steve's box of materials about the pain study when ACT began to be studied again for outcomes in the late 1990's. This meant that the two labs that were first interested -- Dermot Barnes-Holmes and Bryan Roche -- had to wander in the wilderness trying to replicate it. Both labs eventually did, but it took years to dial in the preparation, so progress was needlessly delayed and effort was wasted. That is one reason why finding the actual manual (25 years after its publication and 42 years after the study itself!) is of such historical importance.
Rob Zettle has written a history of this era and later eras of ACT development. The article describing these early days and more is attached below.
ACT Books
ACT BooksThere are many books, audiobooks, and other materials to help you learn more about ACT and CBS. There may seem like a lot of choices in some areas. And there are, which is a testament to how quickly the ACT work has grown.
- ACT Books
- Other books of interest:
- Books in languages other than English
ACT FAQ
ACT FAQClick on a question below to view its answer!
ACBS Members: If you have a question about the therapy, our ACT for Professionals listserv is probably the best place to ask. (Click here to join.) To provide a question and an answer to this FAQ, click on the "add child page" link at the bottom of this page and contribute a page to the website.
How does ACT differ from traditional CBT interventions?
How does ACT differ from traditional CBT interventions?Are there advantages of ACT as compared to traditional CBT?
Are there advantages of ACT as compared to traditional CBT?Ultimately this is an empirical question. After considering that we can look at the possible advantages in a theoretical sense.
Right now there are a handful of studies that have looked directly and they tend to be medium to small. Only a few are published, and one of these barely mentions outcome because it was a piece on process of change. So we have a long way to go before this question will be answered empirically.
Here are the studies done so far:
Rob Zettle, who trained with Beck, did two very small randomized trials on ACT versus CT for depression – one using individual ACT and CT and the other using ACT and CT group therapy. A larger multi-site randomized trial is underway right now. In his two studies (see the ACT Handout) he found Cohen’s d’s at post between ACT and CT of 1.23 (individually delivered) and .53 (group) and at follow-up of .92 and .75. The N was very small though. The ACT group was only an N of 6 in the individual study and about 10 or so in the group study.
The 4 other studies are brand new and are not published yet. Ann Branstetter did a randomized trial with end stage cancer distress. Ann was trained in traditional CBT and she applied CBT procedures she thought would help (such as cognitive restructuring). There was not follow up because the patients were in end stage cancer but at week 12 ACT had a Cohen’s d of .9 compared to traditional CBT on distress over dying. You can email her for details – she is at Southwest Missouri State University.
Jennifer Block’s dissertation at Albany (she was just hired as a faculty member at LaSalle) compared ACT and CBGT in social phobia and found a Cohen’s d of .45 at post in favor of ACT compared to traditional CBT on the behavioral measure (standing up and speaking).
Carmen Luciano’s team at the University of Almeria just did a smoking trial comparing ACT and a CBT package used by a Spanish cancer society and found a Cohen’s d of .42 at a one year follow up on smoking cessation.
Raimo Lappalainen and his group at the University of Tampere has data in an effectiveness trial comparing ACT and traditional CBT (using CBT methods linked to functional analysis, such as skills training, or exposure) in a training clinic. Beginning student therapists were randomly assigned one ACT and one traditional CBT client (N = 14 each condition). Problems ranged across the usual outpatient spectrum but they were mostly anxiety and depression. On the SCL 90 the post Cohen’s d between ACT and CBT was .62. At follow up the effect was larger. Here is the reference: Lappalainen, R., Lehtonen, T., Skarp, E., Taubert, E., Ojanen, M., & Hayes, S. C. (2007). The impact of CBT and ACT models using psychology trainee therapists: A preliminary controlled effectiveness trial. Behavior Modification, 31, 488-511. By thw ay at the process level there was greater acceptance for ACT patients; great self-confidence for CBT patients. Both correlated with outcomes, but when partial correlations are calculated, only acceptance still relates to outcome. The effect was accidentally not included in the publication but at follow up ACT was now significantly better than CBT in self-confidence.
Evan Foreman and James Herbert reported similar data from their clinic at Drexel University: Forman, E. M., Herbert, J. D., Moitra, E., Yeomans, P. D. & Geller, P. A. (2007). A randomized controlled effectiveness trial of Acceptance and Commitment Therapy and Cognitive Therapy for anxiety and depression. Behavior Modification, 31(6), 772-799. In this study 101 heterogeneous outpatients reporting moderate to severe levels of anxiety or depression were randomly assigned either to traditional CT or to ACT. 23 junior therapists were used. Participants receiving CT and ACT evidenced large and equivalent improvements in depression, anxiety, functioning difficulties, quality of life, life satisfaction and clinician-rated functioning. “Observing” and “describing” one’s experiences mediated outcomes for those in the CT group relative to those in the ACT group, whereas “experiential avoidance,” “acting with awareness” and “acceptance” mediated outcomes for those in the ACT group.
It is also known that ACT methods can empower behavioral methods (which are also part of the ACT model by the way ... so this finding is in essences a confirmation of the model itself). For example, consider this study: Levitt, J. T., Brown, T. A., Orsillo, S. M., & Barlow, D. H. (2004). The effects of acceptance versus suppression of emotion on subjective and psychophysiological response to carbon dioxide challenge in patients with panic disorder. Behavior Therapy, 35, 747-766. In it acceptance methods (drawn directly from the ACT book) did a better job than control strategies in promoting successful exposure to CO2 gas in panic disordered patients.
A similar finding was reported in:
Campbell-Sills, L., Barlow, D. H., Brown, T. A., & Hofmann, S. G. (2006). Effects of suppression and acceptance on emotional responses of individuals with anxiety and mood disorders. Behaviour Research and Therapy, 44, 1251-1263. As with the study above, brief acceptance methods led to lower heart rate during exposure to an aversive film and less negative affect during the post-film recovery period that did control strategies in individuals with anxiety and mood disorders.
So far it looks as though there might be a small advantage for ACT over traditional CBT methods in outcomes; there is a different set of change processes involved, and ACT methods may empower traditional behavioral methods.
Theoretically, the strengths of the ACT model as compared to CBT are these.
1. The model is easily scalable and broadly applicable. If you look at the whole outcome literature done so far (RCTs, controlled time series designs, and case studies) the problems targeted form a pretty broad list: PTSD, panic, depression, racist prejudice, burnout, epilepsy, smoking, OCD, pain, psychosis, cancer, diabetes, multiple sclerosis, sports psychology, attitudes against pharmacotherapy, skin picking, learning new procedures at work, heroin abuse, worksite stress, work innovation, marijuana abuse, and several others.
2. The putative processes of change are well specified with at least marginally adequate measures available in most areas. These change processes are a small set and they do not wildly vary from disorder to disorder.
3. The mediational analyses seem to be working. There are by our count already 16 successful formal mediational analyses published, or completed and coming. So far the data are very supportive. The processes successfully examined so far include acceptance, defusion, values, committed action, and psychological flexibility so most of the key ACT have some data in mediational trials.
4. Specific components seem to be working when inductively tested. There are at least 18 such studies. In every case ACT methods are impactful and work in a way that is theoretically coherent. These include all 6 points of the hexagon model.
5. The basic theory is intricately linked with the technology and itself seems to be working. For example, we are approaching 10 RFT studies linked to the three senses of self in ACT; RFT work on values is coming; and so on.
For those who believe only in RCTs of manuals, much of this answer will be dismissed. But the history of science shows that you cannot create a progressive science using only outcome studies. I (SCH) explained why in The Scientist-Practitioner (Hayes, Barlow, & Nelson-Gray, 1999). In a nutshell, though, it is this: without good theory, the technological development problem is based on common sense categories and it becomes empirically and practically overwhelming.
This should not be heard as “ACT adherents say RCTs are not important.” ACT folks have published nearly 30 RCTs of ACT methods. But they are not enough! Development in the areas of philosophy of science, basic principles, applied theory, specification of processes of change and effectiveness are just as important (and in the long run more important) than efficacy tests of technology.
The scientific game the ACT / RFT / Contextual psychology group is playing is this: to try to create a truly progressive science of psychology that can address the human condition in a more adequate way. Sure that is bold, but why not have bold goals? Is the ACT group willing to stand or fall on RCTs as a measure of success? Ultimately yes. But we want and demand another, even more difficult criteria: seeing a more truly useful psychology emerge as a result. That means concepts, theories, components, basic principles, effectiveness, training, dissemination and so on.
We think it is only fair to insist that ACT be measured against its own very difficult criteria when considering the progress of this effort. For example, examining ACT without examining RFT is like examining a cancer drug without looking at physiology.
Like the hare and the tortoise, ACT is following the slow and steady path. We think traditional CBT hopped ahead into a lay theory of cognition -- which produced quick progress but long term problems. We'd rather take the slow, one step at a time approach of contextual behavioral science. Which one will go farthest? Let's see. Let's be patient and see.
If there is an advantage of the ACT wing of CBT as compared to traditional CBT, this is where you are most likely to see it.
Are there any potential advantages of traditional CBT compared to ACT?
Are there any potential advantages of traditional CBT compared to ACT?It is an empirical question, as was the previous one.
As for data so far, right now we have two studies showing a smaller effect size for ACT than for a traditional CBT procedure done outside of an ACT model. Zettle, 2003 found a smaller effect for ACT than for systematic desensitization with trait anxiety when treating a relatively minor problem (math anxiety). The effect was the same in the area of math anxiety per se.
The second study is Forman, E. M., Hoffman, K. L., McGrath, K. B., Herbert, J. D., Bradsma, L. L., & Lowe, M. R. (2007). A comparison of acceptance- and control-based strategies for coping with food cravings: An analog study. Behaviour Research and Therapy, 45(10), 2372-2386. They compared ACT to a traditional CBT program for those who were impacted at different levels by food. 98 participants with chocolate cravings were exposed to a well known CBT-based protocol (Kelly Brownell’s LEARN program) and an ACT-based protocol or no instructions and required to carry chocolate with them of for two days. Those highly impacted by food related cues ate less and had fewer cravings in the ACT condition. But those not impacted by food, did worse in the ACT condition than in the CBT condition (and both did worse than doing nothing at all).
It may not make that much sense to use a procedure like ACT with minor problems because the issues it raises are so fundamental. This could be proven wrong with data. But note that in the Zettle study, ACT worked better with highly experientially avoidant subjects than with low avoidant subjects; desensitization did not show that relationship; in the Forman study those with high food impact were helped by ACT but not those with low food impact. It is not a comparison to CBT but another study [Masuda, A., Hayes, S. C., Fletcher, L. B., Seignourel, P. J., Bunting, K., Herbst, S. A., Twohig, M. P., & Lillis, J. (2007). The impact of Acceptance and Commitment Therapy versus education on stigma toward people with psychological disorders. Behaviour Research and Therapy, 45(11), 2764-2772 found that ACT was not better than education in reducing mental health stigma significantly among participants who were relatively flexible and non-avoidant to begin with. For experientially avoidant and inflexible participants, however, ACT was much better.
It seems possible based on this line of reasoning that CBT might actually work better than ACT in more confined and minor areas; in more severe or chronic areas ACT, might work a bit better ... and perhaps all of that because more avoidant and inflexible folks will be more dominant in severe areas. That is not a conclusion -- it is too early to say -- but it is a guess based on a few studies so far. And remember that ACT is part of CBT -- when we say "CBT" here we mean CBT methods placed into the context of a traditional CBT model that basically focuses on the idea that thoughts cause emotions and behavior.
It helps to keep in mind that ACT is a model not just a package. All of the behavioral methods and some of the cognitive ones can easily be put into ACT protocols. They are still ACT when that happens if they fit the model. That is especially true with behavioral methods -- which are a node on that hexagon model of ACT.
But ultimately we will have to show that, for example, exposure from an ACT perspective is better than (or at least works through a different process than) exposure from a traditional CBT perspective. We have a couple of small studies that indicate that might be true (e.g., see Jill Levitt’s dissertation in Behavior Therapy, 2004) but not large RCTs on the question. Some of these are underway right now (such as in Michelle Craske’s lab) so in a few years we will know.
Is there much in traditional CBT that is helpful? Yes, of course, and virtually all of what is known to work at the level of components fits with the ACT model so these procedures can be used from an ACT perspective. The things that contradict an ACT model are not known to work as components, such a cognitive restructuring. But even there you can modify it to be more a matter of cognitive flexiblity.
Is the ACT model a better place to put all of these procedures? Let’s see. The answer will probably not be “yes, always.” Presumably it is more likely to be “sometimes yes, sometimes no.” But both the yes and no answers will move us forward, and that is the whole point, not silly name brand struggles.
Why to skeptics argue that there is a quite limited support for ACT while advocates seem to say otherwise?
Why to skeptics argue that there is a quite limited support for ACT while advocates seem to say otherwise?Some skeptics have not really read the whole literature and considered it carefully. Let's put these aside -- they are easy to detect and there is little to say about such criticism. What you then have left behind are two types. One are honest critics. These are very valuable and helpful people because they can light the way for additional research and development. The differences with honest critics so far seem to be in these areas.
Breadth of the criteria. The ACT / RFT community gives more weight to a model that is working than to RCTs alone. Mediational analyses, RFT progress, AAQ studies, component studies, experimental psychopathology, the like all weigh in very heavily. It is absolutely fair to let RCTs be the ultimate arbiter but if you pick them off one at a time with methodological worries, and focus only on DSM syndromes one at a time, even at ~120 RCTs you can see less support than people within the ACT / RFT community might believe is there. Over time, however, if the ACT / RFT community does its job, even that problem will be self-correcting because the development path being following includes randomized controlled trials as a centrally important area -- just not the only area.
The temporal measure of progress. Given the larger purpose of ACT / RFT, this harder set of criteria needs to be considered in terms of how hard the actual task is. The ACT / RFT community wants to be held to a high (amazingly high) standard, but this also means that judgments about accomplishment of such goals have to be made in the context of that stated purpose. This does mean that there is a certain prolonged sense of ambiguity. ACT / RFT research is more than 30 years old and critics can still doubt whether we are actually producing a more progressive psychology. That is fair, but then by the time the ACT / RFT community meets its goals to everyone's satisfaction, most folks in psychology and the behavioral sciences will know it, because these goals are so darned lofty.
Breadth of application. The ACT / RFT community think that the breadth of the model really matters, because the model itself claims to be about a deeper understanding of human cognition. In traditional syndromal treatment studies, the models are often quite narrow and breadth of application is not a fair test so when these folks look at ACT / RFT they don't quite know what to say. APA says we are over the bar only in chronic pain in terms of strong empirical support. Across the board the progress is more notable and the breadth of application is already pretty amazing but only now are good researchers in specific areas doing a deep dive -- modifying protocols and chasing process of change evidence. If the program succeeds there will be multiple studies of ACT / RFT applications within specific areas. Right now there are about 10 areas with at least 5 outcome studies, and nearly 20 areas with more that two (see the new book on "The ACT Research Journey" by Hooper and Larsson).
RCTs versus controlled time series designs. ACT comes from behavior analysis. If you eliminate time series designs in favor of only RCTs, the outcome data weaken, evne with nearly 120 RCTs and new RCTs now appearing every 2 weeks on average.
Quality of studies. Many ACT studies are put together by students and young faculty. Quite a number or from the developing world. Only a about 15 RCTs right now are funded. These early studies are often underpowered and the methodological bells and whistles are sometimes not there. Accord to a careful review by A-Tjak et al (in Psychotherapy and Psychosomatics, 2014) this is getting better, and we are starting to see replications with better controls. When you compare ACT to established CBT research from the best labs in the world, you are comparing research programs at two very different stages of development. We shall see what happens over time as funded ACT research becomes more common. However, average quality is a poor measure. A small study from, say, Iran is a wonderful thing to see ... how does any weaknesses pull down the more than 15 studies on ACT published in the Journal of Consulting and Clinical Psychology? You need to look to see if there are enough well done studies. You need to consider small studies that have specific weaknesses by looking at the whole literature. Knocking studies over one at a time means sturies with any flaws contribute nothing. That is, well, stupid. Average ratings means if you get students, or people without funding, or the developing world excited then you are necessarily weaker. That too is, well, stupid. Look at the whole literature and be responsible.
Published versus coming. ACT / RFT advocates often know about the data that are coming. We may know the researchers involved and feel that we can make some judgments. If you just look at publications (which an outside critic simply must do in order to be responsible) the picture looks different from the outside than it does from the inside. ACT / RFT research has been going on for 30 years, but it has only been visible for a few years, with the publication of the 1999 book on ACT and the 2001 book on RFT. About 75% of the outcome research is in the last 3 years. If the program is truly progressive, these differences will narrow over time however. If you want to get the recent meta-analyses and are a member go to the publications area. If you are not, then click here to join!
The reviews by Ost. Lar-Goran has been invited to ACT conferences many times to criticize the work. Some of his criticisms have been very useful. Others come from a different research tradition and don't have much appeal (e.g., the demand to focus only on syndromes; the insistance that only syndromal measure matter in outcomes). The other problem is that his two reviews have data problems. The first one (in 2008) attributed differences in methodological quality between ACT and CBT to the sloppiness of ACT studies. In fact, Brandon Gaudiano showed (see Gaudiano, 2009) that if you more collect data on funding the differences more carefully you see that all of these differences were due to funding. The study by Ost (in 2014) used ratings of methodological quality have not been replicated by others using the same scale (see the A-Tjak study; when Ost's rating were compared to this study on the same studies, Ost's were more against ACT and had an unacceptably low kappa of .35). The scale itself has several problems in my humble opinion but the A-Tjak study used a team approach for ratings that included ACT critics and ACT researchers, instead of using a single ACT critic and student raters. There were also over 80 factual or interpretive errors made in reading the ACT literature, which weaken the conclusions. A response article has been submitted to BRAT.
Bottom line. We think declaring that something is "evidence based" is a communitarian effort that should have the same open and agreed to standards that are carefully applied to all methods. APA has that ... and ACT is listed as evidence based in several areas. SAMHSA has that and ACT is listed in several areas there too. In the ACBS community we prefer to learn from our critics and keep on pursuing our vision and trying to get better.
Where is ACT and RFT going?
Where is ACT and RFT going?Everywhere that cognizing humans go. We want a theory of human behavior that allows us truly to make a difference in our homes, schools, workplace, and clinics. The ACT / RFT community wants it all: a technology that works, a theory that works, basic principles, AND a powerful linkage to our deepest human desires. But we can distinguish aspirations from data – and we have created a culture of openness and self-criticism that seems scientifically healthy. It is often that culture which seems most powerful when people first contact the ACT and RFT community. We are using ACT / RFT to create an ACT / RFT community that is open, non-hierarchical, diverse, committed, sharing, caring, and just plain fun. The vitality the young professionals and students as seen on this very website beg for the question: “what would happen if we worked together to create a community dedicated to the production of a psychology worthy of the human needs we are meant to address?” By appealing to the better nature of out clients (e.g., self-acceptance, mindfulness, values, commitment) we seem to be creating change in the clinic. Similarly, by raising our sites as professionals and creating a supportive, open, generous culture the same might happen in our training programs, clinics, and research teams. For those of us in the ACT / RFT / Contextual Psychology community we do not think that basic and applied science can safely stand apart. We seek the creation of a new empirical contextual psychology that carries forward and deepens our intellectual tradition, revitalizing basic psychology and linking our work to principles that help us address problems of human suffering and human growth. We want to see us create a psychology more adequate to the challenges of the human condition. This was part of the original vision of behavioral psychology and behavior therapy. Behavioral psychology lost its way over the issue of human cognition, and traditional CBT resulted, but perhaps we have found a way forward that will go beyond the excessively narrow goal of empirically evaluated technologies, to include also the two other aspects of our original tradition that were left behind: a firm link of application to basic principles, and an expansive vision of a form of psychology that can help create a better world in every area of human life. If we can do that, psychology itself may become more robust and useful. That is the vision.
- Posted 2005-07-31
How old is ACT?
How old is ACT?ACT is more than 40 years old.
The personal insight that led to ACT is described by Steve Hayes in this TEDx talk: bit.ly/StevesFirstTED. By his best memory, that moment on the carpet (you will understand that phrase if you see the talk) was in the winter of 1980-81. But that was just a transformational moment. ACT began to form in Steve's lab soon after. The lab members at the time included Robert Zettle ("the Z"), Zamir Korn, and Irwin Rosenfarb. The lab was jointly run with the late Aaron Brownstein, a basic behavior analyst.
The first ACT protocol was written by Steve in 1981. ACT was called "Comprehensive Distancing" -- the lab nickname for it was "Big D." You can find the protocol in the "History of ACT" daughter page of the "About ACT" section of the website.
The first actual ACT study was done in 1981-1982 and was presented at ABCT (then called AABT) in 1982:
Hayes, S. C., Korn, Z., Zettle, R. D., Rosenfarb, I., & Cooper, L. (November 1982). Rule‑governed behavior and cognitive behavior therapy: The effects of comprehensive cognitive distancing on pain tolerance. Paper presented at the meeting of the Association for Advancement of Behavior Therapy, Los Angeles.
Steve held back on publishing it despite its success, thinking that the implications were too large and thus outcome studies should not be a focus (especially randomized outcome studies) until its model and methods were better understood and idiographically tested. That is why this very first study was published 17 years later: Hayes, S. C., Bissett, R., Korn, Z., Zettle, R. D., Rosenfarb, I., Cooper, L., & Grundt, A. (1999). The impact of acceptance versus control rationales on pain tolerance. The Psychological Record, 49, 33-47. The only randomized outcome study published directly from the lab in this era was Rob Zettle's dissertation which came out in 1986.
The first ACT training was in 1982: Hayes, S. C. (October 1982). Cognitive distancing and psychopathology. Presentation to Broughton Hospital, Morganton, NC.
"Comprehensive distancing" seamlessly morphed into ACT as we think of it today. The first time "acceptance and commitment therapy" was used in the title of a talk was in 1991: Wilson, K. G., Khorakiwala, D., & Hayes, S. C. (May 1991). Change in Acceptance and Commitment Therapy. Paper presented at the meeting of the Association for Behavior Analysis, Atlanta. The first time it appeared in the title of a journal article was Hayes, S. C. & Wilson, K.G. (1994). Acceptance and Commitment Therapy: Altering the verbal support for experiential avoidance. The Behavior Analyst, 17, 289-303.
Is ACT based on behavior analysis?
Is ACT based on behavior analysis?Is the linkage between ACT and RFT post hoc?
Is the linkage between ACT and RFT post hoc?It has sometimes been said that the link between ACT and RFT is post hoc, but that is not the case. The basic, applied, and philosophical work co-evolved from the very beginning. In some areas of behavior analysis, applied work is based on animal work that is well worked out. Unfortunately, in the area of language and cognition the animal work never got there, so there was a more iterative process.
RFT began from a clinical lab that was trying to fill a need for a better basic analysis. The work went back and forth from basic to applied constantly. Many of the publications come out years later, so understanding the sequence of events requires a closer look at the record. For example Steele and Hayes, 1991 if the first undeniably RFT experimental study, but it was designed and conducted in 1985-86 and was the cap of a years long process of both basic and applied development.
Rob Zettle has written about this history. He was not just there but also created some of the key conceptual advances that lead to both ACT and RFT. The history is available in the publications area (search for Zettle, 2005). By the late 1970s we were getting frustrated with cognitive therapy / cognitive behavior therapy. We wrote a critical chapter on RET in 1979; we were doing conceptual work on rule-governance even that early. In 1981 a chapter interpreting CT from the point of view of rule-governed behavior was written -- it appeared in 1982. It too is on in the publications section (search for Zettle & Hayes, 1982). That chapter is concerned about rule-based insensitivity and undermining pliance; it breaks with Skinner on the definition of rules and do so in a way that demands RFT or something like it.
You can learn more from the actual earliest protocols. These are available here: https://contextualscience.org/ThreeEarliestACTProtocols
In that same year we were already doing the basic studies on rule-based insensitivity that would publish in the mid-80s. So we were already testing how rule produce psychological inflexibility. Studies were being planned to try to learn how to undermine that effect. The earliest ACT (nee “Comprehensive Distancing”) manual was drafted in that same year and the earliest applied tests were begun Probably the easiest way to document this is to look at papers presented orally in 1981-1982, since oral presentations overcome most of the distortions due to publication lags. Here is part of that list:
Hayes, S. C., Korn, Z., Zettle, R. D., Rosenfarb, I., & Cooper, L. (November 1982). Rule governed behavior and cognitive behavior therapy: The effects of comprehensive cognitive distancing on pain tolerance. AABT, Los Angeles.
Hayes, S. C., Zettle, R. D., & Rosenfarb, I. (May 1982). An empirical taxonomy of rule governed behavior. ABA, Milwaukee.
Hayes, S. C. (May 1982). Rule governed behavior and psychopathology. ABA, Milwaukee.
Hayes, S. C., Rosenfarb, I., & Zettle, R. D. (May 1982). Rule governed behavior and sensitivity to changing contingencies. ABA, Milwaukee.
Hayes, S. C. (May 1981). Rule governed behavior: Functional units of listener activity. ABA, Milwaukee.
Rosenfarb, I., Hayes, S. C., & Zettle, R. (May 1981). Self reinforcement: A social commitment analysis. ABA, Milwaukee.
Hayes, S. C. (November 1981). Running on empty: The ascendance of technical research. AABT, Toronto.
Thus, you can see that the experimental rule-governed studies on insensitivity; studies on commitment; conceptual work on rules; conceptual work linking rules to psychopathology; criticisms of CBT; philosophical work on the need for theory; and the earliest studies on ACT all emerged iteratively at the same time.
By 1984 the paper on Making Sense of Spirituality (Hayes, 1984 … you can find this in the publication list) makes it all clear what will come later. Self, deictic frames, defusion, flexibility and more are in there in one way or another. Shortly after that, the first RFT studies and the first ACT randomized trials began to appear.
RFT is far broader than ACT ... but it has been an ACT-RFT effort from the very beginning. This does not mean that ACT processes are in a point to point correspondence with RFT processes. Over time this is happening more and more, but linkages in each direction were created on the fly. The bottom line is this: the record shows that ACT, RFT, and contextualism are all part of one research and conceptual program that emerged at the same time and that have co-evolved for 25 years.
- S
Steven C. Hayes
What do I have to be to become certified as an ACT therapist?
What do I have to be to become certified as an ACT therapist?The ACT community has agreed not to set up our own therapist certification. There is a process to recognize ACT trainers. ACT trainers sign a values statement agreeing to make their training protocols available for low cost or no cost and agreeing not to make proprietary claims or to certify therapists.
Why reject therapist certification? Two reasons: it ossifies the method, and creates a hierarchy that cannot be readily dismantled. Instead, the ACT community provides ways to increasing sophistication and ability; conducts studies on training methods; and encourages all ACT therapists to constantly improve. On the website, therapists can list themselves as ACT therapists whenever they choose, but are asked to list their training experiences.
What is the role of intensive, experiential training in learning ACT?
What is the role of intensive, experiential training in learning ACT?What is the role of the eyes on exercise?
What is the role of the eyes on exercise?It has several functions but the bottom line is that it is the whole ACT model in one exercise Because it is uncomfortable but not dangerous it is a great context in which to practice defusion and acceptance. Its social nature heightens that part of it, since outright avoidance is relatively unlikely once people agree to do it. You can use psychological contact with the other as a metric of being present, so it gives feedback on the costs of fusion and avoidance. When these processes interfere the other person disappears Because self-as-context is social in origin, if the person running the exercise orients the participants to it you can contact the deictic basis of consciousness. The other person becomes somehow connected to you -- and yet you yourself contact a sense of transcendence in that social connection Because almost everyone values people, if you ask folks to use this as a physical metaphor for connection with others, it puts the mindfulness work (the work on acceptance, defusion, self, and the present) into a values context. You see how these processes support valued actions. It is a commitment exercise because you get agreement before hand; and again the social nature of it helps maintain the commitment And it is an exercise in psychological flexibility because it brings all of the other processes together in an unusual and repertoire expanding action It is the whole model in 10 minutes - Steve Hayes
ACT for the Public
ACT for the PublicWelcome to the For the Public section of this site!
We hope that you will find the information provided here on Acceptance and Commitment Therapy (ACT) useful in your journey of understanding and/or applying ACT to your life.
What is ACT?
Acceptance and Commitment Therapy (ACT) has developed as a behavioral intervention to help people learn strategies to live life more in the present, more focused on important values and goals, and less focused on painful thoughts, feelings and experiences. ACT teaches people how to engage with and overcome painful thoughts and feelings through acceptance and mindfulness techniques, to develop self-compassion and flexibility, and to build life-enhancing patterns of behavior. ACT is not about overcoming pain or fighting emotions; it's about embracing life and feeling everything it has to offer. It offers a way out of suffering by choosing to live a life based on what matters most. ACT has developed within a scientific tradition, and there continues to be a thriving research community that examines the basic science underlying ACT and the effectiveness of applying ACT techniques to numerous life problems such as anxiety, depression, PTSD, substance abuse, chronic pain, psychosis, eating problems, and weight management, just to name a few. While the other sections of this site are geared to professionals, you may wish to read more about ACT and Relational Frame Theory RFT (the basic contextual behavioral science of language and cognition on which ACT is based) as you continue interacting with the material. Simply come back and browse through the rest of the site at your leisure!
Resources and Support: ACT for Personal Growth
Many people find that learning from and with others is a great way to enact important life changes. We suggest one or more of the following may best meet your needs:
- Seeking a professional therapist with whom you feel comfortable
- Attending a professionally run therapy group
- Reading self-help books
- Joining the free ACT for the Public email listserv
- Finding others with whom to learn about and discuss applying ACT principles to your life
- ACBS members are encouraged to join the ACT for Professionals email listserv because once on this listserv you can ask virtually any question, or raise virtually any issue, and thousands of ACBS members will read it and you will almost always get thoughtful and helpful responses.
The links at the bottom of the page will walk you through the ways to seek out all of these different types of resources -- most of them from within this website. We have compiled this information in the hopes that it will be useful in guiding you to the right resources for you.
PLEASE NOTE: While research suggests that self-help books and other resources can be helpful for many people, professional psychotherapeutic services are often more interactive and tailored to your individual needs and therefore may be in your best interest. If you are already seeing a therapist, it is best to share with your therapist that you plan to seek additional resources in this community, and to share what you learn in this community so that he or she can better support your growth.
Tips for Seeking an ACT Therapist
Tips for Seeking an ACT TherapistLooking for a therapist who uses ACT strategies in your area? There are more therapists joining ACBS and becoming listed here each day, so check back frequently. Here is a searchable list to Find an ACT Therapist from within this site. If it doesn’t show an ACT therapist in your area, you may still be able to find one by other means. Some suggestions:
- Consult psychology, social work, and psychiatry departments at colleges or universities near you. Ask to speak to any members of the faculty or staff who are experts in behavior therapy, cognitive therapy, or clinical behavior analysis. Upon speaking to these experts, ask them if they have heard about ACT and know of any local ACT therapists.
- In countries besides the U.S., you may be able to contact similar organizations to try the strategy described above.
You can seek therapists through these other venues as well:
- The Association for Behavioral and Cognitive Therapies (ABCT) has a nation-wide database of PhD-level therapists, with searchable specialties (such as ACT) and by area. Visit www.abct.org and click "Find a Therapist".
- The National Association of Social Workers (NASW) has a nation-wide database of therapists licensed at the master's level (specializing in marriage and family therapy, health and wellness, aging, and more). Visit www.helpstartshere.org and click "Find a Social Worker".
You may wish to contact therapists in your area from these lists (above) to see if they use mindfulness and/or acceptance-based methods in their practice. You may find many that do, but do not specifically list themselves as ACT therapists. Research across therapeutic orientations suggests that the therapeutic relationship is an important agent for change, so we recommend that you seek a therapist with whom you feel comfortable and who is comfortable working with you and the issues you are bringing to therapy.
Connecting with Others
Connecting with OthersThere are two main ways to connect with others doing this work.
First, basic website use is free and open to anyone. ACBS members receive additional benefits.
Also, you may wish to join the For the Public email list. Here is a link to join. This email list is a general forum for public members reading ACT self-help books, working with an ACT therapist, or otherwise trying to apply ACT to their lives. Therapists, students and general members of the public all share their questions and personal experiences working with ACT principles on this list. It's free to join, and you can start posting questions right away as well as read older posts online. There are formal and informal groups formed through this email list who meet to discuss learning and applying ACT principles to their lives. These groups are not monitored or sponsored by ACBS, but they can be a great resource within which to learn and grow. You may wish to ask the Public listserv members for information about any groups in your area.
Self-Help Books
Self-Help BooksSelf-Help Books in English
Click here to see a list of ACT Self Help books.

Self-Help Books in Non-English Languages
Also, there are several self-help books written in other languages, as well as translations of Get Out Of Your Mind And Into Your Life, The Happiness Trap, and ACT On Life Not On Anger. Please click here for more information.
Information on Commonly Used Titles
Information on Commonly Used TitlesThese two books listed below are the most commonly discussed on the ACT for the Public Listserv.
 Get Out of Your Mind and Into Your Life offers a five-step plan for coping with painful emotions such as anxiety and depression. It teaches you how to learn life-enhancing behavior strategies that work to further the goals you value most. The realization that painful feelings cannot be controlled will open you to the possibility of fully emotional living. Once present, engaged, and aware, you can begin to build a new life for yourself filled with significance and meaning.
Get Out of Your Mind and Into Your Life offers a five-step plan for coping with painful emotions such as anxiety and depression. It teaches you how to learn life-enhancing behavior strategies that work to further the goals you value most. The realization that painful feelings cannot be controlled will open you to the possibility of fully emotional living. Once present, engaged, and aware, you can begin to build a new life for yourself filled with significance and meaning.
This self-help book was written for a general audience. If you or someone you love is struggling with getting out of your mind and onto a meaningful life path, this book is a great place to start.
Read this message from the author (Steve Hayes) regarding the use of Get Out of Your Mind and Into Your Life.
 The Happiness Trap: How to Stop Struggling and Start Living is the second self-help resource written for a wide-ranging audience and many find that it presents the ACT concepts in a clear, concise manner. Too many of us are caught in the happiness trap: we think that we should be happy all or most of the time, and we believe that we can control the circumstances of our lives in order to avoid unpleasant experiences. Using the principles of Acceptance and Commitment Therapy, Harris offers key concepts and specific techniques for escaping the “happiness trap” to create a full, rich, and meaningful life.
The Happiness Trap: How to Stop Struggling and Start Living is the second self-help resource written for a wide-ranging audience and many find that it presents the ACT concepts in a clear, concise manner. Too many of us are caught in the happiness trap: we think that we should be happy all or most of the time, and we believe that we can control the circumstances of our lives in order to avoid unpleasant experiences. Using the principles of Acceptance and Commitment Therapy, Harris offers key concepts and specific techniques for escaping the “happiness trap” to create a full, rich, and meaningful life.
There is also a companion website for this book maintained by the author, with additional resources you may find useful as you apply this approach to your life.
Free Practical Audio Exercises
Free Practical Audio ExercisesSix ACT Conversations
These audio files are easy-to-understand, excellent resources for walking through the ACT model step-by-step and learning how to apply it to your life. Each segment consists of multiple parts, so you may wish to do a little bit of the exercises at a time.
Visit 6 ACT Conversations at RMIT University in Australia for more information. The audio files and accompanying worksheets are available for downloading.
Mindfulness Practice Exercises
There are several exercises recorded as mp3 or other audio files available for free download. You may wish to save them and listen to them on a computer or personal mp3 player.
- 15-minute Awareness exercise by Jason Luoma
- Leaves on the Stream exercise by Jenna LeJeune
- Observer Exercise from the 1999 ACT book recorded by Randy Burgess
- Live Mindfully is a blog organized by Integrative Health Partners, a mindfulness and acceptance group practice, and provides over a dozen excellent mindfulness and ACT exercises to download for free.
- Excercises in Spanish (Ejercicios en Español) de Fabian Maero
- Free Audio Meditations with Dennis Tirch, Paul Gilbert or Laura Silberstein-Tirch
- ACT Guided Meditations by Lou Lasprugato - These same meditations can also be found freely via the app, Insight Timer, by searching "lasprugato" after downloading the app.
Free Videos: Learning About and Applying ACT
Free Videos: Learning About and Applying ACTThere are many free videos that can help you learn about ACT and begin to apply it to your life. The videos listed here are by no means a comprehensive list, and different therapists and clients may use different ways to illustrate or apply ACT principles.
These videos span a wide range of topics, from how to use ACT principles to cope with common problems to animated ACT exercises you can practice at home. Most of the videos are developed by ACT therapists, but some are made by clients to illustrate how they've applied ACT principles to their lives.
These videos were not created for or by ACBS, but we have put some together here from various sources. We hope that you find some of them useful.
Simply click on the links below to browse. If you are looking for videos about RFT, check out this list. Also, don't forget about the many videos available to logged in ACBS members here.
If you find others on Youtube or elsewhere, please let us know by Adding a Comment and include the URL for the video and we'll get it up for you.
Anger, Compassion, and What It Means To Be Strong | Russell Kolts | TEDxOlympia
Anger, Compassion, and What It Means To Be Strong | Russell Kolts | TEDxOlympiaWhile anger can feel powerful in our bodies, many of us use angry behavior to avoid dealing with things that make us uncomfortable. Compassion gives us a way to be strong that helps us courageously face the things that scare us—about the world, and about ourselves—and help make them better.
Russell is a licensed clinical psychologist and Professor of Psychology at Eastern Washington University, where he has taught for the past 16 years and has received numerous honors including twice being named the associated student body’s Faculty of the Year. Dr. Kolts has authored and coauthored numerous books and scholarly articles, including The Compassionate Mind Guide to Managing Your Anger, An Open Hearted Life: Transformative Lessons for Compassionate Living from a Clinical Psychologist and a Buddhist Nun (with Thubten Chodron), and the forthcoming Buddhist Psychology and CBT: A Practitioner’s Guide (with Dennis Tirch and Laura Silberstein). Dr. Kolts has pioneered the application of Compassion Focused Therapy (CFT) to the treatment of problematic anger and regularly conducts trainings and workshops on CFT.
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
Subtitles are available in: Arabic, Chinese, Italian, English, Japanese, and Serbian
Chessboard Metaphor
Chessboard MetaphorThis is a simple presentation of an ACT exercise commonly used in therapy that illustrates the difficulty with getting caught up in one's thoughts, as well as a way to change one's relationship to them.
DJ Moran, Ph.D. - Psychotherapy Academy
DJ Moran, Ph.D. - Psychotherapy AcademyHere are 4 videos from D.J. Moran, Ph.D. Transcripts are also available.
Eva Adriana Wilson, MD: The Strong and Healthy Self
Eva Adriana Wilson, MD: The Strong and Healthy SelfThe following is a 5 minute video with animations that focuses on the utility of distress in guiding valued living.
Hank Robb, Ph.D.: Being Where You Are and Doing What's Important
Hank Robb, Ph.D.: Being Where You Are and Doing What's ImportantDr. Hank Robb conducts an easy-to-follow introductory treatment session he calls "Being Where You Are and Doing What's Important" for this television series.
This is an excellent for a simple introduction on how ACT can be applied to your life.
Part 1
Our Psychological Landscape: Part 1 from Emily Rodrigues on Vimeo.
Part 2
Our Psychological Landscape: Part 2 from Emily Rodrigues on Vimeo.
Part 3
Our Psychological Landscape: Part 3 from Emily Rodrigues on Vimeo.
How do you turn the corner with anxiety?
How do you turn the corner with anxiety?This is an episode of a national television program in Australia called "Insight". This episode aired on November 6, 2018, on the topic of "Beating Anxiety".
Clients suffering with anxiety talk about the experiences and struggles with anxiety as well as different therapies they have tried.
Traditional CBT and ACT are featured centrally. Steven C. Hayes is a guest on this episode.
https://www.sbs.com.au/news/insight/tvepisode/beating-anxiety
Jason Luoma & Jenna LeJeune: The ACT Therapist
Jason Luoma & Jenna LeJeune: The ACT TherapistThe poem was created by Jason Luoma (http://www.drluoma.com) and Jenna LeJeune (http://www.portlandpsychotherapyclinic.com) as part of an Acceptance and Commitment Therapy conference in Australia. If you like the poem, come to an ACBS conference!
Joe Oliver: Demons on the Boat
Joe Oliver: Demons on the BoatThis is a simple, animated ACT metaphor for identifying and coping with difficult experiences. Animation by Joe Oliver.
Joe Oliver: The Unwanted Party Guest
Joe Oliver: The Unwanted Party GuestThis is another simple animated metaphor that illustrates one way to cope with difficult or unwanted experiences. Animation by Joe Oliver.
Jonathan Bricker: The willingness to crave
Jonathan Bricker: The willingness to crave Anonymous (not verified)Learning ACT - Skills and Competencies for Clinicians
Learning ACT - Skills and Competencies for CliniciansThese videos are from the Learning ACT DVD and expand upon excises and content covered in the book.
The first video serves as an introduction to the rest.
Living Well When You Don’t Feel Well - Joe Trunzo
Living Well When You Don’t Feel Well - Joe TrunzoLiving Well When You Don’t Feel Well: Overcoming Lyme Disease and Illness | Joe Trunzo | TEDxBryantU
Published on 5 Mar 2018
Trunzo highlights a different way of thinking and coping with diseases (and life), specifically Lyme. Dr. Trunzo earned his undergraduate degree in 1993 from Marywood University in Scranton PA and completed his graduate work in 2000 at Drexel University in Philadelphia, PA. He completed his pre-doctoral internship at the University of Vermont and his post-doctoral fellowship at the Centers for Behavioral & Preventive Medicine at Brown University Medical School in Providence, RI.
He is a Professor of Psychology and Chair of the Department of Applied Psychology at Bryant University. He is also a licensed, practicing clinical psychologist with expertise in the psychological management of chronic medical illnesses such as cancer and Lyme disease, as well as the treatment of mood and anxiety disorders, especially obsessive compulsive disorder.
He serves on several professional committees and belongs to a number of professional organizations. In his spare time, he enjoys being with his family, live music, running, and mountain climbing. This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at https://www.ted.com/tedx
Louise Gardner - Your ACT Auntie Series
Louise Gardner - Your ACT Auntie SeriesACT Videos
- ACT unhooking skills
- Be Like A Bendy Tree!
- The Doorway of Decisions
- SOS! The Human Mind from Your ACT Auntie
- Tug of war with a Monster
- What are values?
Mindful Moment Videos
Matthieu Villatte - Self as Context (Flexible Self)
Matthieu Villatte - Self as Context (Flexible Self)This video illustrates how to use hierarchical framing to build a sense of self as a context or container of all psychological experiences. The client feels split among the different roles of his life at the moment (new job, baby)
Mental Brakes to Avoid Mental Breaks | Steven Hayes | TEDxDavidsonAcademy
Mental Brakes to Avoid Mental Breaks | Steven Hayes | TEDxDavidsonAcademyHow can we best deal with difficult or negative thoughts? Dr. Steven Hayes discusses language, cognition, and the science behind putting on the mental brakes.
Steven C. Hayes is Nevada Foundation Professor at the Department of Psychology at the University of Nevada. An author of 41 books and more than 575 scientific articles, he has shown in his research how language and thought leads to human suffering, and has developed "Acceptance and Commitment Therapy" a powerful therapy method that is useful in a wide variety of areas. His popular book "Get Out of Your Mind and Into Your Life" was featured in Time Magazine among several other major media outlets and for a time was the number one best selling self-help book in the United States. Dr. Hayes has been President of several scientific societies and has received several national awards, such as the Lifetime Achievement Award from the Association for Behavioral and Cognitive Therapy.
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
Subtitles available in English and Italian
Mindfulness for Two - Experiential Role Plays
Mindfulness for Two - Experiential Role PlaysThe following are a series of experiential Role-Plays which accompany Kelly Wilson & Troy DuFrene's Mindfulness for Two.
Oliver, Christodoulou, & Whitfield: Passengers on the Bus -- metaphor animation
Oliver, Christodoulou, & Whitfield: Passengers on the Bus -- metaphor animationJoesph Oliver and colleagues, Vaso Christodoulou and Henry Whitfield worked alongside a youth media charity, Exposure, to develop this animation. This was done with the assistance of a grant from the British Association for Behavioural and Cognitive Psychotherapies (BABCP) ACT SIG. Exposure was set up to help kids who have had mental health problems get experience and find work within the media industry.
The animation is an allegory, telling the story of a bus driver, Tom, and his struggles with various passengers on his bus, as he heads his bus towards a life of meaning and vitality.
Enjoy!
Our Common Fate video - by Rikke Kjelgaard
Our Common Fate video - by Rikke KjelgaardThis video demonstrates our common humanity.
That every one of us experience unwanted thoughts and feelings.
Through processes of openness, awareness and engagement we can learn to hold these experiences lightly. We can learn to show ourselves, our inner and outer world both compassion and kindness while engaging in patterns of meaningful and vital behaviours.
This video is made with much appreciated contributions by trainers and trainees in Acceptance and Commitment Therapy (ACT).
***
The rejection of our common fate makes us strangers to each other.
The election of that fate, in love, reveals us as one body.
Sebastian Moore
***
Thank you Robyn Walser and Kelly Wilson for your inspiration and contribution to ACT and to my life and practice and to this movie.
-Rikke Kjelgaard
***
Music by Coldplay
Pain Management Programmes 2017 Glasgow Conference: Plenary Session 3 - The Great ACT Debate
Pain Management Programmes 2017 Glasgow Conference: Plenary Session 3 - The Great ACT DebatePain Management Programme 2017 Glasgow Conference
16th Biennial National Conference
Glasgow Caledonian University, Glasgow, Scotland
14th and 15th September 2017
Plenary Session 3 - The Great ACT Debate - "ACT: best thing since sliced bread or the Emperor’s new clothes?"
David Gillanders and James Coyne
Psychological flexibility: How love turns pain into purpose | Steven Hayes | TEDxUniversityofNevada
Psychological flexibility: How love turns pain into purpose | Steven Hayes | TEDxUniversityofNevadaWhat can we do to prosper when facing pain and suffering in our lives? More than a thousand studies suggest that a major part of the answer is learning psychological flexibility. Steven C. Hayes is one of the researchers who first identified that process and put it into action in the form of a popular acceptance and mindfulness method called Acceptance and Commitment Therapy. In this emotional talk, Hayes distills the essence of psychological flexibility down into a few easy to understand sentences. He takes viewers through a harrowing journey into his own panic disorder, to the very moment in his life when he made this life changing choice: I will not run from me. Hayes shows how making that choice allows us to connect with our own deep sense of meaning and purpose, arguing that taking a loving stance to your own pain allows you to bring love and contribution into the world.
Steven C. Hayes is Nevada Foundation Professor at the Department of Psychology at the University of Nevada. An author of 38 books and more than 540 scientific articles, he has shown in his research how language and thought leads to human suffering, and has developed “Acceptance and Commitment Therapy” a powerful therapy method that is useful in a wide variety of areas. His popular book “Get Out of Your Mind and Into Your Life” was featured in Time Magazine among several other major media outlets and for a time was the number one best selling self-help book in the United States. Dr. Hayes has been President of several scientific societies and has received several national awards, such as the Lifetime Achievement Award from the Association for Behavioral and Cognitive Therapy.
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
Subtitles available in Dutch, English, Finnish, German, Greek, Italian, Japanese, Persian, Polish, Portuguese, Romanian, Russian, Spanish, and Swedish
Rich Blonna, Ph.D.: A Brief Introduction to ACT
Rich Blonna, Ph.D.: A Brief Introduction to ACTThis very brief introduction to ACT spells out the different components of the ACT work.
Russ Harris, MD: About ACT in simple terms
Russ Harris, MD: About ACT in simple termsIn this 30 minute interview with Australian motivational speaker Zara, Dr. Harris discusses ACT in simple terms and how he's applied it in his own life.
Self-Help Plus - Stress Management
Self-Help Plus - Stress ManagementWorld Health Organization's Self Help Plus (SH+) program - shown in 3 RCTs not only to reduce PTSD and depression, but also to prevent the onset of mental illness in those at risk.
- SH+ manual and audio files in English
Self-Help Plus (SH+) is WHO’s 5-session stress management course for large groups of up to 30 people. It is delivered by supervised, non-specialist facilitators who complete a short training course and use pre-recorded audio and an illustrated guide (Doing What Matters in Times of Stress - available in over 20 different languages) to teach stress management skills. The course is suitable for adults who experiences stress, wherever they live and whatever their circumstances. It has been shown to reduce psychological distress and prevent the onset of mental disorders. The format of SH+ makes it well-suited for use alongside other mental health interventions, as a first step in a stepped care programme, or as a community intervention delivered alongside broader community programming.
- Check out this free webinar of WHO's Self Help PlusACT protocol for refugees presented by: Russ Harris and Claudette Foley. They answer Frequently Asked Questions about the protocol – AKA “Self-help Plus” - and explore how to implement it.
Shamash Alidina ACT Training Videos
Shamash Alidina ACT Training VideosMr. Shamash Alidina has shared some videos on Acceptance and Commitment Training.
Here's the link: https://youtube.com/playlist?list=PLFqEhpJvR7lfJfhGFXSPQmRxfHI_mb9ba
The ACT Matrix 101 Videos by Kevin Polk, Ph.D.
The ACT Matrix 101 Videos by Kevin Polk, Ph.D. Kevin PolkThe OCD Mind and Uncertainty | ACT
The OCD Mind and Uncertainty | ACTA brief introductory video to help clients with OCD who are struggling with uncertainty and the urges OCD can bring about.
Submitted by Annabella Hagen
The secret to self control | Jonathan Bricker | TEDxRainier
The secret to self control | Jonathan Bricker | TEDxRainierJonathan Bricker's work has uncoved a scientifically sound approach to behavior change that is twice as effective as most currently practiced methods. His new methods are driving new norms and new apps for how people quit smoking and decrease obesity, saving many people from an early death.
Jonathan Bricker is an internationally recognized scientific leader in a bold approach called acceptance and commitment therapy. A Stanford researcher called his use of the approach “a breakthrough in behavioral research [that] has major public health implications for the major causes of preventable death.” Bricker and his team, having received $10 million in total federal research grants to study this topic, are rigorously testing this intervention on multiple platforms, including smartphone apps, websites, and telephone coaching. His SmartQuit app for quitting smoking was recently launched and is now in distribution worldwide.
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
Subtitles available in English, French, German, Italian, Japanese, Korean, and Spanish
Thoughts on the future of ACBS and contextual psychology - 2016 - Steven Hayes & Barbara Gil-Luciano
Thoughts on the future of ACBS and contextual psychology - 2016 - Steven Hayes & Barbara Gil-LucianoSteven Hayes, University of Nevada, & Bárbara Gil-Luciano, Madrid Institute of Contextual Psychology
Some thoughts on the future of ACBS and contextual science from Steven Hayes. (recorded June 2016)
¿Cuál es el futuro de la CBS (Contextual Behavioral Science - Ciencia Contextual) y hacia dónde crees que se dirige la Psicología Contextual? Entrevista a Steven Hayes
subtitulado en español
Tom Lavin, MFT, LCADC, ACATA: : When Life Hurts - Meaning Can Provide Strength and Direction
Tom Lavin, MFT, LCADC, ACATA: : When Life Hurts - Meaning Can Provide Strength and Direction
When Life Hurts: Meaning can Provide Strength and Direction
Acceptance and Commitment Therapy/Logotherapy Perspective
Presented by Tom Lavin, MFT, LCADC, ACATA
Psychotherapist
Tom Lavin, MFT, LCADC, ACATA: Live Better Psychoeducation Series
Tom Lavin, MFT, LCADC, ACATA: Live Better Psychoeducation SeriesACT: Live Better Psychoeducation Series
The intention of the “Live Better Series” is to provide life perspectives and life enhancement skills to encourage and support people in living vital and meaningful lives.
The “Live Better Series” examines and explores what Dr. Salvatore R. Maddi found to be three essential life attitudes in developing stress hardiness-resiliency:
1. Commitment Attitude: strive to be engaged rather than isolated
2. Control Attitude: be engaged in influencing outcomes, rather than lapse into passivity and powerlessness
3. Challenge Attitude: view stressful situations as opportunities to learn and grow and live one’s values
In cultivating these three resiliency fostering attitudes, the psychoeducation series is based on the core principles of Dr. Steven C. Hayes’ Acceptance and Commitment Therapy:
1. Acceptance of what is
2. Identifying and then choosing and committing to personally meaningful values
3. Taking action on living a life based on one’s identified core values
Complimentary to the core principles of ACT, the series integrates the three essential elements of Dr. Viktor Frankl’s Logotherapy, a therapy based on the fundamental human desire to live a meaningful life:
1. Creative Values: identifying and manifesting one’s talents and gifts to contribute to life
2. Experiential Values: actively engaging with those elements of life that inspire and nurture one’s spirit
3. Attitudinal Values: adopt a self-transcendent attitude: responding with grace , courage , and wisdom in the face of inescapable suffering
Tom Lavin MFT, LCADC, ACATA, the recipient of the 2014 IMPACT AWARD of the Association for Contextual Behavioral Science, is the primary instructor.
Co-presenters for the series include Drs. Steven C. Hayes, Kelly Wilson, Victoria Follette, and Nicole Pavlatos.
****Worksheets that accompany each class are available here.
Tom Lavin, MFT, LCADC, ACATA: New Skills for Living - Experts on using ACT in daily life
Tom Lavin, MFT, LCADC, ACATA: New Skills for Living - Experts on using ACT in daily lifeTom Lavin, MFT, LCADC has hosted the local ABC affliate television show in Reno, NV titled New Skills for Living, a health and wellness series, since 1995 in an effort to help people learn skills to live vital and meaningful lives.
Tom is the recipient of the 2014 IMPACT AWARD of the Association for Contextual Behavioral Science.
You can see expert ACT therapists discuss how ACT principles can be applied to so many aspects of your life!
Topics: ACT in Daily Life, Anxiety, Addiction, Chronic Illness, PTSD, Eating Disorders, Mindfulness for College Students, Families and Addiction Recovery, Smoking Cessation, Valued-Based Living, Happy Couples, Autism, Meaningful Living, etc.
Each of the videos are approximately 20-30 minutes in length.
Visit easeap.com for more information.
"ACT in Daily Life", Steven C. Hayes, PhD
"ACT: Anxiety" Steven C. Hayes, PhD
"ACT: Addressing Addiction" Steven C. Hayes, PhD
"ACT Addressing Chronic Illness" Steven C Hayes, PhD
"Mindfulness for College Students" Jacqueline Pistorello, PhD
"ACT: PTSD" Jacqueline Pistorello, PhD
"ACT: Anxiety" Kelly G. Wilson, PhD
"ACT: PTSD Treatment" Victoria Follette, PhD
"Stop Smoking" Jonathan Bricker, PhD
"Happy Couples" Robyn D. Walser, PhD
"Living Values Makes a Difference" Jennifer C. Plumb, MA
"Effective Psychotherapy" Tom Lavin, MFT, LADC
"Help for People with Eating Disorders" Jason Lillis, PhD
"ACT Therapy for Substance Abuse and Disordered Eating" Lindsay B. Fletcher, MA
"Principles of Vital Living" Tom Lavin, MFT, LADC
"How Families Can Deal with Financial and Relationship Stress" Tom Lavin, MFT, LADC
"Addiction and Family Recovery" Tom Lavin, MFT, LADC
"ACT: Autism" Nanni Presti, MD, PhD
"Addiction Recovery" Barbara Kohlenberg, PhD
"When Life Hurts: ACT and Logotherapy" Tom Lavin, MFT LADC
The link below connects to my April, 2026 presentation to Nevada Physicians on developing resiliency and living a vital, meaningful life. The webinar was sponsored by the Nevada Physician Wellness Coalition.
It's linked here
Physicians were encouraged to not only listen for how they can use this information to support their patients’ health and well-being but, also, how they can apply this information to address their personal stress/burnout and enhance the quality of their lives.
Topics addressed include:
1.Identify your personal stress symptoms
2.Apply the Stress Iceberg concept to identify what may be causing your stress
3.Personally apply how to use the diathesis stress model in understanding how cumulative stress and maladaptive coping might be affecting your health and quality of your life
4.Understand how to use the core principles of Acceptance and Commitment Therapy to respond rather than react to stress
5.Participate in a brief ACT informed meditation
6.Apply the paradigm of Vision-Decision-Action in clarifying values and virtues and committing to becoming the “person I aspire to be and living the life I aspire to live”
7.Personally apply the three venues of living a meaningful life as articulated in Logotherapy
8.Personally identify and commit to living a physically and emotionally flourishing life by addressing Stress Iceberg “under the water level” distresses of resentment/forgiveness, guilt/amends, prioritizing and simplifying life, making the most of each day
Resources for Learning More about ACT
Resources for Learning More about ACTFirst check out the Resources for Learning About ACT.
See the list of ACT books.
To understand more of the ACT langauge and concepts, check out the ACT Glossary of Terms.
To gain a deeper understanding about ACT and it's intellectual foundations, you may wish to browse through this section of the site: www.contextualscience.org/basic_foundations. The topics presented here are written with professionals in mind, but it is a good starting place for learning more about the roots of ACT.
A Note on the Research Supporting ACT
A Note on the Research Supporting ACTYou may be wondering about how effective ACT is when studied carefully. It takes quite a lot to become what is called an "empirically supported treatment"; meaning that a number of rigorous research studies indicate that the treatment has been shown to be effective for helping people cope with a particular problem. As of January 2026, more than 20 organizations worldwide recommend ACT for depression, anxiety, stress, chronic pain, OCD, substance abuse, addiction, psychosis, and coping with chronic illness such as tinnitus and multiple sclerosis. Organizations recommend ACT to treat children and adolescents for anxiety, depression, pain, and OCD.
As of January 2026, there are over 1,450 ACT Randomized Controlled Trials and over 600 peer reviewed assessments of the ACT evidence base. These studies have examined ACT's effectiveness in many research areas, such as depression, anxiety, stress, OCD, substance abuse, addiction, psychosis, schizophrenia, eating disorders, body image disorders, weight loss, sports performance, trauma, insomnia, procrastination, and in coping with health conditions such as chronic pain, tinnitus, multiple sclerosis, cancer, brain injury, bowel diseases, headaches, and migraines.
Researchers have done a considerable amount of research that shows that the individual processes within ACT can be helpful across problems, and researchers care about ensuring that the treatment you get is likely to be helpful for the particular problem(s) for which you seek help.
ACT TEDTalks
ACT TEDTalks Emanuele RossiDirect Links to International Subtitles
Direct Links to International SubtitlesArabic
TED Olympia _ الغضب والتعاطف ومعنى أن تكون قوياً _ راسل كولتز
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=ar
السر وراء التحكم فى النفس | جوناثان بريكر | TEDxRainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=ar
خلق تواصل إستثنائي- ماڤيس تساي TEDxEverett
https://www.youtube.com/embed/B9kg1UdzDvw?cc_load_policy=1&cc_lang_pref=ar
TED _ موهبة الشجاعة العاطفية وتأثيرها _ سوزان ديفد
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=ar
لماذا من الصعب أن نكون بشرا | جون فورسيث | TEDxUnionCollege
https://www.youtube.com/embed/zo-CaG0A1Xs?cc_load_policy=1&cc_lang_pref=ar
قوة الصغر | اشلينغ ليونارد كورتين | TEDxBallyroanLibrary
https://www.youtube.com/embed/w4WpBax7rJU?cc_load_policy=1&cc_lang_pref=ar
Bulgarian
Дарбата и силата на емоционалния кураж
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=bg
Chinese Simplified
避免精神崩溃的精神刹车 | Steven Hayes | TEDxDavidsonAcademy
https://www.youtube.com/embed/GnSHpBRLJrQ?cc_load_policy=1&cc_lang_pref=zh-CN
愤怒,同情,以及它意味着什么是强 | Russell Kolts | TEDxOlympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=zh-CN
情感勇气的礼物和力量 | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=zh-CN
为什么做人那么难?| 约翰 · 福赛斯 | TEDxUnionCollege
https://www.youtube.com/embed/zo-CaG0A1Xs?cc_load_policy=1&cc_lang_pref=zh-CN
Chinese Traditional
情感勇氣的禮物和力量 | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=zh-TW
為什麼做人那麼難 | 約翰.福賽斯( John Forsyth) | TEDxUnionCollege
https://www.youtube.com/embed/zo-CaG0A1Xs?cc_load_policy=1&cc_lang_pref=zh-TW
Danish
Modet til at føle | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=da
Dutch
Psychologische flexibiliteit: je pijn wijst je de weg | Steven Hayes | TEDx University of Nevada
http://bit.ly/SteveTED1-cc-Nederlands
De gave en kracht van emotionele moed | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=nl
English
Psychological flexibility: How love turns pain into purpose | Steven Hayes | TEDxUniversityofNevada
http://bit.ly/SteveTED1-cc-English
Mental Brakes to Avoid Mental Breaks | Steven Hayes | TEDxDavidsonAcademy
http://bit.ly/SteveTED2-cc-English
The secret to self control | Jonathan Bricker | TEDxRainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=en
Anger, Compassion, and What It Means To Be Strong | Russell Kolts | TEDxOlympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=en
Create Extraordinary Interactions | Mavis Tsai | TEDxEverett
https://www.youtube.com/embed/B9kg1UdzDvw?cc_load_policy=1&cc_lang_pref=en
The gift and power of emotional courage | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=en
Why it's hard being human | John Forsyth | TEDxUnionCollege
https://www.youtube.com/embed/zo-CaG0A1Xs?cc_load_policy=1&cc_lang_pref=en
Living Well When You Don’t Feel Well: Overcoming Lyme Disease and Illness | Joe Trunzo | TEDxBryantU
https://www.youtube.com/embed/keC6R-Qtb_M?cc_load_policy=1&cc_lang_pref=en
The Power of Small | Aisling Leonard-Curtin | TEDxBallyroanLibrary
https://www.youtube.com/embed/w4WpBax7rJU?cc_load_policy=1&cc_lang_pref=en
Finnish
Psykologinen joustavuus: Kuinka rakkaus kääntää tuskan tarkoitukseksi | Steven Hayes | TEDx University of Nevada
http://bit.ly/SteveTED1-cc-Suomalainen
French
La flexibilité psychologique : comment l'amour fait de la douleur une raison d'être | Steven Hayes | TEDx University of Nevada
https://www.youtube.com/embed/o79_gmO5ppg?cc_load_policy=1&cc_lang_pref=fr
Le secret de la maitrise de soi | Jonathan Bricker | TEDx Rainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=fr
Le don et le pouvoir du courage émotionnel | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=fr
Pourquoi est-ce si difficile d'être un être humain | John Forsyth | TEDxUnionCollege
https://www.youtube.com/embed/zo-CaG0A1Xs?cc_load_policy=1&cc_lang_pref=fr
German
Psychologische Flexibilität: Wie Liebe Schmerz in existenzielle Bestimmung verwandelt | Steven Hayes | TEDxUniversityofNevada
http://bit.ly/SteveTED1-cc-Deutsch
Mentale Bremsen verhindern mentale Zusammenbrüche | Steven Hayes | TEDx Davidson Academy
http://bit.ly/SteveTED2-cc-Deutsch
Das Geheimnis der Selbstkontrolle | Jonathan Bricker | TEDx Rainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=de
Ärger, Mitgefühl und was es bedeutet, stark zu sein | Russell Kolts | TEDxOlympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=de
Die Gabe und Kraft gefühlsbestimmten Mutes | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=de
Greek
Ψυχολογική ευελιξία: Πώς η αγάπη μετατρέπει τον πόνο σε σκοπό | Στίβεν Χέιζ | TEDx University of Nevada
http://bit.ly/SteveTED1-cc-ελληνικά
Θυμός, συμπόνια και τι σημαίνει να είσαι δυνατός | Russell Kolts | TEDxOlympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=el
Δημιουργήστε εξαιρετικές αλληλεπιδράσεις | Mavis Tsai | TEDxEverett
https://www.youtube.com/embed/B9kg1UdzDvw?cc_load_policy=1&cc_lang_pref=el
Το δώρο και η δύναμη του συναισθηματικού κουράγιου
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=el
Hebrew
המתנה והכח של אומץ רגשי | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=iw
Hungarian
Pszichénk rugalmassága : Hogyan változtathatja a szeretet, a fájdalmat motivációvá? | Steven Hayes | TEDx University of Nevada
https://www.youtube.com/embed/o79_gmO5ppg?cc_load_policy=1&cc_lang_pref=hu
Az érzelmi bátorság adománya és hatalma | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=hu
Italian
Flessibilità Psicologica: come l'amore dà senso alla sofferenza | Steven Hayes | TEDx University of Nevada
http://bit.ly/SteveTED1-cc-Italiano
Freni mentali per evitare crolli mentali | Steven Hayes | TEDx Davidson Academy
http://bit.ly/SteveTED2-cc-Italiano
Il segreto dell'autocontrollo | Jonathan Bricker | TEDx Rainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=it
Rabbia, compassione e cosa significa essere forti | Russell Kolts | TEDx Olympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=it
Il dono e la forza del coraggio emozionale | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=it
Il potere delle piccole cose | Aisling Leonard Curtin | TEDxBallyroanLibrary
https://www.youtube.com/embed/w4WpBax7rJU?cc_load_policy=1&cc_lang_pref=it
Japanese
心理的柔軟性: 愛がどうやって痛みを目的に変えるか | スティーブン ヘイズ | TEDx University of Nevada(ネバダ大学)
http://bit.ly/SteveTED1-cc-日本語
ネガティブな感情をスローダウンする方法|スティーヴン·ヘイズ|TEDxDavidsonAcademy(デビットソン·アカデミー)
http://bit.ly/SteveTED2-cc-日本語
セルフコントロールの秘訣 | ジョナサン·ブリッカー | TED× Rainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=ja
怒りと思いやり、そして強くなることの意味 | ラッセル·コルツ | TEDx Olympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=ja
感情に向き合う勇気の力と素晴らしさ | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=ja
Korean
자기 통제의 비밀 | 조나단 브릭커 (Jonathan Bricker ) | TEDx Rainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=ko
특별한 교감 나누기 | 마비스 차이(Mavis Tsai) | TEDxEverett
https://www.youtube.com/embed/B9kg1UdzDvw?cc_load_policy=1&cc_lang_pref=ko
자신의 감정을 마주할 수 있는 용기 (Susan David) | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=ko
작은 것의 힘 | 애슐링 레오나르드 커틴(Aisling Leonard-Curtin) | TEDxBallyroanLibrary
https://www.youtube.com/embed/w4WpBax7rJU?cc_load_policy=1&cc_lang_pref=ko
Macedonian
Mental Brakes to Avoid Mental Breaks | Steven Hayes | TEDxDavidsonAcademy
http://bit.ly/SteveTED2-cc-македонски
Дарот и моќта на храброста | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=mk
Marathi
भावनिक धैर्य: एक ताकद, तशीच देणगीही. | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=mr
Persian
انعطاف پذیری روانشناختی : چگونه عشق، درد انسان را به هدف و معنا سوق میدهد
http://bit.ly/SteveTED1-cc-فارسی
ترمزهای ذهنی برای دوری از درهم شکستن روانی | استیو هیز | TEDxDavidsonAcademy
http://bit.ly/SteveTED2-cc-فارسی
موهبت و قدرت شهامت عاطفی | سوزان دیوید | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=fa
Polish
Elastyczność psychologiczna: Jak miłość zmienia ból w powołanie| Steven Hayes | TEDx University of Nevada
http://bit.ly/SteveTED1-cc-Polskie
Dar i moc emocjonalnej odwagi | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=pl
Portuguese
O dom e o poder da coragem emocional | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=pt-PT
Portuguese, Brazilian
Flexibilidade psicológica: como o amor transforma a dor em propósito | Steven Hayes | TEDx Universidade de Nevada
http://bit.ly/SteveTED1-cc-Portugues
https://www.youtube.com/embed/o79_gmO5ppg?cc_load_policy=1&cc_lang_pref=pt-BR
Raiva, compaixão e o que significa ser forte | Russell Kolts | TEDxOlympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=pt-BR
O segredo do autocontrole | Jonathan Bricker | TEDxRainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=pt-BR
Create Extraordinary Interactions | Mavis Tsai | TEDxEverett
https://www.youtube.com/embed/B9kg1UdzDvw?cc_load_policy=1&cc_lang_pref=pt-BR
O dom e o poder da coragem emocional | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=pt-BR
O poder do pequeno | Aisling Leonard-Curtin | TEDxBallyroanLibrary
https://www.youtube.com/embed/w4WpBax7rJU?cc_load_policy=1&cc_lang_pref=pt-BR
Romanian
Flexibilitatea psihologică. Cum iubirea transformă durerea în scop | Steven Hayes | TEDx University of Nevada
http://bit.ly/SteveTED1-cc-Română
Darul și puterea curajului emoțional | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=ro
Russian
Психологическая гибкость: Как боль превращается в цель благодаря любви | Steven Hayes | TEDxUniversityofNevada
http://bit.ly/SteveTED1-cc-русский
Секрет самоконтроля | Джонатан Брикер | TEDxRainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=ru
Создание экстраординарных взаимодействий | Мавис Цай | TEDxEverett
https://www.youtube.com/embed/B9kg1UdzDvw?cc_load_policy=1&cc_lang_pref=ru
Дар и сила эмоциональной смелости | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=ru
Гнев, сострадание и что значит быть сильным | Рассел Колтс | TEDxOlympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=ru
Serbian
Bes, saosećajnost i šta znači biti jak | Rasel Kolts (Russell Kolts) | TEDx Olympia
https://www.youtube.com/embed/QG4Z185MBJE?cc_load_policy=1&cc_lang_pref=sr
Dar i snaga emocionalne hrabrosti | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=sr
Spanish
Flexibilidad psicológica: Como el amor convierte el dolor en propósito | Steven Hayes | TEDx University of Nevada
http://bit.ly/SteveTED1-cc-Español
Frenos mentales para evitar daños mentales | Steven Hayes | TEDx Davidson Academy
http://bit.ly/SteveTED2-cc-Español
El secreto del autocontrol | Jonathan Bricker | TEDx Rainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=es
Create Extraordinary Interactions | Mavis Tsai | TEDxEverett
https://www.youtube.com/embed/B9kg1UdzDvw?cc_load_policy=1&cc_lang_pref=es
El don y el poder del coraje emocional | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=es
Por qué es difícil ser humano | John Forsyth | TEDxUnionCollege
https://www.youtube.com/embed/zo-CaG0A1Xs?cc_load_policy=1&cc_lang_pref=es
Swedish
Psykologisk flexibilitet: Hur kärlek förvandlar smärta till mening | Steven Hayes | TEDxUniversityofNevada
http://bit.ly/SteveTED1-cc-Svenska
Turkish
Psikolojik esneklik: Aşk acıyı nasıl amaca dönüştürür? | Steven Hayes | TEDx University of Nevada
https://www.youtube.com/embed/o79_gmO5ppg?cc_load_policy=1&cc_lang_pref=tr
Kendini kontrol etmenin sırrı | Jonathan Bricker | TEDxRainier
https://www.youtube.com/embed/tTb3d5cjSFI?cc_load_policy=1&cc_lang_pref=tr
Duygusal cesaret yetenek ve gücü | Susan David | TED
https://www.youtube.com/embed/NDQ1Mi5I4rg?cc_load_policy=1&cc_lang_pref=tr
Vietnamese
Cách tạo nên những mối liên kết kỳ diệu - Mavis Tsai | TEDxEverett
https://www.youtube.com/embed/B9kg1UdzDvw?cc_load_policy=1&cc_lang_pref=vi
Anger, Compassion, and What It Means To Be Strong | Russell Kolts
Anger, Compassion, and What It Means To Be Strong | Russell KoltsWhile anger can feel powerful in our bodies, many of us use angry behavior to avoid dealing with things that make us uncomfortable. Compassion gives us a way to be strong that helps us courageously face the things that scare us—about the world, and about ourselves—and help make them better.
 Russell is a licensed clinical psychologist and Professor of Psychology at Eastern Washington University, where he has taught for the past 16 years and has received numerous honors including twice being named the associated student body’s Faculty of the Year. Dr. Kolts has authored and coauthored numerous books and scholarly articles, including The Compassionate Mind Guide to Managing Your Anger, An Open Hearted Life: Transformative Lessons for Compassionate Living from a Clinical Psychologist and a Buddhist Nun (with Thubten Chodron), and the forthcoming Buddhist Psychology and CBT: A Practitioner’s Guide (with Dennis Tirch and Laura Silberstein). Dr. Kolts has pioneered the application of Compassion Focused Therapy (CFT) to the treatment of problematic anger and regularly conducts trainings and workshops on CFT.
Russell is a licensed clinical psychologist and Professor of Psychology at Eastern Washington University, where he has taught for the past 16 years and has received numerous honors including twice being named the associated student body’s Faculty of the Year. Dr. Kolts has authored and coauthored numerous books and scholarly articles, including The Compassionate Mind Guide to Managing Your Anger, An Open Hearted Life: Transformative Lessons for Compassionate Living from a Clinical Psychologist and a Buddhist Nun (with Thubten Chodron), and the forthcoming Buddhist Psychology and CBT: A Practitioner’s Guide (with Dennis Tirch and Laura Silberstein). Dr. Kolts has pioneered the application of Compassion Focused Therapy (CFT) to the treatment of problematic anger and regularly conducts trainings and workshops on CFT.
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
Create Extraordinary Interactions | Mavis Tsai
Create Extraordinary Interactions | Mavis TsaiOur ability to form close connections is not only at the core of our mental health, but interpersonal closeness helps us live longer. Mavis Tsai presents the components of an extraordinary interaction and six powerful questions you can share with others to create unforgettable conversations.
 Mavis Tsai, Ph.D., is a clinical psychologist/research scientist and Associate Director of University of Washington’s Center for Science of Social Connection. She has gained a world-wide following as the co-creator of Functional Analytic Psychotherapy (FAP), a contextual behavioral and relational therapy that harnesses the power of the therapeutic relationship to transform clients’ lives. She is the co-author/editor of five text books on FAP (some of which have been translated into Portuguese, Spanish, Japanese and Italian) and over 60 articles and book chapters. She received Washington State Psychological Association’s 2014 Distinguished Psychologist Award in recognition of outstanding contributions to knowledge in clinical psychology. Her most recent and passionate work is in training volunteers in five continents to launch Live with Awareness, Courage and Love Meetups, which address the need for people to connect more authentically with themselves and with others, and to spread the
Mavis Tsai, Ph.D., is a clinical psychologist/research scientist and Associate Director of University of Washington’s Center for Science of Social Connection. She has gained a world-wide following as the co-creator of Functional Analytic Psychotherapy (FAP), a contextual behavioral and relational therapy that harnesses the power of the therapeutic relationship to transform clients’ lives. She is the co-author/editor of five text books on FAP (some of which have been translated into Portuguese, Spanish, Japanese and Italian) and over 60 articles and book chapters. She received Washington State Psychological Association’s 2014 Distinguished Psychologist Award in recognition of outstanding contributions to knowledge in clinical psychology. Her most recent and passionate work is in training volunteers in five continents to launch Live with Awareness, Courage and Love Meetups, which address the need for people to connect more authentically with themselves and with others, and to spread the
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
Living Well When You Don’t Feel Well: Overcoming Lyme Disease and Illness | Joe Trunzo
Living Well When You Don’t Feel Well: Overcoming Lyme Disease and Illness | Joe TrunzoTrunzo highlights a different way of thinking and coping with diseases (and life), specifically Lyme.
Dr. Trunzo earned his undergraduate degree in 1993 from Marywood University in Scranton PA and completed his graduate work in 2000 at Drexel University in Philadelphia, PA. He completed his pre-doctoral internship at the University of Vermont and his post-doctoral fellowship at the Centers for Behavioral & Preventive Medicine at Brown University Medical School in Providence, RI.
He is a Professor of Psychology and Chair of the Department of Applied Psychology at Bryant University. He is also a licensed, practicing clinical psychologist with expertise in the psychological management of chronic medical illnesses such as cancer and Lyme disease, as well as the treatment of mood and anxiety disorders, especially obsessive compulsive disorder.
He serves on several professional committees and belongs to a number of professional organizations. In his spare time, he enjoys being with his family, live music, running, and mountain climbing. This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at https://www.ted.com/tedx
Mental Brakes to Avoid Mental Breaks | Steven Hayes
Mental Brakes to Avoid Mental Breaks | Steven HayesHow can we best deal with difficult or negative thoughts? Dr. Steven Hayes discusses language, cognition, and the science behind putting on the mental brakes.
 Steven C. Hayes is Nevada Foundation Professor at the Department of Psychology at the University of Nevada. An author of 38 books and more than 540 scientific articles, he has shown in his research how language and thought leads to human suffering, and has developed “Acceptance and Commitment Therapy” a powerful therapy method that is useful in a wide variety of areas. His popular book “Get Out of Your Mind and Into Your Life” was featured in Time Magazine among several other major media outlets and for a time was the number one best selling self-help book in the United States. Dr. Hayes has been President of several scientific societies and has received several national awards, such as the Lifetime Achievement Award from the Association for Behavioral and Cognitive Therapy.
Steven C. Hayes is Nevada Foundation Professor at the Department of Psychology at the University of Nevada. An author of 38 books and more than 540 scientific articles, he has shown in his research how language and thought leads to human suffering, and has developed “Acceptance and Commitment Therapy” a powerful therapy method that is useful in a wide variety of areas. His popular book “Get Out of Your Mind and Into Your Life” was featured in Time Magazine among several other major media outlets and for a time was the number one best selling self-help book in the United States. Dr. Hayes has been President of several scientific societies and has received several national awards, such as the Lifetime Achievement Award from the Association for Behavioral and Cognitive Therapy.
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
Psychological flexibility: How love turns pain into purpose | Steven Hayes
Psychological flexibility: How love turns pain into purpose | Steven HayesWhat can we do to prosper when facing pain and suffering in our lives? More than a thousand studies suggest that a major part of the answer is learning psychological flexibility. Steven C. Hayes is one of the researchers who first identified that process and put it into action in the form of a popular acceptance and mindfulness method called Acceptance and Commitment Therapy. In this emotional talk, Hayes distills the essence of psychological flexibility down into a few easy to understand sentences. He takes viewers through a harrowing journey into his own panic disorder, to the very moment in his life when he made this life changing choice: I will not run from me. Hayes shows how making that choice allows us to connect with our own deep sense of meaning and purpose, arguing that taking a loving stance to your own pain allows you to bring love and contribution into the world.
Steven C. Hayes is Nevada Foundation Professor at the Department of Psychology at the University of Nevada. An author of 38 books and more than 540 scientific articles, he has shown in his research how language and thought leads to human suffering, and has developed “Acceptance and Commitment Therapy” a powerful therapy method that is useful in a wide variety of areas. His popular book “Get Out of Your Mind and Into Your Life” was featured in Time Magazine among several other major media outlets and for a time was the number one best selling self-help book in the United States. Dr. Hayes has been President of several scientific societies and has received several national awards, such as the Lifetime Achievement Award from the Association for Behavioral and Cognitive Therapy.
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
The Power of Small | Aisling Leonard-Curtin
The Power of Small | Aisling Leonard-Curtin Aisling Leonard-Curtin, M.Sc., C.Psychol., Ps.S.I., is a chartered counselling psychologist who lives with her wife Trish in Dublin. She is co-director of Act Now Purposeful Living, has a private practice, and deliver acceptance/mindfulness workshops. She has over a decades experience in a wide range of settings including adult psychiatry, psycho-oncology, educational, health and community. Aisling’s hobbies include writing fiction, performing improve comedy and hanging out with her pets. Aisling Leonard-Curtin, M.Sc., C.Psychol., Ps.S.I., is a chartered counselling psychologist who lives with her wife Trish in Dublin. She is co-director of Act Now Purposeful Living, has a private practice, and deliver acceptance/mindfulness workshops. She has over a decades experience in a wide range of settings including adult psychiatry, psycho-oncology, educational, health and community. Aisling’s hobbies include writing fiction, performing improve comedy and hanging out with her pets. This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at https://www.ted.com/tedx
Aisling Leonard-Curtin, M.Sc., C.Psychol., Ps.S.I., is a chartered counselling psychologist who lives with her wife Trish in Dublin. She is co-director of Act Now Purposeful Living, has a private practice, and deliver acceptance/mindfulness workshops. She has over a decades experience in a wide range of settings including adult psychiatry, psycho-oncology, educational, health and community. Aisling’s hobbies include writing fiction, performing improve comedy and hanging out with her pets. Aisling Leonard-Curtin, M.Sc., C.Psychol., Ps.S.I., is a chartered counselling psychologist who lives with her wife Trish in Dublin. She is co-director of Act Now Purposeful Living, has a private practice, and deliver acceptance/mindfulness workshops. She has over a decades experience in a wide range of settings including adult psychiatry, psycho-oncology, educational, health and community. Aisling’s hobbies include writing fiction, performing improve comedy and hanging out with her pets. This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at https://www.ted.com/tedx
The gift and power of emotional courage | Susan David
The gift and power of emotional courage | Susan DavidPsychologist Susan David shares how the way we deal with our emotions shapes everything that matters: our actions, careers, relationships, health and happiness. In this deeply moving, humorous and potentially life-changing talk, she challenges a culture that prizes positivity over emotional truth and discusses the powerful strategies of emotional agility. A talk to share.
 Susan David, Ph.D. is one of the world’s leading management thinkers and an award winning Harvard Medical School psychologist. Her new #1 Wall Street Journal bestselling book, Emotional Agility based on the concept Harvard Business Review heralded as a Management Idea of the Year and winner of the Thinkers50 Breakthrough Idea Award, describes the psychological skills critical to thriving in times of complexity and change. She is a frequent contributor to the Harvard Business Review, New York Times, Washington Post, Wall Street Journal, and guest on national radio and television. Named on the Thinkers50 global list of the top management thinkers, Susan is a sought-after keynote speaker and consultant, with clients that include the World Economic Forum, EY, United Nations, Google, Microsoft, NASDAQ, and many other national and multinational organizations. Her focus is on defining and executing effective strategy, especially in the areas of engagement, high-performance leadership, and culture change. Susan is the CEO of Evidence Based Psychology, on the faculty at Harvard Medical School, a Cofounder of the Institute of Coaching (a Harvard Medical School/McLean affiliate), and on the Scientific Advisory Boards of Thrive Global and Virgin Pulse. Susan is also core faculty of the global Homeward Bound, an all-women leadership program that culminates in an expedition to Antarctica and aims at increasing the influence and impact of women in the sciences.
Susan David, Ph.D. is one of the world’s leading management thinkers and an award winning Harvard Medical School psychologist. Her new #1 Wall Street Journal bestselling book, Emotional Agility based on the concept Harvard Business Review heralded as a Management Idea of the Year and winner of the Thinkers50 Breakthrough Idea Award, describes the psychological skills critical to thriving in times of complexity and change. She is a frequent contributor to the Harvard Business Review, New York Times, Washington Post, Wall Street Journal, and guest on national radio and television. Named on the Thinkers50 global list of the top management thinkers, Susan is a sought-after keynote speaker and consultant, with clients that include the World Economic Forum, EY, United Nations, Google, Microsoft, NASDAQ, and many other national and multinational organizations. Her focus is on defining and executing effective strategy, especially in the areas of engagement, high-performance leadership, and culture change. Susan is the CEO of Evidence Based Psychology, on the faculty at Harvard Medical School, a Cofounder of the Institute of Coaching (a Harvard Medical School/McLean affiliate), and on the Scientific Advisory Boards of Thrive Global and Virgin Pulse. Susan is also core faculty of the global Homeward Bound, an all-women leadership program that culminates in an expedition to Antarctica and aims at increasing the influence and impact of women in the sciences.
The secret to self control | Jonathan Bricker
The secret to self control | Jonathan BrickerJonathan Bricker's work has uncovered a scientifically sound approach to behavior change that is twice as effective as most currently practiced methods. His new methods are driving new norms and new apps for how people quit smoking and decrease obesity, saving many people from an early death.
 Jonathan Bricker is an internationally recognized scientific leader in a bold approach called acceptance and commitment therapy. A Stanford researcher called his use of the approach “a breakthrough in behavioral research [that] has major public health implications for the major causes of preventable death.” Bricker and his team, having received $10 million in total federal research grants to study this topic, are rigorously testing this intervention on multiple platforms, including smartphone apps, websites, and telephone coaching. His SmartQuit app for quitting smoking was recently launched and is now in distribution worldwide.
Jonathan Bricker is an internationally recognized scientific leader in a bold approach called acceptance and commitment therapy. A Stanford researcher called his use of the approach “a breakthrough in behavioral research [that] has major public health implications for the major causes of preventable death.” Bricker and his team, having received $10 million in total federal research grants to study this topic, are rigorously testing this intervention on multiple platforms, including smartphone apps, websites, and telephone coaching. His SmartQuit app for quitting smoking was recently launched and is now in distribution worldwide.
This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at http://ted.com/tedx
Why It's Hard Being Human | John Forsyth
Why It's Hard Being Human | John ForsythJohn devoted most of his adult life to writing, speaking, teaching, doing research, and training mental health professionals and the public in the use of Acceptance and Commitment Therapy (ACT) and practices that cultivate mindfulness, loving kindness, and self-compassion. He is also a Professor of Psychology and Director the Anxiety Disorders Research Program at the University at Albany, SUNY in Upstate New York. This is a job that he absolutely love. But he also wear many other hats. He’s a licensed clinical psychologist in New York, with expertise in the use and application of Acceptance and Commitment Therapy (ACT) for several forms of psychological and emotional suffering. He is also an active researcher, teacher, and consultant and serve as a senior editor of the ACT book series with New Harbinger Publications. His talk is a narration of why it is hard to be human in today's advanced world. John devoted most of his adult life to writing, speaking, teaching, doing research, and training mental health professionals and the public in the use of Acceptance and Commitment Therapy (ACT) and practices that cultivate mindfulness, loving kindness, and self-compassion. He has been at this for over 20 years, and have seen the enormous impact that ACT can have in the lives of many, including my life too.
He is a Professor of Psychology and Director the Anxiety Disorders Research Program at the University at Albany, SUNY in Upstate New York. This is a job that he absolutely love. But he also wear many other hats. He’s a licensed clinical psychologist in New York, with expertise in the use and application of Acceptance and Commitment Therapy (ACT) for several forms of psychological and emotional suffering. He is also an active researcher, teacher, and consultant and serve as a senior editor of the ACT book series with New Harbinger Publications. This talk was given at a TEDx event using the TED conference format but independently organized by a local community. Learn more at https://www.ted.com/tedx
Η αξία της ζωής | Maria Karekla
Η αξία της ζωής | Maria Karekla
Η Δρ. Μαρία Καρεκλά είναι κάτοχος διδακτορικού στην Κλινική Ψυχολογία, με ειδικότητα στις Αγχώδεις Διαταραχές και στην Ψυχολογία της Υγείας. Είναι Επίκουρη Καθηγήτρια στο Τμήμα Ψυχολογίας του Πανεπιστημίου Κύπρου και υπεύθυνη του εργαστηρίου ACThealthy: Εργαστήρι Κλινικής Ψυχολογίας και Συμπεριφορικής Ιατρικής, καθώς συντονίζει την επιτροπή του διδακτορικού προγράμματος στην κλινική ψυχολογία. Επίσης προεδρεύει της Επιτροπής Βιοηθικής Κύπρου για βιοϊατρικές μελέτες και είναι μέλος του Συμβουλίου Εγγραφής Ψυχολόγων.
Ανάμεσα στις ερευνητικές της δραστηριότητες συμπεριλαμβάνονται έργα στο θέμα της θαλασσαιμίας, του διαβήτη, των διατροφικών διαταραχών, του άσθματος, του καπνίσματος και των χρόνιων πόνων. Οι έρευνες της έχουν λάβει επιχορήγηση από Εθνικούς, Ευρωπαϊκούς και άλλους φορείς και έχουν βραβευτεί από οργανισμούς όπως η Ευρωπαϊκή επιτροπή και το Pompidou group, το Association for the Advancement of Behavior Therapy και το Society of Behavioral Medicine. Έχει στο βιογραφικό της πέραν των 50 δημοσιεύσεων σε επιστημονικά περιοδικά. Επίσης εκπροσωπεί το Πανεπιστήμιο Κύπρου και την Κύπρο σε διάφορες επιτροπές που άπτονται του επαγγέλματος της.
 Dr. Maria Karekla holds a doctorate degree in Clinical Psychology from the University at Albany, SUNY with a specialisation in Anxiety Disorders and Health Psychology. Currently holds the position of Assistant Professor for Clinical Psychology at the University of Cyprus and she is responsible for the ACTHealthy lab: Laboratory of Clinical Psychology and Behavioral Medicine, while she is a key member in the development of the doctoral level clinical psychology program. She actively and systematically participates in psychological research projects that have received awards by (among others) the European council and Pompidou’s group, and the Association for the Advancement of Behavior Therapy. Her research focuses on areas of health promotion and the investigation of individual difference factors (especially experiential avoidance) as they relate to the development and maintenance of various forms of psychopathology (especially anxiety disorders and health related problems). She is a member of the clinical psychology and school psychology program development committees at the University of Cyprus. Maria is currently a member of the European Awarding Committee for the specialization of psychotherapy of EFPA and has served as a liaison of the Cyprus Psychologists Association to numerous subcommittees and task forces of EFPA. A number of her research projects have received local, EU and other funding. Dr. Karekla’s “ACTHealthy: Anxiety disorders and Health Psychology” research laboratory has cooperated with other institutions, business and bodies both in Cyprus and abroad on numerous project.
Dr. Maria Karekla holds a doctorate degree in Clinical Psychology from the University at Albany, SUNY with a specialisation in Anxiety Disorders and Health Psychology. Currently holds the position of Assistant Professor for Clinical Psychology at the University of Cyprus and she is responsible for the ACTHealthy lab: Laboratory of Clinical Psychology and Behavioral Medicine, while she is a key member in the development of the doctoral level clinical psychology program. She actively and systematically participates in psychological research projects that have received awards by (among others) the European council and Pompidou’s group, and the Association for the Advancement of Behavior Therapy. Her research focuses on areas of health promotion and the investigation of individual difference factors (especially experiential avoidance) as they relate to the development and maintenance of various forms of psychopathology (especially anxiety disorders and health related problems). She is a member of the clinical psychology and school psychology program development committees at the University of Cyprus. Maria is currently a member of the European Awarding Committee for the specialization of psychotherapy of EFPA and has served as a liaison of the Cyprus Psychologists Association to numerous subcommittees and task forces of EFPA. A number of her research projects have received local, EU and other funding. Dr. Karekla’s “ACTHealthy: Anxiety disorders and Health Psychology” research laboratory has cooperated with other institutions, business and bodies both in Cyprus and abroad on numerous project.
More CBS TEDxTalks
More CBS TEDxTalksFree ACT Articles, Podcasts, and Interviews
Free ACT Articles, Podcasts, and InterviewsThere are several articles that have appeared in magazines and popular news outlets, as well as interviews with ACT experts on the radio, the internet, and podcasts. Click on the following links to peruse these articles: ACT in Popular Media and also Podcasts.
ACT in Popular Media
ACT in Popular MediaThe links below are to articles that have appeared in popular media outlets, interviews with ACT therapists in online or radio sources, and other links of interest to you.
ACBS Members: Please note that this section of the site is intended for members of the public. Therefore, whenever possible, please copy the text of an article or interview onto the site and/or post links to the original media source directly (e.g., hyperlinks) when you add to this section.
Podcasts
PodcastsACBS Podcasts
- 15 in 15 - the ACBS World Conference 15 Podcast (2017)
- ACT in Context: The Acceptance and Commitment Therapy Podcast (2011)
ACBS Chapter and SIG Podcasts
- PodACT (Brazil Chapter)
- Colombia Contextual: Un Podcast de ACBS Colombia Chapter (2021)
- Podcast: Voices & Values - DEI SIG (2017)
Other Podcasts
ANZ Chapter President, Julian McNally, Radio Interview Feb 2024
ANZ Chapter President, Julian McNally, Radio Interview Feb 2024In this interview conducted by ABC Radio Newcastle at the beginning of the ANZ ACBS Chapter Conference, Julian explains for the general public the difference between CBS and other approaches to psychology, how values provide a context for behavior change, examples of defusion and the impossibility of changing thoughts, and outlines the close links in the ACBS community between practitioners and researchers.
This clip is an excerpt of the whole interview (6'20''). To hear the whole interview, click here: http://gofile.me/2o6SF/n0hrRIfqn
To join or learn more about ANZ Chapter of ACBS, go here: anzacbs.com.
The Times of India - Therapy for the desi mind (2022)
The Times of India - Therapy for the desi mind (2022)Therapy for the desi mind
Acceptance and commitment therapy teaches people to acknowledge their negative feelings instead of trying to resist or wrestle with them
By Saranya Chakrapani / TNN / May 22, 2022
“I began taking a deep dive into Indian spiritual texts like the Upanishads and Buddhist philosophies and found a whole lot of metaphors that could be used to convey the idea of self-empowerment through the ACT modality to someone struggling with anxiety or depression,” says Dr Balaji.
Washington Post: "A meaningful life is possible amid suffering, some therapists say" (2022)
Washington Post: "A meaningful life is possible amid suffering, some therapists say" (2022)A meaningful life is possible amid suffering, some therapists say
Acceptance and commitment therapy teaches people to acknowledge their negative feelings instead of trying to resist or wrestle with them
By Katherine Kam February 19, 2022
Emily Sandoz, a psychologist in Louisiana, has witnessed clients’ grueling struggles during the pandemic. Many said they felt trapped and deprived of their usual ways of coping. Others began therapy for the first time after the pause in their busy lives forced some existential questions: “Do any of these things that I used to put all this energy into even matter? Does my job even matter? Do my relationships matter?”
Then, she said, her clients felt guilty.
“I know that this has been stressful for everyone, but . . .”
“I just feel like I should be able to handle this.”
“I know what I need to do, but I’m just not doing it.”
It’s natural to feel distress during such a harrowing time, Sandoz tells them, but even in the midst of inevitable pain and hardship, people can still live meaningful lives aligned with their highest values.
Sandoz provides a form of behavioral therapy called acceptance and commitment therapy, or ACT. Psychologists consider it a third-wave therapy after traditional behavior therapy and cognitive behavioral therapy. Infused with mindfulness concepts, ACT acknowledges that suffering is part of the human condition and guides people in becoming “psychologically flexible” to navigate life’s ups and downs and keep moving forward.
Wall Street Journal: "How to Deal With Stress in Your Life: Embrace It" (2021)
Wall Street Journal: "How to Deal With Stress in Your Life: Embrace It" (2021)How to Deal With Stress in Your Life: Embrace It
By Elizabeth Bernstein August 28, 2021
When frustration, anxiety and fear start to cloud the mind, psychologists recommend an approach called acceptance that helps people deal clearheadedly with tough situations.
Read the article at https://www.wsj.com/articles/how-to-deal-with-stress-in-your-life-embrace-it-11630152000
BBC: "Fibromyalgia and Pain" (2021)
BBC: "Fibromyalgia and Pain" (2021)Fibromyalgia and pain: 'How cooking gave me my family back'
By Bryony Hopkins April 6, 2021
Ian spent years "existing" until the NHS referred him to the pain management programme at the Bath Centre for Pain Services. The programme focuses on a psychological model called acceptance and commitment therapy, which looks at finding ways to move forward with things that can't be shifted. Read more about Ian's story at https://www.bbc.com/news/disability-56536589
Wall Street Journal "How to Live With the Pain of Loss, Without Going Numb" (2018)
Wall Street Journal "How to Live With the Pain of Loss, Without Going Numb" (2018)How to Live With the Pain of Loss, Without Going Numb
People often try to deny their feelings, but that doesn’t work. Here are some healthier techniques.
August 20, 2018 Interview with Steven C. Hayes
https://www.wsj.com/articles/how-to-live-with-the-pain-of-loss-without-going-numb-1534772199
ACT in Popular Media Archives (2001 - 2017)
ACT in Popular Media Archives (2001 - 2017) CommunityLauren Porosoff Articles - Using ACT and RFT in the Classroom (2017)
Lauren Porosoff Articles - Using ACT and RFT in the Classroom (2017)Solution Tree - flexible context sensitivity and functional coherence (2018)
Brian Goff talks ACT - 101.9 FM, Portland (2016)
Brian Goff talks ACT - 101.9 FM, Portland (2016)Hear radio host Sheila Hamilton interview Evergreen Clinical’s Brian Goff about ACT on KINK’s Speaking Freely (101.9 FM Portland, OR).
The Self-Acceptance Project (2013)
The Self-Acceptance Project (2013)In this free online video event series, Tami Simon speaks with several contemporary luminaries in the fields of spirituality, psychology, and creativity. Together they explore the questions around self-acceptance—and investigate how we can overcome the difficulties of embracing who we are. Where do our self-critical voices come from? Can we silence them, or is there a better way to deal with them? Can we be motivated to change and excel while still accepting ourselves as we are? Why is it often so much easier to feel compassion and forgiveness towards others than towards ourselves?
Russ Harris Interview (May 2012)
Russ Harris Interview (May 2012)3 day workshop with Russ Harris in Copenhagen: Interview with Russ Harris on the 15th of May 2012
Interview by Maria Krøl and Ole Taggaard Nielsen
I: What was it that brought you to ACT?
R: I thought it was a very realistic look at the human condition. It starts with the premise that life involves lots of pain. No matter how good your life gets there’s going to be plenty of pain that goes with it. I found that to be very realistic. We’re all gonna have lots of painful feelings, we’re all gonna have lots of negative thoughts. So how do we learn to live with that? How can we still live a rich, full and meaningful life, even with the pain? So it was very realistic, and it really resonated with my experience. And I liked that there was a lightness and playfulness about the model; it had a sense of humor. I also love the creativity of it; the way that it frees you up to design your own metaphors and your own interventions. It gave me a lot of freedom as a therapist; there are just so many different ways I can do it. I love that I can be creative and playful. And I love the compassion and the self-compassion that’s built into the model. And I think more than anything, I loved the training: how it was about working with my own issues, and applying the approach to my own stuck-points in life; to help with my own pain and suffering. It just really resonated with me.
I: You mentionend that you used to do traditional CBT. When did you move in the ACT direction?
R: I started working as a GP (family doctor) in 1991 and I became increasingly interested in the psychology of health and wellbeing. And as I started spending more and more of my time looking at the role of stress in the lives of my patients. My consultations would average to 20-30 minutes, which was unusually long for a GP. 5 minutes at the end of the session would be about the medical problem, and 25 minutes would be about what’s happening in your life: the stresses and difficulties. And I started to realize that I was really in the wrong profession.
So I wanted to train in therapy and the first model I trained in was traditional CBT. And I liked it. It’s a very effective model. I think I started formally doing sessions of therapy as opposed to GP counselling, in about 1994. And from that point, until 2003, I mainly did traditional CBT. However, at the same time that I was doing CBT, I kept training in other models, I was always looking for other things because even though CBT had some really good stuff, it didn’t, for example, have much to say about finding meaning and purpose in life. Also, I was very interested in mindfulness. There’s a whole branch of medicine called Psychoneuroimmunology, which is about the connection between the mind and the body, and there was some very interesting research coming out, about the benefits of mindfulness meditation for the immune system. So I was very interested in mindfulness, but it was very hard to get my clients to meditate.
As for traditional CBT, I really liked the behavioral elements: the skills-training, exosure, scheduling, and goal-setting etc, and I also liked the distancing components, where you become more aware of your thinking processes; but I didn’t like the components that were about challenging thoughts, because it didn’t actually work for me. I could challenge my thoughts all day long, but they’d just keep coming back, again and again. And I liked the mindfulness stuff, but I wasn’t overly keen on meditating. And I wanted to explore meaning and purpose with my clients, but I wasn’t quite sure how to do it. So I was trying for many years to bring these elements together: behavioural activation, mindfulness, cognitive distancing, meaning and purpose. I didn’t know anything about ACT, but it’s what I was intuitively trying to do. So when I finally discovered ACT in 2003, it was like ”WOW, this is fantastic!” A friend told me about it, I went to the book store, I looked at the book and it was love at first sight. ”Oh My God, this is fantastic.” I just fell head over heels in love with it. I became obsessed with it, and I instantly moved all my clients from traditional CBT to ACT. It was a bit confusing for them initially. I would say, ”No, no we don’t need to challenge those thoughts anymore”. They would say, ”Really?”
I: What is the goal of ACT, and how is it different from traditional CBT?
R: The aim of ACT is to create a rich, full and meaningful life while accepting the pain that inevitably goes with it. You might get some CBT people to say that’s the aim of CBT too - but words like ”rich, full, meaningful”, well, I didn’t encounter that emphasis in my own CBT training. More technically the aim of ACT is to increase psychological flexibility. And that’s definitely not the aim of CBT. Psychological flexibility is your capacity to be in the present moment, open fully to your experience and act in line with your values: to ”Be present, open up and do what matters”. That’s the outcome we’re looking for.
I: Could you tell me a little bit about the therapeutic stance in ACT?
R: The therapeutic stance is that ”We’re both in the same boat”. There’s no real difference between client and therapist; it’s just who’s sitting in that chair on that day. This metaphor that we like to share on the first session is the ”two mountains metaphor”. I say to clients: you come along to therapy, and it’s easy to get the idea that therapists have their life sorted out, that they don’t have any issues, no major problems. And I don’t want you to leave this room buying into that illusion. I want to shatter that myth right now. What’s it like is, you’re climbing your mountain over there and I am climbing my mountain over here. From where I am on my mountain I can see stuff on your mountain that you can’t see. For example, I might be able to see an alternative pathway that’s easier, or you’re using your pickaxe incorrectly, or there’s an avalanche about to happen. But I’d hate you to think that I’m sitting on the top of my mountain, no problems, no issues, just sitting back and enjoying life. I’m climbing my own mountain, over here. And we’re all climbing our mountain till the day we die. But what we can learn to do here is to climb more effectively, climb more efficiently; learn how to enjoy the climbing. Learn how to take a break and have a good rest and take in the view and appreciate how far we’ve come. That’s what this is about. So it’s a stance of commonality and equality: we’re both in the same boat; we’re dealing with the human condition. It’s not like some people have got a mental illness and some don’t; this is the human condition.
I: What is ”happiness” in ACT?
R: In ACT we stay away from the word ”happiness” because most people think that happiness means ”feeling good”. So in ACT rather than using the term happiness we use the term ”vitality”: a sense of embracing this moment of life, living this moment of life to the fullest. Steve Hayes has a saying: ”There’s as much life in a moment of pain as a moment of joy”. So the question is: ”Can I embrace this moment of life, whether it’s a very painful moment or whether it’s a joyful moment?” I say to clients all the time: ”If you’re going to live a full human life you’re going to feel the full range of human emotions”. So if you pushed me hard to define happiness in terms of the ACT model I would say ”Happiness means living a rich, full and meaningful life in which we feel the full range of human emotions - both the painful ones and the pleasent ones - without a struggle.”
I: How can you as a therapist help a client to identify personal values?
R: Many different ways. You can often identify them by asking questions: What matters to you? What’s important to you? A question I ask every client on the first session is: ”If the work that we do in this room could make a difference in one relationship, which relationship would that be? How would you behave differently in that relationship as a result of the work that we do?” Other useful questions are ”What do you want to stand for in life?”; ”When you look back at your life from your deathbed, what do you want to say that life was about?”; ”If you could be the ’ideal you’, how would you treat your body, how would you treat your children, how would you treat your job, how would you treat the environment, how would you treat your loved ones?”. You can think of vaues as how you would treat your relationship with anyone or anything; what are the qualities that you would bring to it? For many people these questions are useful. However, some people just go blank when you ask them such questions; in which case, we would do experiental exercises, of which there are many. One of the best is Kelly Wilson’s ”sweet spot” exercise, where you ask someone to get in touch with a very rich sweet memory, one of life’s ”sweet spots”. So it could be a memory of a time of love, a time of creativity, a connection with nature, a moment of achievement or pride or having fun, or a simple pleasure. We help them to relive the memory, and then we ask them questions to tease values from it: What does this memory tell you about what matters to you? What qualities were you embodying in the memory? What does this tell you about the way you want to behvae or the things you want to do more of, moving forwards? In this memory what were you ”in relationship with”? Was it a relationship with nature, or with your body, or with a loved one, or with an activity? In that relationship, what personal qualities were you embodying? There are many experiemental exercises, but the sweet spot is a particularly good one.
I: What are your thoughts on medication as a treatment for depression and other psychological problems?
R: The ACT stance on medication is like the ACT stand on everything else. The ACT model rest on the concept of ”workability”: is it working to give you a rich, full and meaningful life. If it is, keep doing it. If it’s not, do something different. This would be the ACT stance for any medication; not just psychiatric medication, but also medication for diabetes or cancer. For example some people with cancer choose not to have chemotherapy. They figure ”The chemotherapy won’t cure me, it will just give me six extra months of life- and the quality of life will be so low, I’d rather not do that.” So the ACT stance on medication is neither for it, nor against it; it’s all about workability. And there are quite a few published ACT studies where clients were on medication as well as doing ACT.
I: Do you have clients that choose to be on medication?
R: Sure, and if they do, I’ll work with them. I ask clients on antidepressants: ”What difference do they make?” The most common answer I’ll get is: ”I felt a bit better initially but now I don’t know if they’re doing anything” or I’ll get: ”I’m not feeling as much pain, but I’m not feeling as much of anything”. Most therapists don’t ask, but if you ask clients on antidepressants if they have sexual problems, about 70% of clients will say ”yes”. The incidence is much higher than the drug companies acknowledge. It’s a big problem. If a client considers the costs of being on medication outweigh the benefits - as many of them do - I will work in conjunction with a psychiatrist to help them get off it. I personally don’t want to play the role of prescribing medication or monitoring medication; I’m not interested in that. Basicly since I started doing therapy, I’ve said, ”I’m here to work with you as a therapist, if you want medication, you go see a gp or a psychiatrist, they can monitor all of that.”
I: You seem to use a lot of your own experiences in your book, in presentations and in therapy; what is the purpose of that?
R: ACT is a model that is in favor of self-disclosure from the therapist. ACT doesn’t insist on self-disclosure, but it’s very much in favor of it. If you read the literature you’ll certainly find studies and papers warning you about the dangers of self-disclosure, but you’ll also find plenty about the enormous therapeutic benefits of self disclosure. ACT is in favor of self-disclosure as long as it is done mindfully and judiciously: to model ACT for the client, or validate their experience, or normalize their experience, or build therapeutic rapport in a useful way.
I: Today when you did tell your own story, I think people got very emotional and touched by it. Are you purposefully aiming to bring up emotionality in the client?
R: What we are aim to do in ACT is to model and instigate and reinforce ACT processes. So I can model the ACT processes, I can instigate them, and if I see them happening in the room, I can reinforce them. One way of modelling them is through self-disclosure. We want to have an intimate therapeutic relationship. Kelly Wilson uses the term ”values and vulnerabilities”. If you know nothing about my values and vulnerabilities, we don’t have an intimate relationship.
Now ACT doesn’t insist on this. You can do ACT and be closed off, without sharing any of your personal thoughts or feelings; but it’s very different when you open up and self-disclose. It helps to break the illusion that the therapist has their life sorted out and doesn’t struggle with this stuff. Many of our clients are fused with the idea that ”everyone else is happy and has a wonderful life except for me”. When the therapist says, ”I get anxious too” or ”My mind is saying that I’m not good enough”, the client goes, ”Oh woww, you too!”
I: What are you occupied with at the moment in ACT concerns?
R: I’m writing four books. I’m writing with Louise McHugh – co-authoring a textbook, trying to make RFT really simple and understandable, and link it to ACT. RFT is the theory of language and cognition that underlies ACT, and many people find it really hard - so we’re trying to make it really simple.
I’m also writing a self-help book with Joe Ciarrochi and Ann Bailey on the use of ACT for weight loss. There are five or six published studies now on ACT with weight loss. That book is called ”The weight escape”, and it should be out in late 2013. I’m nearing completion of an advanced-level textbook called ”Getting Unstuck in ACT” for people who already know the basics of ACT. It’s about the most common ways therapists get stuck, and how to get unstuck again. That should be out in early 2013. And I’m writing a humorous book on mindfulness called ”The Way of The Sloth”. The sloth is an animal in South America. It hangs upside down from the trees with these hugh long claws, and it’s really slow moving. It’s the slowest mammal in the world. In English, the word ”sloth” means ”laziness”. ”Sloth” is one of the ”seven deadly sins” in the bible. Everyone thinks that this animal, the sloth, is really lazy - but what we’re saying in this book is that it’s a master of mindfulness. It doesn’t waste any energy; it’s this mindful creature; the zen master of the forest. So it’s a humorous book, where everyone gathers in the forrest to ask the sloth questions about life, the universe and everything.
I: Do you still have clients?
R: Not many, these days. Just a handful. I’d like to see more but I just don’t have the time; I’m always travelling and teaching.
I: Would you like to tell us a bit about your new book ”The reality slap”? It will published in Danish soon?
R: A ”Reality Slap” is when life just slaps you in the face, knocks you around, turns your world upside down. So ”The Reality Slap” is a book for anyone who goes through a major stressful life event; in particular, it’s about loss and grief. Death of a loved one, bankruptcy, divorce, major illness, a serious accident, a disability: any of these big life events. How do we cope with these events? There are 4 basic principles.
First principle: Hold yourself kindly. This is about self-compassion: Can I be kind to myself? There’s a massive gap here between what I want and what I’ve got; there’s a huge amount of pain showing up: so can I be kind to myself? Many of us don’t know how to do that. We stuff our face with drugs or alcohol or food, or we beat ourselves up, or withdraw from life: this is not really being kind to ourselves. So what are simple ways that I can be kind and caringand supportive to myself, in the midst of my pain?
The second principle, I call ”Dropping an anchor”. All these painful emotions, thoughts, feelings: it’s like an emotional storm. And if I get swept away by the storm, there’s nothing effective I can do. So how do I drop an anchor? Basically, I use mindfulness to ground myself in the present moment, and let those thoughts and feelings flow through me, without carrying me away.
The third principle is ”Take a stand”. What do I want to stand for in the face of this? What do I want to be about in the face of this challenge, in the face of this loss, in the face of this tragedy or crisis? I don’t have to give up on life. I can still stand for something, even if what I’m going through is horrendous. Even if the person I loved most has died, I can still stand for something in the face of that. I can give up on life, or I can stand for something that makes it meaningful. So it’s really about values, and committed action.
The fourth and last principle is ”Find the treasure”. Even in the midst of great pain and suffering, there are things that we can treasure and appreciate. For example, when we’re at the funeral of a loved one, we experience great pain - but in the midst of that pain, people reach out to us with love and kindness and caring; so can we appreciate and treasure those moments?
This principle has to come last, only once the other three are in place. The danger is that many people will try to ”find the treasure” as a first line response. They’ll say things like ”Well, every cloud has a silver lining” or ”What does not kill me makes me stronger”. But if that’s the first thing that you say to someone in great pain, they will experience it as completely invalidating. So ”Find the treasure” comes after everything else. And we’re not trying to pretend that the pain is not there. There is pain here AND there are things here that I can appreciate. But principles one to three have to come first.
Dealing with Fear -- Radio interview with Steven Hayes and phone-in questions (October 2011)
Dealing with Fear -- Radio interview with Steven Hayes and phone-in questions (October 2011)In this episode of the Regina Brett show, ACT psychologist Steven Hayes discusses the psychology of fear, and how ACT can help. He then offers advice to individuals who call in with questions.
Or, if you are logged in, you can download the mp3 file which is attached to this page.
Psychology Today: How Analyzing Your Problems May Be Counterproductive (February, 2010)
Psychology Today: How Analyzing Your Problems May Be Counterproductive (February, 2010)How Analyzing Your Problems May Be Counterproductive
Published on February 13, 2010
By Ray B. Williams
When you're upset or depressed, should you analyze your feelings to figure out what's wrong? Or should you just forget about it and move on? New research and theories suggests if you do want to think about your problems, do so from a detached perspective, rather than reliving the experience.
This answer is related to a psychological paradox: Processing emotions is supposed to help you facilitate coping, but attempts to understand painful feelings often backfire and perpetuate or strengthen negative moods and emotions. The solution seems to be neither denial or distraction, according to research conducted by University of Michigan psychologist Ethan Kross, who says the best way to move forward emotionally is to examine one's feelings from a distance or detached perspective.
Kross, along with University of California colleague Ozelm Ayduk, conducted a series of studies that provide the first experimental evidence of the benefits of taking a detached perspective on your problems. Kross says, "reviewing our mistakes over and over, re-experiencing the same negative emotions we felt the first time, tends to keep us stuck in negativity." Their study, published in the July, 2008 issue of Personality and Social Psychology, described how they randomly assigned 141 participants to groups that required them to focus (or not to focus) on their feelings using different strategies in a guided imagery exercise that led them to recall an experience that made them feel overwhelmed by sadness or depression. In the immersed-analysis condition, participants were told to go back to the time and place of the experience and relive it as if it were happening to them over again, and try to understand the emotions they felt, along with the underlying causes. In the detached-analysis condition, the subjects were told to go back the time and place of the experience, take a few steps back and move away from the experience, and watch it unfold as though it was happening to them from a distance, and try to understand what they felt and the reasons for the feelings-- what lessons are to be learned.
The results of the experiment? Immediately after the exercise the distanced-analysis approach subjects reported lower levels of anxiety, depression and sadness compared to those subjects who used the immersed-analysis strategy. One week later the participants were questioned. Those that had used the distanced-analysis strategy continued to show lower levels of depression, anxiety and sadness. In a related study, Ayduk and Kross showed that participants who adopted a self-distanced perspective while thinking about their problems related to anger, showed reductions in blood pressure.
Kross' and Ayduk's research supports the work done by psychotherapist Dr. Steven Hayes. Traditional cognitive psychotherapy may not be the best intervention according to Dr. Steven Hayes, a renowned psychotherapist, and author of Getting Out of Your Mind and Into Your Life. Hayes has been setting the world of psychotherapy on its ear by advocating a totally different approach.
Hayes and researchers Marsha Linehan and Robert Kohlenberg at the University of Washington, and Zindel Segal at the University of Toronto, what we could call "Third Wave Psychologists" are focusing less on how to manipulate the content of our thoughts (a focus on cognitive psychotherapy) and more on how to change their context--to modify the way we see thoughts and feelings so they can't control our behavior. Whereas cognitive therapists speak of "cognitive errors" and "distorted interpretation," Hayes and his colleagues encourage mindfulness, the meditation-inspired practice of observing thoughts without getting entangled by them--imagine the thoughts being a leaf or canoe floating down the stream.
These Third Wave Psychologists would argue that trying to correct negative thoughts can paradoxically actually intensify them. As NLP trained coaches would say, telling someone to "not think about a blue tree," actually focuses their mind on a blue tree. The Third Wave Psychologists methodology is called ACT (Acceptance and Commitment Therapy), which says that we should acknowledge that negative thoughts recur throughout our life and instead of challenging or fighting with them, we should concentrate on identifying and committing to our values in life. Hayes would argue that once we are willing to feel our negative emotions, we'll find it easier to commit ourselves to what we want in life.
This approach may come as a surprise to many, because the traditional cognitive model permeates our culture and the media as reflected in the Dr. Phil show. The essence of the conflict between traditional cognitive psychologists and psychotherapists is to engage in a process of analyzing your way out your problems, or the Third Wave approach which says, accept that you have negative beliefs, thinking and problems and focus on what you want. Third Wave psychologists acknowledge that we have pain, but rather than trying to push it away, they say trying to push it away or deny it just gives it more energy and strength.
Third Wave Psychologists focus on acceptance and commitment comes with a variety of strategies to help people including such things as writing your epitaph (what's going to be your legacy), clarifying your values and committing your behavior to them.
It's interesting that that The Third Wave Psychologists approach comes along at a time when more and more people are looking for answer outside of the traditional medical model (which psychiatry and traditional psychotherapy represent). Just look at a 2002 study in Prevention and Treatment, which found that 80% people tested who took the six most popular antidepressants of the 1990's got the same results when they took a sugar pill placebo.
The Third Wave Psychologists approaches are very consistent with much of the training and approach that many life coaches receive, inclusive of Neuro-Linguistic Programming (NLP), and many spiritual approaches to behavioral changes reflected in ancient Buddhist teachings and the more modern version exemplified by Eckhart Tolle (The Power of Now and A New Earth). The focus of those approaches reinforces the concepts of acceptance of negative emotions and thoughts, and rather than giving them energy and fighting with them, focus on mindfulness, and a commitment to an alignment of values and behavior.
What's fascinating is how brain science and psychological research is supporting ancient spiritual practices. Perhaps now the East and the West, science and spirituality, are coming together.
-----------------------------------------------------------------------
Blogs: Wired for Success
How to fulfill your potential
Ray Williams is Co-Founder of Success IQ University and President of Ray Williams Associates, Inc., providing leadership development, personal growth, and executive coaching services.
accessed from psychologytoday.com
Russ Harris Interviewed on RadioNZ (2010)
Russ Harris Interviewed on RadioNZ (2010) Jen PlumbBigThink.com Interview with Steve Hayes (2009)
BigThink.com Interview with Steve Hayes (2009)Topics discussed in the interview:
- What Keeps Steven Hayes Up at Night?
- The Tolerating Cure
- How to Deal With a Panic Attack
- Happiness Is an Empty Promise
- The Catch-All Nature of Acceptance and Commitment Therapy
- Finding a Career by Way of a Panic Attack
Full Interview Transcript:
Question: What led you to explore this field of psychology?
Steven Hayes: Well, I'm in psychology probably the way a lot of people get into psychology: you're interested in why there's so much pain and suffering around you. And I certainly saw that at home, just growing up, and decided early on that it was a place to put my science interests and also just my humanitarian interests, and you could put those two together in one field. After I was a psychologist I developed a panic disorder, and that changed a lot of -- what kind of work I do, because I was trained as a behavior therapist and as a cognitive behavior therapist. And when I applied the methods that I would apply with others when they had panic disorder, it didn't really fully hit what I thought was needed for me.
And I turned back towards several things that were sort of in my experience from more eastern traditions, human potential traditions, and then tried to marry that up -- I'm a child of the '60s and grew up in California, so was exposed to the kind of garden variety eastern thinking that most folks in my generation were exposed to, and I actually found more in mindfulness and acceptance methods that were directly of benefit to me than in the traditions I was nominally part of.
So that really changed my thinking, and it caused me to set out on about a 30-year journey as to how dig down to the essence of what's inside some of our deepest clinical traditions, but also our spiritual and religious traditions, particularly these eastern traditions. But not just that; all of the mystical wings of the major spiritual and religious traditions have methods that are designed to change how you interact with your logical, analytical, linear thinking. And I didn't want to leave that just intact; I didn't want to simply be a meditation teacher or something. I wanted to understand it, and we spend a lot of time kind of pulling at its joints and trying to understand why these things might be helpful to people, I think particularly helpful to people in the modern world who are exposed through the media and the kind of chattering world that we've created to a lot of horror, a lot of pain, a lot of judgment, a lot of words, and need to find a place to go that is more peaceful and more empowering, being able to lives their lives in an intimate, committed, effective way. So that's kind of how I came there, or I ended up where I ended up.
Question: What is ACT and how does it differ from traditional forms of cognitive therapy?
Steven Hayes: Sure. Well, the empirical clinical traditions, especially in the cognitive behavioral tradition, early on they were trying to apply behavioral principles mostly developed with animal models directly to people. And there's a lot of benefit that happened there; it's still relevant today. You can do a lot of good things for people who suffer with anxiety, depression and so on using those methods. I'm old enough to have seen all three of these steps, and somewhere in the late '70s and mid-'80s people realized that you had to have a better way of dealing with cognition, and they couldn't find it in the animal models. So they went to more commonsense clinical models where they would sort of divide thinking styles up into rational and irrational processes, making cognitive errors and so forth. And they thought if we could just get people to think more rationally and focus on the evidence and take some of those over-expansive thoughts that are creating difficulty for them and change them, then they'd do better. And some of it was -- the techniques were helpful, but the theory didn't work very well.
Increasingly over time we learned that the components that theory tells you to put in and the processes that should change didn't really explain the outcomes and add to the outcomes. And it had this potential for a downside: people can get even more self-focused, even more caught up in their own thinking. And we're part of a newer sort of third generation of tradition that is using acceptance and mindfulness practices and values, commitment, behavior change practices and marrying them up. So the difference between traditional CBT and the acceptance and commitment therapy, or ACT -- but not just ACT; also mindfulness-based cognitive therapy, dialectical behavior therapy, a number of the other more kind of modern acceptance and mindfulness approaches -- instead of teaching people to detect, to challenge, to dispute and change their thinking, we teach people to notice what they're thinking and to notice what they're feeling, what their body is doing, learn from it, but then focus also on their values and getting their feet moving towards the kinds of lives that they want to produce to have a life worth living.
And it turns out that that's, we think, a quicker and more direct way, a more certain way, to moving ahead in your life than first trying to get the cognitive ecology inside this skull of ours all lined up with an ability to detect our logical errors and correct them and so forth. Meanwhile, the clock is ticking. There's relationships to have, children to be raised, work to be done, contributions to be made, and you're waiting to get the world within all lined up. We think it's more effective to find a way to back up from that a little bit; notice it, see what's there, learn from it, and move ahead directly towards the kind of lives that you want to produce. And it turns out those processes are not just in therapy, but in this office, in your home, in the schools and organizations. And so the ACT work has very quickly expanded out from psychotherapy into behavioral medicine, and from that even into organizational work and now into prevention work and into communities and schools. So it's kind of exciting to see psychology touching people where they are, in the streets, in a way that is empowering and sort of simplifies what it is that people need to learn to be more effective and happy, successful, vital in their lives.
Question: How can a therapist help someone realize their values?
Steven Hayes: You know, a couple of things: if someone watching this were to focus on what pains them the most, and then would take the time to look inside -- what do I care about such that that's particularly painful? -- they're probably going to find a significant area that they value. I'll give an example: most people are hurt deeply by betrayals in relationships. And what your mind tells you to do is, don't be so vulnerable; don’t be so silly; don't open yourself up; don't be so trusting; you can be betrayed. In fact, the reason why you hurt so much is that you want relationships that are loving, committed, intimate; you want trust. And what your mind's telling you to do in a way is, don't care about that so much so that you won't be hurt so much. It might be better to really get up against and sort of contact that caring, and maybe take a more loving stance even with your own pain, and keep your feet moving towards what you really want, because the cost in terms of intimacy and connection and caring that comes when you try not to be vulnerable, when you're constantly looking out for betrayals of trust, is too great. It makes it very hard to have relationships of the kind that you really want. So there's an example. One, look where the pain is. Flip it over; you'll find that's where the values are.
Another one is just to think of the times that you've felt most with yourself, most connected, most vital, most energized, most flowing, natural. And if you take some of these specific memories and you walk inside them, you're going to find that there's things in there that you care about. There's things in there that, when it's really working well, are kind of a lighthouse, like a beacon in the distance, that you can move towards. You never fully reach these things. I mean, I'll give you an example. There are times when you felt especially important to another person, or cared about or loved or accepted. Well, loving relationships aren't something you can have like a precious little jewel you put in a box and then put on your shelf. It's something you walk towards. And there's always difficulties; there's always pain in relationships. But you can keep walking towards that beacon in the distance. That process, that journey, is called life. And if you're moving towards the things that you value, life is more vital, flowing; it's more empowering. And so that's another way: go inside the sweetness of life, catch the places where you genuinely were moved by or connected with life, and you'll find in there kind of a light that can direct you when the cacophony gets very noisy and you get confused and lost, that can direct you towards what you care about.
Question: How does the role of an ACT therapist differ from the role of traditional psychologists?
Steven Hayes: It might be a little bit, because this psychology is a psychology of the normal. A lot of the psychologies that are out there are built on the psychology of the abnormal. We have all these syndromal boxes that we can put people in and so forth. The actual evidence on syndromes is not very good. I mean, there's no specific biological marker, for example, for any of the things that you see talked about in the media. Even things like schizophrenia -- there's no specific and sensitive biological markers for these things. So yeah, there may be some abnormal processes involved in some of them, but vastly more of human suffering comes from normal processes that run away from us. Like normal processes of problem-solving work great on the world without; when it's applied within, you too easily get into a mode of mind where you can start living when the problem of your history is solved.
But your history's not going to go away; it isn't the same thing as dirt on the floor or paint peeling off the walls; it's not going to be solved in that way. It's more like learning how to carry it, to contact it, to see it. Because it's based on the psychology of the normal, the therapist is part of that too. And so when the therapist gets in there and is working on acceptance and mindfulness and values, they too are working with those very same processes. And so it requires a therapist not to be a master at it -- you don't even have to be good at it -- but just to see the value of it and to be willing to look at their own difficult emotions and thoughts and find a way to carry them gently in the service of the clients that they're serving.
So for example, if a therapist is feeling insecure in therapy, a lot of therapists will try to sort of push that aside to try to do the therapy. Instead, we would ask people to get with that feeling of insecurity, because after all, the client is being asked to do the same thing. So it tends to be relatively intense, interactive, horizontal. It's not one up; the therapist is in the same soup. And it has a kind of a quality of two human beings in the same situation, really, working through these psychological processes. And yeah, I'm working for you; you hired me; I'm working for you as a therapist. But I'm not up here and you're down there. And what you're struggling with, at other times and with other areas I'm struggling with.
Question: Why can ACT treat everything from schizophrenia to prejudice?
Steven Hayes: Well, and even more than that. I mean, I've mentioned even in this office the same processes are there. We've done research showing that ACT and the processes that underlie it can help things like can secretaries learn new software? Can therapists learn new methods? What about stigma and prejudice between people? So it isn't just in the psychotherapy areas. And why that would be, as an empirical fact there's a pretty enormous breadth to these methods. And why that would be -- because everywhere that a human mind goes, these processes of avoiding the world within in order to try to regulate your behavior, or becoming entangled in your thoughts interfering with your ability to take advantage of what's around you, or losing contact with your values for fear that you'll know more about the places where you hurt -- those kinds of processes are just normal psychological processes that are built into language and cognition itself. They're built into problem-solving. And so if you take the mode of mind that works great in 95 percent of your life and apply it within, it then implodes. It starts creating barriers, and that's true at work, it's true in organizations, it's true in our culture, true in our politics. And yeah, it's true in our consulting rooms.
So we're going -- the reason why it spreads out -- we have pretty good evidence for this; I know it sounds a little grandiose -- but the mental cognitive processes that we're targeting are ones that narrow human beings' repertoire and make it harder for them to learn to be more flexible, to take advantage of the opportunities in front of them. And we think that's something we can have something to say about, something to help with in all of these different areas, maybe even in areas like child development or organizations and schools, or maybe even things like prevention or how peoples interact with each other, one to the other. So we've taken the work, for example, into things like prejudice and stigma, because in the modern world, if we can't solve that we have planes flying into buildings. And then we have planes flying over countries. The amount of hate and objectification and dehumanization that's on the planet isn't something we can tolerate any more in a world that's coming of suitcase bombs and the ability to amplify that hate out into harm towards each other. So it applies broadly because anywhere that a human mind goes these processes go.
Question: What is happiness?
Steven Hayes: You know, there's many different definitions of it. I think one dangerous definition of it is to think of happiness as kind of a warm, joyful, **** feeling in your heart that you have to pursue and grab and hold onto for fear that it'll go away. I mean, it's fun when you have those feelings, but we know, and the evidence shows, them more intent you are on having those feelings and chasing those feelings, that's a butterfly that flies away the more you chase it. A better way to think about happiness that actually is something that I think you can reach towards is, it's living in accord with your values and in a way that is more open and accepting of your history as it echoes into the present, that's more self-affirming, self-validating and values-based. The Greeks had a word for it; they called it eudaimonia, and it's not a bad definition. And I think that definition of happiness is something that will empower human lives.
The definition that we have that gets very hedonistic and emotion-oriented -- the problem is that there's too many quick and dirty ways to chase that in ways that end up being unhelpful to people. If you avoid the feelings of betrayal and the sense of insecurity that comes in relationships that aren't working by running into detuned relationships, by sexuality that isn't connected to intimacy, et cetera. Yeah, you might feel good, but it doesn't live well. If you just have another martini or even more severe forms of substance use, yeah, it might feel good, but it doesn't live well. And if you escape into kind of a materialism -- the right car, the right woman, the right house, the right trip, the right place, the right job, the right praise -- you know, these things -- all of the folks who are wise in our culture, over the history of our culture, have written about the dangers of trying to define a meaningful life that way. But commercial culture and our media is constantly encouraging us to think that if we feel good we live well. And then we're only too happy, thank you very much, to sell you goods and services from the dancing oivoids and the pill you can take, or the trips or the cars or the clothes or the women that you can get with -- whatever that is that will give you the quick route to that.
And it's an empty promise. I think young people know it's empty, but they're not quite sure what to do. And I kind of look at what's on the T-shirts and I see another solution, which also worries me. I see "Just do it." "No fear." -- this kind of suppressive response to the treacle that the culture tries to define for us as a meaningful life also blows up on you. "No fear" is not something that you should put on your shirt. How about "I can hold my fear and still connect with you"? Put that on your shirt. "It’s okay to be me, with all of my history." Put that on your shirt. So there's a middle path. There was a guy who sat under a tree a long time ago who is important to a pretty big chunk of the human population that called it The Middle Path. There is a middle path between indulgence and suppression, but the culture has overwhelmed that in the cacophony that has been created in the modern world and the commercial encouragement of avoidance and indulgence on the one hand, or suppression and "just do it," treating yourself as an object on the other. We've got to find a way that's more compassionate, softer, that allows us to move forward towards the kind of lives that we really want to live.
Question: Are Americans striving too much for happiness?
Steven Hayes: I think the commercial culture, and also science and technology after all, which gives us greater ease but also makes it harder for us to sit with the small amounts of distress that come just by living itself, is probably -- the combination of the commercial culture and the media culture and the science and technology has probably made it more difficult in American culture. But I think it's built into language and cognition. It was only given some counterweights -- the major institutions that are there are our spiritual and religious traditions, which emerged very early on, at the point at which human language grew and written language created kind of the problem that we can have now with language kind of running away from us. And those traditions have weakened too in our culture, and they've changed. So we probably do -- it isn't that we're chasing happiness; I think we have the wrong model of happiness. I mean, defined as eudaimonia, defined as a values-based life of integrity and fidelity to yourself and what you most deeply want to stand for, that definition of happiness -- man, that's the kind of life I want to live and I think that will support people and sustain people.
But this cheap-thrill version, this sort of ease definition, the feel-good definition of happiness is an empty promise. And the culture in the West I think has done a particularly bad job of indulgence in that vision of what happiness is and encouraging people to chase it. And I think we can see in the growing amount of problems that we have in the developed world that it's an empty promise. And I'll give you an example, not from the U.S., but in Scandinavia probably the most worker-supportive part of the planet, they have the highest rate of chronic pain and the greatest rate of worker-related disability. So right inside this idea that any kind of pain and difficulty is so much unwelcome that if you say that you're in pain, we're going to come in guns a-blazing and even pay you full salary to quit work because you're burned out, or to -- inside that what you're going to create is gigantic amounts of chronic pain syndrome. Scandinavians spend 15 percent of their gross national product on disability. Fifty percent of the public health nurses are on disability. I mean, and that's where we're headed in the U.S. too, because unless we get wiser as to how to carry the difficulties of life in a way that's self-compassionate and empowering, we can create this kind of world in which we'd rather sort of plug into the matrix with whatever pills or escapist tendencies we can think of instead of walking through a process of living that's going to include loss. It's going to include limitations on function. It's going to include some significant difficulties. We need to learn and teach our children how to do that. And the West is just doing a terrible job of that right now.
Question: Do you believe in medicating depression and other forms of mental illness?
Steven Hayes: Medication -- I want good science, and big pharma is only too happy to give us bad science, because the way the FDA is set up and what the requirements are -- I mean, these are geek topics, and the normal person wouldn't really know how to evaluate it. But you only require a certain number of randomized trials. You don't have to have the proper control groups. You can have the blind be penetrated; people can know that they're on the medication, which we know there's a big placebo effect inside medications. So the science is often inadequate. The best science that's out there, then I want to -- then that's fine; let's go there. And there's decent science.
Let's take something like antidepressant medications. There's decent science saying it has an effect, but it's shockingly small after you control for penetration of the blind, people knowing that they're getting the active pills versus sugar pills, if you use an active control. It's probably only a few points. Like in depression, on the 56-point scale, the estimate is it probably accounts for about two points difference. But it's a multi, multibillion-dollar industry. And by the way, has huge side effects. And some of these medications, 40 percent of the people taking them have significant sexual side effects, for example. And that's just one. The level -- a single antidepressant medication can be worth a billion dollars to a company.
So I want good science, and I want it to be realistically marketed. I wouldn't like -- I think all these commercials that we have -- only two countries on the planet that allow pharmaceutical companies to market directly to people, New Zealand and the United States -- it's a bad idea, in my opinion. I think it ought to be better regulated. And when it's presented to people, it ought to be presented in a way that's realistic. For example, often people will prescribe these medications, and we'll say, you have a brain disease; you'll have to be on these medications permanently. It's because you have a brain disease. Well, brain disease -- there would be a specific biological marker for the so-called disease. There is no biological marker for depression. It's not true that we know that it's a brain disease. Is the brain involved in depression? Yes, the brain is involved with what you and I are doing right now. If neither one of us had a brain, we wouldn't be having a conversation. But that doesn't mean it's a brain disease.
And so the prescribers very often overstate, oversell, and the detail people are only too happy to tell them to do that. This idea that there's something wrong with your brain, and because of that you're permanently -- by the way, almost never are these medications evaluated with what will happen if you're on them for three, four, five, 10, 15 years. Sometimes some of the side effects that come up come up only later, and sometimes they're very severe, even irreversible side effects. So I would like it to be more like yes, these medications might be helpful to a degree, but what they do in areas like depression or antipsychotics is, they give you a little more distance between the things that cause you to get entangled with thoughts and feelings. And so they might be of some help, open up a little window. Now can we go in there and learn some of these methods directly to do that?
For example, antidepressant medications, you still have some depressive thoughts. Antipsychotic medications, you still have some psychotic symptoms for the vast majority of the people taking them. But it gives them a little separation, and it doesn't control his behavior as much when you have a sad feeling, difficult thought, an odd perceptual experience. We can teach people those exact skills in therapy, and so evidence is pretty good if you use it as just a window to get in there and teach these skills, you get longer-term benefits and without the side effects. So don't be sold just because a commercial interest wants to sell you things. The government ought to help out, because the average citizen can't go out and be doing reviews of the scientific literature. And focus on the processes that have low side effects and good long-term outcomes. Right now you're going to find those in the psychosocial area, in the therapy area, in the empirically supported treatments such as ACT or cognitive behavior therapy, behavior therapy. And go there first rather than going to the pill bottle as if it's going to be the end of your journey, that it's going to solve the problem. Very often it's only going to help, and even only to a minor degree, and more is going to be needed.
Question: What’s your advice to someone dealing with a panic attack?
Steven Hayes: Well, the advice I'd give if you were my patient would be a little different because we'd have a little more time. But if I can distill it down to the essence of what we do in a course of therapy, the person with panic -- I can say this from the inside out since you're looking at a panic-disordered person in recovery -- has adopted a posture with regard to the world within in which their own anxiety is their enemy. And they think that if they can just get the anxiety to go down, go away, not occur as much or not occur with such intensity, or at least not occur here, or there, in that situation, that then things would be better. In fact, all of that is not the solution to the problem; it is the problem. Holding anxiety as your own enemy, and that it has to go down, diminish it, go away and not happen here is a kind of self-invalidating, interiorly focused process that would get you even more entangled with these processes. Instead, what we're going to need to learn to do is to allow your history to bring into the present thoughts and feelings and memories, and to sort of hold them mindfully and self-compassionately, and then focus on what you do and bring them along for that journey.
So -- feelings are only your history being occasioned by the present moment. If that's your enemy, then your history is your enemy. If sensations are your enemy, your body is your enemy. And if memory is your enemy, you'd better have a way of controlling your mind in such a way that you never are reminded of things that are painful from the past. Well, there is no such thing like that that's healthy. And most of the things that people do that are called psychopathology are the unhealthy things people do when they try to accomplish that agenda. If you avoid people, avoid having your buttons pushed, avoid going to places that might occasion anxiety; if you're hammering down drugs and alcohol; these are all methods of trying to mount that unhealthy agenda.
So I would say, could we instead take this anxiety to be something that may be of importance, may even be meaningful? And it says something about your history, and could we learn to sort of hold it in a way that's more compassionate, to sort of bring the frightened part of you close and treat it with some dignity, and keep focused -- instead of making that go away -- focused instead on what kind of life you want to live connected to what kind of meaning and purpose. That's going to be a quicker, more self-compassionate and more certain journey forward than this kind of "out with the anxiety, in with the relaxation," "out with the self-doubt, in with the confidence" kind of -- "let's just snap out of it" kind of harsh and non-compassionate place that we stand with ourselves inside things like panic disorder.
Question: Why don’t some psychologists believe in the effectiveness of ACT?
Steven Hayes: It's an argument about theory and processes, but the processes, and the ones we've been talking about, inform what we think of ourselves and what we should encourage in our children and what we should try to put into the culture. And I think really we've been through a time when we thought we could think our way out of this, and kind of think clearly and that would solve the problem, and detect logical errors and that would solve the problem. We thought of suffering as a problem of sort of dysfunctional cognitions. I think we're coming into a time instead where it has to do with how you stand in relationship to your own world within and in relationship to those around you in the world without. And I believe these are the things that we need to put into our schools, education, into our psychotherapy and into our culture more, finding a way to not be so harsh and judgmental, so objectifying and dehumanizing, constantly focused within and trying to get these difficult thoughts and feelings to go away; or focused without and objectifying and dehumanizing others. So the core of the controversy is, is it more powerful to take an acceptance and mindfulness-based approach compared to a cognitive and emotional change approach when we're dealing with these problems? I think the evidence is more in our favor, especially the process evidence.
And I think if you look at where the culture is going, there's a reason why Eckhart Tolle is on Oprah. There's a reason why The Purpose-Driven Life is a best seller, quite apart from appealing to evangelicals and the Christianity that's in it. It's also -- there's a yearning for meaning, for values and for mindfulness and acceptance, because we've created a modern world where our children are exposed to 10, 20, 30 times the number of words that our great-grandfathers were exposed to. And we're exposed in a single day or two to more horror on our Internet Web pages than our great-grandfathers were exposed to in decades of living. And we have not created modern minds for that modern world. Science and technology has just dumped it on us. And I think people yearn for it. I think you see it in what's popular. And why are people wanting to learn about meditation, and why are they going on mindfulness retreats? And why are they talking about a purpose-driven life? It's because they know more is needed in the modern world.
And that's the core of the controversy. I think it's pretty clear in how things are moving in empirically supported treatments that we're going to be speaking to the culture in a different voice. It's not going to be the loosey-goosey voice of the '60s, but it's going to have some echoes of some of the deeper clinical and spiritual and religious traditions that had wisdom in it. If we're not going to get there through religious means and things of that kind, which greatly has weakened in the West, we're going to have to find a way to put it in the culture in a different way, because we need something right now other than yet another cable shoutcast or yet another Internet Web page showing us the cellulite on the actress's rear end. I mean, the amount of sort of judgment and harshness that's in our culture -- we need something that's prophylactic for that, and I think that's what's inside these new methods.
Question: What keeps you up at night?
Steven Hayes: What keeps me up at night in a positive way is the possibility that we might contribute to the development of human culture in a way that, years from now, people who will never know our names may be able to live more empowered lives. And if you ask like what is the name of your great-great-great-grandfather, you probably don't even know if you get three or four greats out. So it's not that we're immortal; we're going to die very, very soon. It's not that what we produce is going to live on; it will not. But the changes that we can make in the culture can be there for people that we will never meet, that will never know us, and that's what keeps me up at night. It's what excites me about science, that we can learn ways of being with each other. And the behavioral sciences have not been enough of a part of cultural development. The physical sciences have; the behavioral sciences have not. And I would like to see if we can bring some things into human culture that would humanize and soften and empower people.
What keeps me up at night in a negative way is, if we don’t solve these problems of the human heart and of the human head, of human psychology, there is no technological solution so great that it can prevent the world that is coming, and a world of suitcase bombs or of the ability to pollute the planet in a way that it cannot recover, of global warming and the rest. We've created through science and technology a different world that has frightening sides to it, and psychology and behavioral science has to be part of this, because if you take something like the so-called war on terrorism, if we go out another 20 years and it isn't just planes into buildings, but it's a suitcase bomb in the middle of New York, there's not enough soldiers and there's not enough bullets to kill enough people to make us safe. I think we're going to have to find a way to humanize the culture itself.
And it isn't just them; it's us. When we fly planes over countries, dropping bombs on the evil ones, I think we're doing something very similar to what's being done when the infidels are getting their comeuppance with planes going into buildings. So it's gotten to the point where if we are not healthy psychologically as a human society, we will not have a planet to live on. And that's what keeps me up at night, when I see so little focus on the behavioral side of these problems, and the idea that just politics, or just physical science, is going to solve this. Or just the military; it's not true. We have to solve this, and we've got to solve it in our own heads and in our own hearts, one at a time. And I think psychotherapy actually tells us a little bit about what we might need to do to soften the culture and make it more possible for us to live together as human beings on this planet.
Time Magazine: Self-Help Through Negative Thinking (2009)
Time Magazine: Self-Help Through Negative Thinking (2009)Cloud, J. (July 2009). Yes, I suck: Self-help through negative thinking. Time Magazine. Time, Inc.: New York, NY.
In the past 50 years, people with mental problems have spent untold millions of hours in therapists' offices, and millions more reading self-help books, trying to turn negative thoughts like "I never do anything right" into positive ones like "I can succeed." For many people — including well-educated, highly trained therapists, for whom "cognitive restructuring" is a central goal — the very definition of psychotherapy is the process of changing self-defeating attitudes into constructive ones.
But was Norman Vincent Peale right? Is there power in positive thinking? A study just published in the journal Psychological Science says trying to get people to think more positively can actually have the opposite effect: it can simply highlight how unhappy they are.
The study's authors, Joanne Wood and John Lee of the University of Waterloo and Elaine Perunovic of the University of New Brunswick, begin with a common-sense proposition: when people hear something they don't believe, they are not only often skeptical but adhere even more strongly to their original position. A great deal of psychological research has shown this, but you need look no further than any late-night bar debate you've had with friends: when someone asserts that Sarah Palin is brilliant, or that the Yankees are the best team in baseball, or that Michael Jackson was not a freak, others not only argue the opposing position, but do so with more conviction than they actually hold. We are an argumentative species.
And so we constantly argue with ourselves. Many of us are reluctant to revise our self-judgment, especially for the better. In 1994, the Journal of Personality and Social Psychology published a paper. showing that when people get feedback that they believe is overly positive, they actually feel worse, not better. If you try to tell your dim friend that he has the potential of an Einstein, he won't think he's any smarter; he will probably just disbelieve your contradictory theory, hew more closely to his own self-assessment and, in the end, feel even dumber. In one fascinating 1990s experiment demonstrating this effect — called cognitive dissonance in official terms — a team including psychologist Joel Cooper of Princeton asked participants to write hard-hearted essays opposing funding for the disabled. When these participants were later told they were compassionate, they felt even worse about what they had written.
For the new paper, Wood, Lee and Perunovic measured 68 students on their self-esteem. The students were then asked to write down their thoughts and feelings for four minutes. Every 15 seconds during those four minutes, one randomly assigned group of the students heard a bell. When they heard it, they were supposed to tell themselves, "I am a lovable person."
Those with low self-esteem — precisely the kind of people who do not respond well to positive feedback but tend to read self-help books or attend therapy sessions encouraging positive thinking — didn't feel better after those 16 bursts of self-affirmation. In fact, their self-evaluations and moods were significantly more negative than those of the people not asked to remind themselves of their lovability.
This effect can also occur when experiments are more open-ended. The authors cite a 1991 study in which participants were asked to recall either six or 12 examples of instances when they behaved assertively. "Paradoxically," the authors write, "those in the 12-example condition rated themselves as less assertive than did those in the six-example condition. Participants apparently inferred from their difficulty retrieving 12 examples that they must not be very assertive after all."
Wood, Lee and Perunovic conclude that unfavorable thoughts about ourselves intrude very easily, especially among those of us with low self-esteem — so easily and so persistently that even when a positive alternative is presented, it just underlines how awful we believe we are.
The paper provides support for newer forms of psychotherapy that urge people to accept their negative thoughts and feelings rather than try to reject and fight them. In the fighting, we not only often fail but can also make things worse. Mindfulness and meditation techniques, in contrast, can teach people to put their shortcomings into a larger, more realistic perspective. Call it the power of negative thinking.
---------
View this original article online here.
Also click our link to access the 2006 Time article by John Cloud referenced in the above article.
ACBS Professional/Student Members: Once you are logged in, you can view the original Woods, et al (2009) article here.
ACT Articles in Veja Magazine in Portugese (2006)
ACT Articles in Veja Magazine in Portugese (2006) Steven HayesAn Overview of ACT; Psychotherapy Australia Magazine (2006)
An Overview of ACT; Psychotherapy Australia Magazine (2006)Embracing Your Demons: an Overview of Acceptance and Commitment Therapy By Russ Harris
This a simplified overview of ACT, written deliberately in a non-technical manner, so that therapists and counsellors of all backgrounds can appreciate it.
Martha Beck's story in O Magazine (2006)
Martha Beck's story in O Magazine (2006)This is Martha Beck's column in "O":
MELANIE'S LIFE WAS SHRINKING LIKE A CHEAP BLOUSE in an overheated dryer. At 30 she'd developed a fear of flying that ended her dream of world travel. Within a year, her phobia had grown to include—or rather, exclude— driving. After the World Trade Center attacks, Melanie became terrified to enter the downtown area of any city. She quit her job as an office manager (the potential for mail-based terrorism was too big) and called me hoping I could help her devise a way of earning money from home.
"Everybody tells me my fears aren't realistic," she said. "But I think I'm the most realistic person I know. It's a dangerous world— I just want to be safe."
There was only one thing for which Melanie would leave her apartment. Once a month, she walked to a rundown neighborhood to meet her drug dealer, who sold her Xanax and OxyContin of questionable purity. I insisted that Melanie see a psychiatrist before I'd work with her, and the worried shrink called me before the impression of Melanie's posterior had faded from his visitor chair. "She's taking enough medication to kill a moose," he told me. "If she slipped in the shower and knocked herself out, withdrawal could kill her before she regained consciousness."
Ironic, n'est-ce pas? Safety-obsessed Melanie was positively devil-may-care when it came to better living through chemistry. This made no sense to me—until I realized that Melanie's objective wasn't really to avoid danger but to prevent the feeling of fear.
Melanie was using a strategy psychologist Steven Hayes, PhD, calls experiential avoidance, dodging external experiences in an effort to ward off distressing emotions. It wasn't working. It never does. In fact, to keep her tactics from destroying her, she would have to learn the antidote for experiential avoidance—and so must the rest of us, if we want our lives to grow larger and more interesting, rather than smaller and more disappointing.
Why Experiential Avoidance Seems Like a Good Idea
Most of us do this kind of emotional side step, at least occasionally. Maybe, like Melanie, you feel skittish on airplanes, so you take the train instead. In the realm of physical objects, dodging situations associated with pain is a wonderfully effective strategy; it keeps us from pawing hot stovetops, swallowing tacks, and so on. Shouldn't the same logic apply to psychological suffering? According to Hayes, it doesn't. Experiential avoidance usually increases the hurt it is meant to eliminate.
Consider Melanie, who, quite understandably, wanted to steer clear of the awful sensation of being afraid. Every time she withdrew from a scary activity, she got a short-term hit of relief. But the calm didn't last. Soon fear would invade the place to which Melanie had retreated—for example, she felt much better driving than flying for a little while, but it wasn't long before she was as petrified in cars as airplanes. Drugs calmed her at first, but soon she became terrified of losing her supply. By the time we met, her determination to bypass anything scary had trapped her in a life completely shaped by fear.
The reason this happens, according to Hayes and other devotees of relational frame theory, is that Melanie's brain works through forming connections and associations. So does yours. Your verbal mind is one big connection generator. Try this: Pick two unrelated objects that happen to be near you. Next answer this question: How are they alike? For instance, if the objects are a book and a shoe, you might say they're alike because they both helpedyou get a job (by being educated and dressing well). Ta-da! Your book, your shoe, and your job are linked by a new neural con¬nection in your brain. Now you're more likely to think of all these things when you think of any given one.
This means that every time you avoid an event or activity because it's painful, you automatically connect the discomfort with whatever you do instead. Suppose I'm having a terrible hair day, and to not feel that shame, I cancel a meeting with a client. Just thinking about that client brings on a pang of shame. If I watch a movie to distract myself, I may be hit with an unpleasant twinge just hearing the name of that movie. This happens with every form of psychological suffering we try to outrun. Your true love dumps you, and to stave off grief, you avoid everything you once shared —your favorite song, the beach, mocha lattes. Now you're bereft not only of your ex but also of music, seascapes, and a fabulous beverage. Your losses are greater, as is your grief. So you go on a hike to cheer yourself up, and what do you think as you gaze at the lovely scenery? Well, duh. You wish your ex were seeing it with you, and you're sadder than ever. When we run from our feelings, they follow us. Everywhere.
The Willingness Factor
In Hayes's book Get Out of Tour Mind & into Your Life, he suggests that we picture our minds as electronic gadgets with dials, like old-fashioned radios. One dial is labeled Emotional Suffering (Hayes actually calls it Discomfort). Naturally, we do everything we can to turn that dial to zero. Some people do this all their lives, without ever noticing that it never works. The hard truth is that we have no ultimate control over our own heartaches.
There's another dial on the unit, but it doesn't look very enticing. This one Hayes calls Willingness, though I think of it as Willingness to Suffer. It's safe to assume that we start life with that dial set at zero, and we rarely see any reason to change it. Increasing our availability to pain, we think, is just a recipe for anguish souffle. Well, yes...except life, as Melanie so astutely commented, is dangerous. It'll upset you every few minutes or so, sometimes mildly, sometimes apocalyptically. Since desperately twisting down the Emotional Suffering dial only makes things worse, Hayes suggests that we try something radical: Leave that dial alone—abandon all attempts to skirt unpleasant emotions—and focus completely on turning up our Willingness to Suffer.
What this means, in real-world terms, is that we stop avoiding experiences because we're afraid of the unpleasant feelings that might come with them. We don't seek suffering or take pride in it; we just stop letting it dictate any of our choices. People who've been through hell are often forced to learn this, which is why activist, cancer patient, and poet Audre Lorde wrote, "When I dare to be powerful—to use my strength in the service of my vision, then it becomes less and less important whether I am afraid."
Once we're willing to confront our emotional suffering, we begin making choices based on attraction instead of aversion, love instead of fear. Where we used to think about what was "safe," we now become interested in doing what seems right or fun or meaningful or ripe with possibilities. Ask yourself this: What would I do if I stopped trying to avoid emotional pain? Think of at least three answers (though 30 would be great and 300 even better). Write them here:
1.
2.
3.
Stick with this exercise until you get a glimmer of what life without avoidance would be like. To paraphrase Dr. Seuss, Oh, the places you'd go! Oh, the people you'd meet, the food you'd eat, the jokes you'd tell, the clothes you'd wear, the changes you'd spark in the world!
One thing none of us will ever be able to calculate is how much we've lost by not having these experiences—something Hayes calls the pain of absence. Being unwilling to suffer robs us of incalculable joy—and the awful punch line is that we still get all the anguish we tried to escape (and then some).
The Consequences of Willingness
What happens when we're willing to feel bad is that, sure enough, we often feel bad—but without the stress of futile avoidance. Emotional discomfort, when accepted, rises, crests, and falls in a series of waves. Each wave washes parts of us away and deposits treasures we never imagined. Out goes naivete, in comes wisdom; out goes anger, in comes discernment; out goes despair, in comes kindness. No one would call it easy, but the rhythm of emotional pain that we learn to tolerate is natural, constructive, and expansive. It's different from unwilling suffering the way the sting of disinfectant is different from the sting of decay; the pain leaves you healthier than it found you.
It took Melanie a huge leap of faith to accept this. She finally decided to turn up her Willingness to Suffer dial, simply because her Emotional Suffering levels were manifestly out of her control. She started by joining a yoga class, though the thought of it scared her witless. She found that her anxiety spiked, fluctuated, and gradually declined. Over the ensuing months, she entered therapy, traded her street-drug habit for prescribed medication, and found a new job. Melanie's worry isn't completely gone; it probably never will be. But that doesn't matter much. She is willing to accept discomfort in the pur¬suit of happiness, and that means she'll never be a slave to fear again.
To the extent that we reject anything we love solely because of what we fear, we're all like Melanie. Find a place in your life where you're practicing experientialavoidance, an absence where you wish there were something wonderful. Then commit to the process of getting it, including any inherent anxiety or sadness. Get on an airplane not because you're convinced it won't crash, but because meeting your baby niece is worth a few hours of terror. Sit on the beach with your mocha latte, humming the song you shared with your ex, and let grief wash through you until your memories are more sweet than bitter. Pursue your dreams not because you're immune to heartbreak but because your real life, your whole life, is worth getting your heart broken a few thousand times.
When fear makes your choices for you, no security measures on earth will keep the things you dread from finding you. But if you can avoid avoidance — if you can choose to embrace experiences out of passion, enthusiasm, and a readiness to feel whatever arises—then nothing, nothing in all this dangerous world, can keep you from being safe.
-------
Martha Beck is the author of Leaving the Saints and The Joy Diet (both Crown).
New Harbinger's interview with Steve Hayes (2006)
New Harbinger's interview with Steve Hayes (2006)Interview with Steven Hayes on Get Out of Your Mind and Into Your Life
New Harbinger Publications: In Get Out of Your Mind and Into Your Life, you contradict some of the most central tenets of psychology. You say for example that, “accepting your pain is a step toward ridding yourself of your suffering,” and “we assume that...suffering is normal and it’s the unusual person who learns how to create peace of mind.” How did you come to adopt ideas that are so contrary to earlier models of psychological thought?
Steven C. Hayes: Actually the idea that human suffering is pervasive is hardly new. Most of our spiritual and religious traditions begin there, for example. And our scientifically based therapy traditions inadvertently do too, though they don’t seem to realize it. Every professional writing a grant or pitching the need for a new treatment program begins with a section documenting how pervasive a given problem is in the community. And you see that work being written up in the popular media all the time with stories about the unbelievably large numbers of people who have, say, been abused, or have an addiction problem, or struggle with relationships, or have a mental disorder, or who are just stressed at work.
To see the truth of the claim I make in this new book, all you have to do is stop and say, “Hey, wait a minute. What if we added up all of these problems? How many people would fail to be in one ‘abnormal’ grouping or another?” When you craft the question properly the answer hits you in the face: it’s pain and struggle that is normal, not happiness. Most people I know have the personal information needed to reach the same conclusion. Just ask yourself this: How many people do you know really well who don’t struggle at times—or even often—in their lives?
There is almost this conspiracy of silence. Because we’re told that happiness is normal we tend to keep silent about our struggles—it means we’re abnormal. But because most people have the same secret, we walk around feeling isolated and alone. That doesn’t mean you can’t be happy. You can. But you have to learn how to avoid the traps our minds lay for us. The reason why suffering is so pervasive is because we’re so bad at doing anything about it.
The natural, rational thing to do when we face a problem is to figure out how to get rid of it and then actually get rid of it. In the external world, our ability to do just that is what allowed us to take over this planet. But that only works in the world outside of our skin. We don’t at first realize that and so we deal with our own psychological struggles by trying to get rid of our painful feelings, difficult memories, or worrisome thoughts—as if then we’ll be happy. But it doesn’t work.
Modern science is fairly clear that this is one of the surest ways to prevent happiness from ever arriving. Said another way, suffering is so pervasive because our attempts to solve it actually make it persist. We are caught in a trap of our own making. As for how I got there, my position came from three sources. The traditional model didn’t work for me; it didn’t work for my patients; and as I began to research it, I figured out why that was. And our research showed that doing some very counterintuitive things instead did work.
NHP: Can you give us a layperson’s primer on acceptance and commitment therapy (ACT)?
SCH: ACT is based on the idea that psychological suffering is usually caused by running away from difficult private experiences, by becoming entangled in your own thoughts, and as a result of all of that failing to get your feet moving in accord with your chosen core values. ACT is based on a new and extensive basic research program on language and cognition, relational frame theory (RFT), which explains why pain occurs so readily in people and is so hard to solve. Fortunately it also suggests new, powerful alternatives such as acceptance, mindfulness, values, and committed action.
ACT—and this new book—helps people acquire these new skills. They can be learned fairly quickly, and they seem to apply to an amazingly wide range of human difficulties. We teach clients how to back up from thoughts and the world structured by thought and instead to focus on the process of thinking itself: how to feel feelings as feelings, fully and without needless defense, even when we don’t like them; how to show up in the present moment as a conscious human being; and how to begin to act in accord with chosen values. In short, we teach people how to be more flexible in moving toward what they really want and less automatic, programmed, and self-defeating. Get Out of Your Mind and Into Your Life explains how to do just that.
NHP: You claim these ideas apply to almost every psychological problem people face. Can you talk about some of the problems ACT can be applied to?
SCH: Research is showing that ACT methods are beneficial for a broad range of clients. There is almost nothing you can mention that doesn’t have at least some supportive data on the role of acceptance, mindfulness, and values, or negative data on the impact of avoiding your own experiences and failing to act in accord with your values in that same area. ACT teaches people fairly quickly how to alter their relationship to difficult private experiences and how to get behavior change going NOW, rather than waiting to have difficult emotions or thoughts go away before acting.
This empowering message has been shown to help clients cope with a wide variety of clinical problems, including depression, anxiety, stress, burnout, substance abuse, prejudice, smoking, adjusting to chronic disease, and even psychotic symptoms. In the area of anxiety and panic, avoiding your own negative private experiences is one of the strongest predictors of bad outcomes.
Conversely, we now know from research with a variety of anxiety disorders that when you let go of the struggle with anxiety, you’re on the road to a healthier life. This doesn’t necessarily mean that anxiety will go away—it means that its role in your life will diminish, sometimes quickly. If you think about it, you can see why. Suppose I could tell if you were the tiniest bit anxious. You could not fool me. And suppose I then held a gun to your head and said, “Relax completely or I’ll shoot.”
Almost no one would pass such a test. Yet that is the exact situation a panic disordered person has put himself or herself in. Instead of being shot, what is threatened is loss of self-esteem or loss of the view that a good life is possible, but that is pretty much the same thing—and the outcomes are equally predictable. We have several studies now showing that ACT can be helpful with anxiety problems.
Depression is sometimes spoken of as a feeling, but it’s more than that. It’s also an agenda: the agenda of not feeling bad. When you are depressed you are less able or willing to feel, and because of that you are less able or willing to act. Here is one way to put it: depression is what you feel when you are not willing to feel something else. ACT undermines that whole game, and instead focuses on what it is that you really, really want in life, while feeling and thinking whatever you feel and think. It turns out that these feelings won’t be just depression, but perhaps anger, fear, sadness, or loss, among others. If depression has to first go away before a person can move forward, you have an unsolvable problem. But when we learn how to just notice our depressive thoughts, and feel our feelings as feelings, deliberately and fully—it turns out that we can begin to live again, right now, even with depressed feelings or depressogenic thoughts.
And when we do that, we start to move. We’re able to contribute to others. To make a difference. That breaks the back of depression. There are three small controlled studies on ACT and depression, and it makes a big difference. This work is still young, but so far it appears that ACT may actually be more effective than the best current psychological treatment for depression. We will know when bigger studies are done. In science that is the key: replication by others.
Chronic pain leads people to spend their lives trying to find a way to get rid of it, but research shows that this approach to pain makes it more central, more dominant, and more disruptive to people’s lives. Meanwhile there is even a bigger tragedy happening than the pain itself—a life is being lost. It turns out that ACT can greatly improve functioning by helping the chronic pain patient focus on his or her own chosen values and, while being aware of the pain when it’s present, begin to live again.
ACT helps the person with chronic pain step back from the chatter that says he or she can’t live until pain goes away, and without arguing back, simply begin to move forward. I personally don’t have chronic pain. But I do have tinnitus—my ears are screaming 24/7. And do you know what the literature says? Any attempt to cope with it is harmful. What you need to do is to let go of it and focus on living. I now sometimes go an entire day without noticing tinnitus even once—but every time I check, wow! Is it noisy! Chronic pain is like that.
We need to learn to live with it. We are not talking about living with it like putting up with it or tolerating it. We are talking about LIVING with it. It appears that ACT can make a difference in chronic pain quickly. In one study with people just starting to become chronic pain patients, four hours of ACT reduced sick- leave due to pain almost to zero levels; in another with patients who have been in pain for over a decade, three weeks of ACT improved their functioning 20 to 40 percent, depending on the area. So we know we can make a difference with chronic pain.
Most addiction seems to be in large part driven by avoidance and cognitive entanglement. When you use, you are trying to feel only good. Drugs are sometimes called a fix. Fixing means repairing what is broken but it also means to hold something in place. Drug and alcohol abusers are trying to hold “feeling good” in place by chemical means. When you abandon that attempt you will sometimes feel good and sometimes feel bad. If you can do that and focus instead on changing your behaviors, you have a way forward.
We now have controlled ACT studies with several kinds of substance abuse including marijuana and heroin, and they show good effects. ACT has an agenda sort of like that serenity prayer from AA: accept what you can’t change, change what you can. In the prayer, clients ask for the wisdom to know the difference—ACT theory specifies that difference. It’s good to change your behavior; it’s harmful to try to change the automatic results of your history. There are now three randomized trials on ACT for smoking and so far it beats the patch, Zyban, and traditional cognitive behavior therapy.
We also know this: Urges to smoke don’t predict whether or not you can quit. Most people are surprised by that, because urges seem important. But what is missing is the context in which these urges occur. What predicts quitting or not quitting is how much you first have to not feel urges before you can stop. Said another way, the task in smoking cessation is to learn to let the urges and emotions and thoughts just wash over you, while doing nothing at all about them other then noticing them as they are … and to do all of that while not reaching for that cigarette. You do that and you are on the way to quitting smoking for good.
ACT is used in several trauma centers nationwide such as the National Center for PTSD in Palo Alto, CA, or the trauma and substance abuse program at the Baltimore, MA, VA hospital. Entire units are organized around ACT. So the providers in this area see value in what we are doing. Both the basic studies on the psychological process that underlies trauma and early treatment studies show the same thing: it’s not pain that predicts trauma. It’s the unwillingness to feel pain that predicts trauma.
This is an important insight for us all in the modern era because the media has made it possible for all of us to be exposed regularly to horror. We see the bombings in Iraq. We all saw those dots that were not dots coming out of the top floors of skyscrapers on 9/11. World wide we are exposed to amazing levels of painful events every day if we just turn on our televisions. 9/11 is just the clearest example. Now, a few years later, we are learning who was traumatized by those events. It was not those most horrified. It was those most unwilling to feel horrified. And no wonder. If you are unwilling to feel what you already did in fact feel, where do you go? How can you run fast enough? Here is the formula: Pain + unwillingness to feel pain = trauma. The implication of this equation is not mere exposure. We know that poorly timed exposure sometimes actually makes folks worse.
What ACT does is give people the skills they need to willingly carry the pain they have and integrate it into a valued life. You need to learn how to back up from your thoughts and see them as they are; to show up in the moment; to commit to your values. That, plus exposure, will move you ahead.
This is a relatively new area for us but there are now already four studies on compulsions or related phenomena such as skin picking, and ACT appears to be working quite well on these so far. Suppose you have the thought, like Howard Hughes in The Aviator, “aphids are dirty and flowers with these bugs will contaminate you.” That weird thought will produce very unpleasant feelings. So the obsessive person undoes the feeling by throwing out the flowers, by washing his hands, or by other rituals. It produces relief, but it also just feeds the compulsion beast, and it comes back bigger than ever.
ACT cuts that vicious cycle. If you have the thought “aphids are dirty and flowers will contaminate you,” you don’t need to argue with it or make it go away. You need to defuse from that thought. Notice it come and go. Watch it like you’d watch a leaf float by. Do nothing about it, except to think it as a thought. And accept the feelings it produces. Feel them the way you would reach out and feel fabric. And then get back to valued living. You do that and you’ve broken the back of an obsessive cycle. It’s amazing to me that we give people so little help in rising to the psychological challenges of chronic disease.
Take diabetes. Every time a diabetic tests for blood glucose, the implications of this chronic disease become present: it’s a disease that can blind you, lead to loss of limbs, or even kill you. That is a psychologically hard thing to do. And the numbers that come back as you test your blood glucose can be very upsetting—they can be high even when you think they should be low. And each high number once again reminds you that you have a disease that can blind you, lead to loss of limbs, or even kill you.
My wife and I just walked through her gestational diabetes, and it was a roller coaster. We both came away amazed at how hard it was and what a burden people who will deal with this their whole lives must be carrying. We have shown in our lab that just three hours of ACT can double the number of diabetics who are in control of their blood glucose three months later. If that continues, we would reduce loss of limb or blindness by more than half—for only a tiny three-hour intervention.
People are so hungry for help, and the “feel goodism” of the culture just is no help at all. If you can help patients learn to carry their fears, watch their scary thoughts, and focus on valued actions, you are giving them the tools they need to manage their illness. It’s not just a problem of information; it’s a problem of psychological flexibility.
The epilepsy data are even more dramatic. In one recent study a nine-hour ACT program plus medication reduced seizures by over 90 percent at a one-year follow up compared to medication alone. Ninety percent! It seems that the combination of acceptance, mindfulness, and values stopped the self-amplifying loop that kept the stress up, quality of life down, and seizures continuing unabated.
The larger message here is that you have to teach people how to step up to the psychological challenge of physical disease. But you don’t do that by helping people win a war with their insides—you do it my helping them step out of that war and focus of what concrete actions they need to take to live the kind of life that want to live.
ACT is showing good results with stress. Stress is not just the negative results of anxiety or worry—it’s also the effect of control being applied where it doesn’t belong. It’s also the effect of getting lost inside our own minds. In one recent study, we showed that just a few hours of ACT reduced stress several months later, and it did it because people learned acceptance and mindfulness skills.
Burnout is just a more specific type of stress-related result, but it seems especially sensitive to cognitive entanglement. In one of our studies the tendency to take negative thoughts about work literally predicted burnout higher than stress itself. So when you have, say, that judgmental thought about your boss, being able just to notice that thought and focus on your work values can mean the difference between quitting and succeeding in that workplace.
It’s beginning to appear that even the most horrifying private experiences fit with this idea. Medications don’t completely remove hallucinations and delusions for most people with a psychosis. Yet in this country very little else is provided to these patients to help them cope with these frightening and disruptive experiences.
This lack of help is terribly inhumane—there is much we can do. If you have ever seen the movie A Beautiful Mind you understand the basics of what we try to teach in an ACT approach. We teach patients to just watch their hallucinations, to notice their own delusional thoughts, to focus on their values, and to keep their overt behaviors going. That package works. In two separate studies it has been shown that just two to five hours of ACT will reduce rehospitalization by 38 to 50 percent over the next four months. Who knows what we will be able to do with more extensive packages.
Prejudice is probably the single most important problem on the planet. The “War on Terrorism” should not just be a war on terrorism—it needs to be a war on intolerance since that is a big part of where terrorism comes from. Whether it’s killing the infidels, or the Catholics, or the Tutsis, it’s all a form of prejudice. But in the modern era, prejudice has enormously powerful tools at its disposal: bombs, chemicals, biological weapons. And we are not yet up to the worst of the list.
Let me ask you this. If there was a big red button in every home on the planet and if an adult pushed it the world would end, how long would the planet last? Not long. But once we have freely available suitcase bombs…and are we not close to that very situation? And how long before we have those bombs. Ten years? Twenty? Well, whatever your answer, that is how long we have to figure this out because that is the day we have a big red button in everyone’s house.
When a terrorist attacks an innocent human being he or she is revealing the end stage of a process of objectifying and dehumanizing others. But to some degree this same process underlies more usual phenomena such as prejudice based on ethnicity or gender or stigma associated with illness or appearance. Most approaches to stigma and prejudice are either educational—in one way or another telling others what to believe and do—or experiential, learning through direct contact with stigmatized groups. Unfortunately the effects of both are weak and unreliable. In one recent study done in a prison, education about racial differences actually increased racial conflict.
And these methods are not mindful of the issues we have been talking about. If you try to suppress a prejudiced thought you will increase its strength and psychological impact, not decrease it. We need another way forward. Yet we all have prejudiced programming—ethnic and gender biased jokes, for example. Even if our values are not racist or sexist, our minds sometimes are. It doesn’t matter your race or gender; we’re all swimming in this stream.
ACT shows another way forward. We have found that acceptance of prejudicial thoughts (as thoughts) and learning to just notice them mindfully while connecting with our values will increase people’s willingness to engage in non-prejudiced behaviors. We have shown it with prejudice toward substance abusers in recovery, ethnic prejudice, bias toward the mentally ill, and bias against science-based treatments. We will see how far it can go.
Shame and prejudice are really the same thing; one is just inwardly focused. Buying into “I’m bad” is really not different from buying into “you’re bad.” And it turns out that the same methods that help with prejudice and stigma also help with shame and self-stigma. ACT can help people increase job performance, too. Have you ever worked with someone who comes up with excuses anytime he or she needs to learn something new—a new telephone system, a new budgeting process, and so forth?
We’re learning that the same experiential avoidance process that ACT targets is part of this resistance. It’s obvious if you think about it. How did you feel when you first started to learn to dance, when you first skied, when you first put on ice skates, and so forth? Didn’t you feel a bit foolish and awkward? If you can’t allow that, how can you learn? We’ve found that our measures of experiential avoidance can predict what office workers will do at work: Our short questionnaires correlate with keystroke errors a year later because people who are high avoiders don’t learn the software well.
Why? Because they’re never willing to feel stupid or uncomfortable. ACT has been shown to undermine this avoidance, and as a result people are more willing and able to learn. In one recent study we showed that workers who had just been through an ACT workshop were then more willing and able to learn things that had nothing to do with ACT (in this study it was therapists learning to using certain medications in their work). And therapists were using these new methods more at a three-month follow up.
NHP: Some of this work is said to have come from your own battles with anxiety and panic. How did these ideas apply to your own struggles?
SCH: I had a panic disorder. At the height of it, my life shrank until I could not travel, get on an elevator, drive, go to a movie, get on a plane, or even talk on the phone without a tremendous struggle. It was clear to me that I had a choice: I could either lose my life as I knew it or I could learn to step forward into my fear. I went back into my behavioral training, my science training, my eastern training, my human potential training. ACT in some ways is my personal journey—it’s how I faced anxiety. But it’s not just me. Other major ACT researchers and writers are chronic depressives, heroin addicts, or social phobics, and they have poured these experiences into the work. That’s not by accident. When life has beaten you up, the uncommon sense in ACT begins to have appeal.
Sometimes people are just by their nature ready for this approach even when they’re young, but most of us start out thinking we can win the war with our minds and our history. And you might even get away with that view if nothing bad ever happens. When it does, though, you need to take a different path. When futility sets in you have a chance to do something new. I began to learn how to abandon the war with my mind and history.
I personally do ACT everyday. I do acceptance, defusion, mindfulness, and values work continuously. I know right now I might have anxiety attack. It’s been ten years since the last, but I know I can’t control that. It’s not up to me—it’s up to my history and my current situation. But what I can control and what only I can control is whether I will back up from my own experience. My pledge to myself is that I will stand with myself, regardless. If that means I get so anxious I can’t talk, right here, right now, that will be a problem—but if I stay true to my commitment, it will be your problem, not mine.
NHP: A lot of what you’re describing sounds Buddhist-inspired. How does ACT differ from Buddhism, both in theory and in the practice it requires?
SCH: Buddhism has a lot of wisdom in it, as do all of the major spiritual and religious traditions, but it emerged from pre-scientific times. Some of its specific ideas show that lineage; some of its methods require weeks, months, and years to work. ACT is in the same general psychological space, but it’s driven by a scientific theory, and its methods are designed to be quicker and more focused. I find it very encouraging that the two overlap because ACT did not come from Buddhism or any specific religious or spiritual tradition. It came from modern contextual psychology. If things from very different starting points overlap in their end points, to my mind this increases the chance that they’re both on to something.
NHP: How does ACT differentiate between pain and suffering?
SCH: Pain is just pain. We all have it—all the time if you just look. For example, we all know we will die. There is some pain in that knowledge, and you can contact that knowledge anytime, anywhere. But that alone is not suffering. If you add in unwillingness to feel pain, entanglement with your thoughts about pain, and loss of your valued actions—now you’ve amplified pain into suffering. I’ve seen that exact thing happen with thoughts about death, for example. But YOU did it. The pain didn’t do it. You see this in area after area: Anxiety + unwillingness to feel anxiety and keep moving in a valued direction = panic. Sadness, loss, anxiety, or anger + unwillingness to feel sadness, loss, anxiety, or anger while moving in a valued direction = depression. Pain + unwillingness to feel pain = trauma.
NHP: You’re a language researcher and chapter two of Get Out of Your Mind and Into Your Life is called “Why Language Leads to Suffering.” Can you tell us why you suggest that language is a source of human suffering?
SCH: We’ve learned four important things in our research. Human language and cognition is bidirectional, arbitrary, historical, and controlled by a functional context. Because language is bidirectional, words pull the events they’re related to into the present. Anywhere you go you can remember painful things. Just think of them. That is totally new on the planet, so far as we know. No other creature seems to do it. So it means we have orders of magnitude more pain than other creatures. And it’s arbitrary—what we relate isn’t dictated by form. Kick a dog and he’ll yelp—it’s dictated by form.
Show a person a beautiful sunset who has just had someone very near and dear die and that person may cry, wishing the lost loved one could be here to see it. The crying is not dictated by form—even beauty can create sadness. That means we can’t solve our problem with pain situationally. But because language is historical, we can’t win by changing the content of our cognitions. A person who thinks “I’m bad” and who then changes it to “I’m good” is now a person who thinks “I’m bad, no I’m good.” Where you start from is never fully erased—because you are a historical creature. Your mind is psychological, not logical. We make all of this so much worse by deliberate attempts to get rid of our history and its echoes—the automatic thoughts and feelings that emerge from our past. Because we’re historical creatures, these efforts elaborate whatever we’re trying to get rid of. Because human cognition is bidirectional, it mocks our attempts to change thoughts and feelings.
For example, suppose we need to get rid of anxiety because if we don’t bad things will happen. Anxiety is the natural response to bad things … so our efforts will tend to evoke anxiety, defeating our purpose. Fortunately, our work on cognition shows that the events that cause us to relate one thing to another are different than the events that give these relations functional properties. We take advantage of that in ACT. We change the functions of thoughts and feelings, not their form, and that makes all the difference.
NHP: You also say that research suggests many of the tools we use to solve problems lead us into the traps that create suffering. What does this mean?
SCH: Here’s how we solve problems: We use verbal processes to enable categories, time, and evaluation. “If I did that then this would happen, which would be good.” Notice all three are there: the categories and names of things and their features; time and contingency (if … then); and evaluation (this is better than that). This is great for problem solving. We see an imaginary future and evaluate it—all through the use of arbitrary symbols. It’s because of this ability that we took over the planet. Yet this alone is plenty enough to create psychological problems. “If I go to the mall, I will feel anxious, which is really bad.” Same processes: categories, time, and evaluation. “If my lover leaves me I won’t be able to function.” Same thing. “If I kill myself I will stop hurting.” Same thing. This is why you can’t weed out the processes that cause suffering—these same processes are at the root of our achievements as a species.
We need to learn how to use these processes when they’re helpful and let them lie dormant when they’re not. It’s very hard to do—like the delusions that follow Russell Crowe in the movie A Beautiful Mind— most of our most difficult experiences are there night and day begging us to taken them literally. But once we do we are lost. It’s hard to learn how to do nothing even when it’s only nothing that will do. Humans are terrible at that. We are terrible at letting go.
NHP: One of the premises of ACT is that avoidance of difficult emotions leads to suffering, which is highly counterintuitive. First, why do you say this and second, what do you say to someone who says that avoidance of pain is ingrained and automatic?
SCH: Let me take the last part first. The avoidance of pain is indeed ingrained and automatic. That is the point. So, sure, it’s absolutely normal to needlessly avoid pain. And there is nothing wrong with avoiding many forms of situational pain. There is no need to put your hand on a hot stove, for example. But historical pain is something else. If you have a painful memory, you’ll always have it and avoiding it will only distort your life because memories don’t go away. If you have a thought you don’t like, trying to make it go away is like trying not to think of a piece of chocolate cake … in the effort deliberately not to think it, you just did.
Here is why avoiding that kind of pain is problematic: First, the painful event doesn’t truly go away, it’s just avoided, and the next time it’s contacted it’s bigger and stronger and even more likely to control behavior. Second, it makes us attend all the more to this very pain. Like a noise in the background, as soon as it’s important that it go away, it’s now in the foreground and far, far worse that it was only moments before. Third, the very basis of avoiding painful thoughts or feelings is that the reaction is really bad—but that means that as we deliberately try to avoid things, we’re building them into more and more powerful events because we start this process with the embraced belief that they truly are dangerous.
We literally make our nightmares come true because the real damage is done the moment we take them literally. At that point they transform themselves from mere historical events—mere processes of the mind worth noting—into things that can control our lives. After all if they’re controlling efforts at avoidance they’re already controlling our lives.
NHP: You talk a lot about values in your book, and the “commitment” in acceptance and commitment therapy refers to making a commitment to living a values-based life. What does it mean to live a values-based life and how does it help reduce suffering?
SCH: Values are like directions on a compass. They’re never achieved, but in each and every step they influence the quality of the journey. Values dignify and make more coherent our life course—and they put pain in a proper context. It’s now about something. Let me go back to that movie A Beautiful Mind. It’s only when the hero has to decide between what he values and entanglement with insanity that it’s possible and sensible to accept the delusions; to notice them; and to abandon trying to control them—all in the service of being a husband, father, and a mathematician.
In the same way, we only put down our avoidance, addictions, and mental wars because it’s costing us something dear, whatever it is that we want our lives to be about. Without that cost we would be lost. It’s amazing how often people have never really thought about what they want in their lives. They’ve been fighting a mental war, waiting for life to start, and have never really asked or answered the question of what kind of a life they’re waiting to live.
The joyful vision of ACT is that you can start living that very life NOW, with your thoughts, feelings, memories, and sensations. You start that journey by asking what it is that you really want your life to be about. That is the point on the compass.
NHP: What kinds of techniques do you try to teach in ACT? Can you walk us through an ACT exercise?
SCH: Okay. First think of a painful thought, a self-critical thought, one of those nagging deep down familiar bits of negativity. Do you have one? ACT has scores of techniques that are designed to help you catch the word machine in flight rather than getting caught up in the world seemingly structured by it. These “defusion” techniques help us notice the process of thinking, not just their products.
So let’s try a few with that very thought. I’ll do them in rapid fire, but in the book we present all of this in more detail, and you can take the time you need to explore them properly.
First say that thought very fast over and over again, feeling your mouth as you say it and noticing how odd it sounds when said fast. Now say it slowly, one word on the inbreath and the next on the outbreath until it’s all said. Now sing the thought out loud. Be careful not to ridicule, satirize, or criticize your thoughts. Rather just notice as you sing that these are thoughts. Now say them in the voice of a politician from the opposite political party as you. Be careful not to ridicule, satirize, or criticize your thoughts. Rather just notice as you hear these words that these words are thoughts. You don’t have to do anything about them. Just thank your mind for the thought and notice what shows up.
These are four of literally hundreds of techniques ACT therapists have developed to liberate humans from the grip of their own cognition and emotion—but all without making the cognition or emotion go away. Once you’re on to it, you can come up with your own methods. In this new book we actually walk readers through that process. Once you see the model and its purpose it’s not hard. You can literally create your own methods to get out of your mind and into your life. So the book is not a new belief system. It’s a new context for living with that word machine we call our minds, without turning our lives over to it.
Salon.com Interview with Steven Hayes (February, 2006)
Salon.com Interview with Steven Hayes (February, 2006)Below you will find a link to the Salon.com interview with Steve.
https://www.salon.com/2006/02/25/happiness_4/
More likely, you will need to go to http://www.salon.com and search for "Steven Hayes" -- the first article should be this one.
Sunday Telegraph in the UK: Human Pain and Human Vitality (March, 2006)
Sunday Telegraph in the UK: Human Pain and Human Vitality (March, 2006)Here is a column that appeared in the March 5, 2006 Sunday Telegraph Human Pain and Human Vitality Nearly 30 years ago I had my first panic attack. A productive and reasonably successful young academic, I soon found myself struggling to give a lecture, to speak on the phone, or to ride in an elevator. From the outside I appeared calm – but on the inside I felt I was dying. Literally. Sitting still on a park bench my heart beat 165 times a minute as I fought a battle, not with a physical challenge requiring such blood flow, but with the word machine between my ears. Some of my experiences at the height of this struggle now seem so alien that it is only with difficulty that I can imagine the mindset that produced them. I’ll share one, knowing for many it may simply seem incomprehensible. An airline attendant stood at the front of a plane and described how to use the passenger seatbelts. I watched with a sense of amazement and incredulity, as one might gaze at an impossibly athletic feat during the Olympics. I remember thinking “how can she do that without being terrified?! She has to say all of those specific words, and they have to be right, and do it in front of a plane full of people!” Each of us compares our insides to others’ outsides, and our picture of the human condition is ever distorted as a result. That difference makes it believable that it is our birthright to be psychologically healthy, happy, and carefree – and that feeling good is the measure of a life well lived. Commercial interests are only too pleased to feed this vision, assuring us that we will approach it readily through the right car, home, or vacation. The pharmaceutical industry will provide the right pill; the media the latest “feel good” therapy; and the local bar both the ideal beer, and the setting to find the right romantic partner. It is seemingly only the abnormal person who suffers. The outsides of others provide superficial evidence of the validity of this vision. But what if everyone has a secret? And what if the joke is that we all have the same one? The fact is that almost all people are in pain somewhere in their lives much of the time. It is hard to be fully human. Almost all will struggle and suffer, and find that easy methods of feeling good bear little relationship to living a meaningful, valued, vital life. Anyone who reads the popular media, never mind the voluminous scientific literature on this topic, probably realizes that human problems are pervasive in the developed world. Few, however, seem to face the implications of such statistics considered as a whole. Over 30% of the population will have a psychiatric disorder sometime in their lives. Nearly 50% will struggle with thoughts of suicide for two weeks or more. Divorce rates reach similar levels; second marriages are no better; and the relationships that remain are often restricted or empty. If we add in the rates of emotional or physical abuse, sexual concerns, loneliness, burnout, problems with children, or 100 other such problems we need to consider the possibility that it is human pain is that is nearly universal. In effect it is abnormal to be “normal.” The treacle of modern “feel goodism” is simply false. That was my starting point, 25 years ago. Unable to control my anxiety, and sinking ever deeper into panic disorder as I tried to do so, I began to explore what it would be like to approach what I was struggling so mightily to avoid. I began to research whether it was the emotional and cognitive objects of my struggle that were my enemy, or struggle itself. We now know that one of the most pathological things a human being can do is to attempt to avoid their own thoughts and feelings, and to link their overt actions to this attempt. Researchers such as Frank Bond (University of London) have discovered that the psychological inflexibility that results from this effort produces bad outcomes almost everywhere you look. It predicts more anxiety, depression, worry, and trauma. It undermines your ability to learn new things, enjoy your job, be intimate with others, or rise to the challenges of physical disease. Lance McCracken (University of Bath) has shown that these processes predict far more disability due to chronic pain than the amount of pain or injury itself. Turned outward, the human mind is highly effective. We can predict the future and remember the past; we can evaluate outcomes based on imagined courses of action. It is these symbolic problem-solving abilities that have lead us to dominate the planet, despite being weak, slow, and vulnerable. But these same abilities also entangle us needlessly in a struggle with our own thoughts and feelings. If we don’t like dirt on the floor we can vacuum it up and the dirt will be gone. Conversely, if we don’t like a painful memory and try not to think it –we will make it more of a focus, more frequent, and more impactful. If we fear a future lack of food we can grow plants that will later nourish us. But if we fear the harm produced by future panic and thus try to avoid it, we will have brought that imagined harm into the present and amplified its role in our lives. The human mind has in effect been turned on its owner, merely by allowing it to do what it normally does, but in the wrong domains. It turns out that this is not necessary. We have developed methods to train people in a healthy alternative: accept feelings and be mindful of thoughts without arguing, coming instead into the present moment more consciously and fully, focusing on values and taking actions that move in their direction. For example, if the thought “I’m bad” is present, trying to change it only confirms that there is something unacceptable about you. In our approach we might instead say “bad” 100 times aloud, or sing the thought, or print it on a T-shirt and wear it, or say it in the voice of one’s least favored politician. Like the movie A Beautiful Mind, this defanged thought is then willingly brought along into valued actions, such as being a loving person, or contributing to others. Controlled research shows this these methods are helpful in areas as diverse as anxiety, burnout, diabetes management, smoking, pain, and depression among several others. I walk through these concepts and techniques in Get Out of Your Mind and Into Your Life (New Harbinger; 2005) which was the number one self-help book last week in the United States on Amazon. The basic and applied psychological science behind these methods will be presented for students, therapists, and researchers at a week-long “world conference” July 22-28 at the University of London (see www.contextualscience.org). For the first time in human history, we are trying to raise an entire generation on the message that feeling good equals living well. It is not true. It has never been true. And now we are seeing the sad results in our homes and on our streets. Our task as human beings is to learn how to carry pain without needlessly amplifying it into suffering, while creating a values-based life. Steven C. Hayes University of Nevada, Reno
Time Magazine: Happiness is Not Normal (2006)
Time Magazine: Happiness is Not Normal (2006)John Cloud wrote this article for Time magazine in February 2006, in which he described the contrast between 'third wave' approaches (specifically Acceptance and Commitment Therapy) and more traditional cognitive behavioral therapies.
For more information, see attached. Please note: You must be logged in as an ACBS member in order to view the content below.
For more discussions about the Time Magazine article, click here.
The Time Magazine story (2006)
The Time Magazine story (2006)There are a number of popular stories on ACT / RFT that have appeared. You can find the ACT ones in "About ACT / Communicating about ACT / Popular Media" but given the prominence of Time Magazine this one is listed here. The article in Time (Cloud, 2006) came out in the February 13, 2006 issue. It was pretty long -- 6 pages -- and dealt with ACT in some depth. It sent Get Out of Your Mind and Into Your Life into the top 25 books (and number 1 self-help book) on Amazon for nearly a month and is still reverberating in the form of stories in the popular media in various other outlets.
Some of the issues raised by the Time story are discussed in the child pages attached to this page.
--------------------------------------------------------------------------------------------------------------------------------
Happiness Isn't Normal
by John Cloud
February 13, 2006
Before he was an accomplished psychologist, Steven Hayes was a mental patient. His first panic attack came on suddenly, in 1978, as he sat in a psychology-department meeting at the University of North Carolina at Greensboro, where he was an assistant professor. The meeting had turned into one of those icy personal and philosophical debates common on campuses, but when Hayes tried to make a point, he couldn't speak. As everyone turned to him, his mouth could only open and close wordlessly, as though it were a broken toy. His heart raced, and he thought he might be having a heart attack. He was 29....
Is ACT a Cult? Is ACT Just a Fad?
Is ACT a Cult? Is ACT Just a Fad?These thoughts are in bullet point form from a power point presentation by James Herbert at Drexel University.
He gave this talk at the ACT Summer Institute at La Salle University in summer of 2005.
I've (SCH) tweaked it to make it more readable and understandable in this form.
Is ACT Just a Fad or a Cult? Addressing the Critics
James D. Herbert, Ph.D.
Drexel University
As ACT has moved into the mainstream, a variety of criticisms have emerged from within the academic community.
- As ACT becomes more popular, we can anticipate even more criticism from even more voices. The common theme is that
- ACT is merely the latest therapeutic fad to litter the mental health landscape.
The purpose of these points is to outline the criticisms so far, examine them critically and honestly, and explore how we as a community may respond.
There are a number of complaints about ACT. These include the following:
- Overly-hyped claims
- “Getting ahead of the data”
- Excessive enthusiasm among those interested
- ACT is a cult
- ACT has excessive and grandiose visions
- Proselytizing
- ACT as a “way of life"
- Promotes “undue influence” by seeking to identify principles and technologies that could be used to impact behavior without their explicit consent
- Experiential exercises in ACT training are coercive and manipulative
- There’s “nothing really new” here
- Premature dissemination to the public via self-help books
- Both ACT and especially RFT are plagued by obscurantist jargon
Let’s look at each of these in turn.
Getting Ahead of the Data
In order to evaluate this we must examine the evidential warrant of specific claims
Some critics have tried to say that the ACT community is making excessive claims based on the ratio of theoretical to empirical papers. But this means that mere interest would indicate excess. That is not fair. The ratio isn’t a proxy. Nor are dreams/visions
Some critics are clearly unaware of the data that exist (e.g., see Hayes, Luoma, Bond, Masuda, & Lillis, 2006); those who are correctly note that it’s limited, but don’t generally compare specific claims with evidence, or consider the research strategy being pursued.
In fact it seems that ACT proponents have in fact been appropriately cautious in claims
Our response: Continue to be clear about specific claims and back claims with evidence
Excessive Enthusiasm
This seems to be largely based on reactions to the listserv, and to reactions of some professors to their students returning inspired from workshops. But enthusiasm per se is only a problem if it interferes with critical thinking. Is there any evidence of this? If so, let's look at it, but so far the concerns do not seem to be linked to such interference.
Our response: Make sure not to be blinded by enthusiasm.
The “C” word: Is ACT a Cult?
“Cult” label usually evoked by:
- A closed system
- A charismatic leader, or if there is more than one, a very small group of such leaders hand picked by the main leader
- A strong profit motive
- Financial and/or sexual exploitation of vulnerable populations
- A hierarchy of secretive levels to pass through in order to gain special knowledge or status
- Intolerance of dissent
Such groups also:
- Challenge the status quo
- Offer a grand vision
- Engender high levels of enthusiasm
So is ACT a Cult?
The first set of features don’t apply. This website is an example; the list serve is an example. Anyone can participate and argue and have their say. But the second set of features clearly do apply. However, these latter features are poor discriminators of science vs. pseudoscience or cults.
Our response: This is silly; ignore it -- but also make sure that we maintain an open, horizontal, self-critical, empirical culture.
Grandiose Visions
Rightly or wrongly, ACT does indeed aspire to great things. Helps to understand history of behavioral analysis to appreciate the historical context. Behavior analysis always had a utopian vision (e.g., Walden II). It is critical to distinguish specific claims from distal goals and dreams; the former are subject to direct examination via evidential warrant; the latter are not.
Problem is that mainstream psychotherapies are cautious about big claims, whereas many dubious ones are not. So unless people look carefully, ACT can look too expansive.
Our response: Clarify explicitly the distinction between specific claims and distal visions.
Proselytizing ACT as a “Way of Life”
There are two variations of this: Clinicians must adopt an ACT perspective to their own life, and the focus of the client’s presenting problem is inappropriately shifted to ACT-consistent goals. Although ACT does suggest that clinicians try out some principles on themselves, it doesn’t require them to adopt any particular belief system.
Regarding clients, this is not unique to ACT, as all psychotherapies attempt to socialize the client to their model. The key in all cases is informed consent.
Our response: We could probably be clearer on these points, and we need to be cautious about things an individual clinical may do in applying ACT to her or her life and things that are said to be "necessary" in the absence of data. Individuals are free to explore -- claims can only be made based of scientific criteria.
ACT Seeks “Undue Influence” Over Others
This is a very familiar criticism to radical behaviorists. There are ethical issues surrounding parameters of informed consent that are an important cultural values. Like all values, must be decided independent of science per se. An extreme Libertarian stance rules out all public health interventions (e.g., programs promoting smoking cessation, safe sex to prevent STDs, routine diagnostic procedures like mammograms and prostate exams, childhood vaccinations). The fact that a technology could possibly be misused is no reason to stifle science.
Our response: Participate in the broader public ethical dialogue.
ACT Offers “Nothing New”
This is generally argued by those with minimal familiarity with ACT. Ironically, traditional CBT folks sometimes who make this argument have themselves been on the receiving end of this allegation from psychoanalysts and others. Many (though not all) techniques and strategies are indeed openly borrowed, and so aren’t new. What is new is the organizing model, and especially the close link with theory, a basic research program, and philosophy.
Our response: Point this out when challenged. Help others learn RFT, behavior analysis, and functional contextualism, and to see how this informs treatment development.
Experiential Exercises in Training Are Coercive and Manipulative
Experiential exercises are used in ACT to highlight consciously self-reflective nature of ACT. But we must remember the audience, and be very careful to avoid coercion, even implicitly. Degree of focus on experiential exercises remains an unresolved issue empirically.
Our response: Examine this issue openly within the community, ethically and empirically. Until this is worked out, be mindful of the issues, open to the concerns, and cautious.
Self-Help Books
There is a legitimate debate over appropriate threshold for direct dissemination via popular literature. On the one extreme some say you must have strongly supportive data, not only of general approach, but its effectiveness in the self-help format and for the specific problem in question. A growing number of ACT self-help books are being studied in randomized and open trials for effectiveness (as of 2011, we know of trials assessing Get Out of Your Mind, The Mindfulness and Acceptance Workbook for Anxiety, and Living Beyond Your Pain). Even outside of ACT, only a tiny number of books have that. At the other extreme: Anything goes. Reasonable people can disagree about this, but it is in no way unique to ACT.
Our response: Encourage authors to be appropriately cautious, while participating in the broader dialogue - and continuing assessing self-help book efficacy.
Obscurantist Jargon
Some critics see too many new terms in ACT and RFT, and reject them before learning these terms. The problem is that one person’s obscurantist jargon is another’s technical vocabulary. All other areas of natural science have technical languages. To evaluate jargon, must look at things like theoretical coherence, precision, scope, and connectivity. The ACT / RFT community has largely done this so far.
Our response: Develop the language as necessary, but be mindful of Occam’s razor. Distinguish scientific talk from clinical talk. Be prepared to defend the use of a technical term by showing that no existing term would do.
The Bottom Line
These criticisms fall into four camps. Those base on: Ignorance; style; a challenge to the status quo; and substantive issues. It is critical to distinguish these, as each calls for different responses.
Criticisms Based on Ignorance
Educate (e.g., journals, workshops, books, presentations), with a sensitivity to the audience
Criticisms Based on Style
Attempt to understand the reaction, and decide how to respond. We are not obligated to address every stylistic criticism. But we should be mindful of our audience and our purpose. Remind others that this tradition is not about individuals but a scientific model. If person X has the wrong style, focus on the message, not the messenger and evaluate the evidence.
Criticisms Based on Challenges to the Status Quo
Continue to do good science, including modifying theories and technologies based on data. Science is inherently self-correcting, so if ACT lives up to its promise it will eventually win hearts and minds. But be wary of striking the pose of Galileo; it isn’t enough to be novel – we must also be “right” in the sense of useful as considered against the goals of "prediction and influence with precision, scope, and depth"
Substantive Criticisms
Carefully consider substantive criticisms, especially those challenging the evidential warrant of specific claims and specific theoretical issues. Then, offer a thoughtful response, and remain open to change when appropriate based on arguments and data.
Steve's reactions to the Time article
Steve's reactions to the Time articleThe author did a terrific job, in my view. He starts out with a sentence that has me as a mental patient and finishes with a paragraph that says for ACT to go mainstream it will have to shed "its icky zealotry and grandiose predictions" but in between is a pretty serious effort to understand and explain.
I want to acknowledge John Cloud publicly. If every reporter treats this work as carefully and fairly we will be blessed. He is an honorable guy who worked really hard over several months to get it right.
The first thing John said was "I'm doing the RFT tutorial. I'm half way through it." I paused and replied "OK. If you are doing that, I'm there. If you are that serious I will answer every question and spend every ounce of energy needed to help you do your work." And I did. I was an open book (as you can see!). Some of what is in that story my mother did not know. But he earned that.
Of course, he is a writer, and writers need angles. The angle he chose was almost mythological: wild eyed rebel vs. the establishment. Even the photos fit that theme (me in a motorcycle jacket; in a tree fort; etc). So some of the basic science, the grants etc were deemphasized and things like bad clothes or weird rings were emphasized.
But, hey, in the grand scheme of things ACT is more outside than inside, so it was not a functional distortion to omit some things like that.
I apologize for the focus on me. That was not of my doing: John came to ABCT, interviewed Tim Beck, David Barlow, Judith Beck and many others. He went and saw talks by Kelly, Kirk, and many others. He then wrote the story as he chose. I suppose he felt that he needed to get people to care about the issue enough to read a very long story ... and he did that by putting my own struggles at center stage.
Mostly all other names in the ACT / RFT universe are not in the story. I did try repeatedly to push the names of researchers or co-authors (as John will attest!) but reporters just make their own calls on such things. And I wish he'd mentioned behavior analysis at least once (I begged!). But RFT is there by name; and some of the science is there. He does mention in a general way the students and the researchers and clinicians around the world. And the World Conference is mentioned! Woo Hoo. And the website is there ... which may be why you are reading this.
I am so thankful that there were no "anti" quotes from the ACT side about anyone. The story shows us (well, at least me) as a bit goofy, but not negative toward others. We took a few shots ... but that is to be expected I suppose.
Is this story premature? Maybe, but the culture decides on such things, and through accident and interest, here we are.
On the issue of grandiosity
No predictions are in there that are grandiose. What is in there is the willingness to see that the culture needs so much more from behavioral science than it is providing. I did say "Our survival really is at stake." That is so. Can anyone looking at the "war on terrorism" not realize that soldiers alone cannot do it? But that does not mean I think we can solve the problem. I did not say that and that is not in the quote. I just think we have to try. We have to try to solve the problem of hatred. We have to find a way to help people learn to love themselves and others, and to act in accord with their deepest values. And I do think we may have a possible path forward inside this work -- let's see. Together, let's see. That is a grand vision maybe ... but I'm not the only one dreaming. Who knows about outcome ... can we begin the process?
On the cult deal ... look for the other page and James Herbert's great talk on that given at the ACT Summer Institute.
My bottom line
In the long run what will matter is the substance: the science and the human value of the work we do. We will need every ounce of community and shared values and purpose we've gathered to do our work together as it becomes more visible and as the resulting centrifugal forces gather. The reason this work is being noticed is because of a community that cares. It is not a cult. There is no forced agreement. Look at this site! Anyone can post anything; and to be a member you just join. How much more open can a group be? I know of no other scientific group that is developing as an open community like this. How can a shared, open, self-critical community be a cult! It is just a fear word.
To the critics who say it, I say, join the group and post your views. You will find reason, support, and compassion here, not hierarchy.
So let's keep our eye on the horizon and remember why we got into this work in the first place. It was not about attention in magazines, nice though that might be. Unlike the fear expressed from by others outside of this community, it does not run on artificial agreement or hierarchy -- we need each of us to bring ourselves forward and to create something of value together. As individuals. Together.
Despite the worries, it seems clear we are entering into the conversation in a new way. That is an opportunity. It is also a burden. It will cut in multiple ways.
Could I also say on a personal level that I appreciate the support I've received in this process from many of you who have known it was going on. The letters and emails I am now getting from people who are suffering are enough to make me weep ... as my students have seen. Let's remember them. This work is about them.
Reacciones de Steve sobre la entrevista en la revista Time (traducción al español)
Reacciones de Steve sobre la entrevista en la revista Time (traducción al español)El autor hizo un trabajo excelente, en mi opinión. Comienza con una oración acerca de mí como paciente y termina con un párrafo que dice que para que ACT se haga popular tendrá que sacudirse su “fanatismo y predicciones grandiosas”, pero entre esas dos afirmaciones hay un serio esfuerzo por entender y explicar.
Quiero reconocer a John Cloud públicamente. Si cada reportero tratase su trabajo tan cuidadosamente y equitativamente podríamos sentirnos afortunados. Es una persona honorable y ha trabajado realmente duro durante varios meses para entenderlo bien.
La primera cosa que John dijo fue “estoy haciendo el tutorial de RFT. Voy por la mitad”. Yo me detuve y contesté “Ok, si estás haciendo eso, estoy aquí. Si estás tan comprometido voy a contestar cada pregunta y dedicar cada gramo de energía que sea necesario para ayudarte a hacer tu trabajo”. Y lo hice. Fui un libro abierto (como se puede ver!). Algo de lo que apareció en esa historia no lo sabía ni mi madre. Pero él se lo ganó.
Por supuesto, es un escritor, y los escritores necesitan ángulos. El ángulo que él eligio fue casi mitológico: rebeldes vs el orden establecido. Incluso las fotos encajan en ese tema (yo con una campera de motociclista, en un casa en un árbol). De manera que las partes de ciencia básica, las becas de investigación fueron minimizadas y cosas tales como la vestimenta o los anillos raros fueron enfatizadas.
Pero, ey, en el panorama general de las cosas ACT está más afuera que adentro, de manera que no fue una distorsión funcional el omitir esas cosas.
Me disculpo por el foco en mí. No fue obra mía: John fue a la ABCT, entrevistó a Tim Beck, David Barlow, Judith Beck y muchos otros. Y luego fue a ver charlas de Kelly [Wilson ], Kirk [Strosahl], y muchos otros. Y luego escribió la historia en la manera en que quiso. Supongo qu esintió que necesitaba que la gente se interesara en el tema lo suficiente como para leer una historia muy larga… e hizo eso poniendo mis propias luchas en primer plano.
La mayoría de los otros nombres en el universo ACT/RFT no están en la historia. Repetidamente intenté introducir los nombres de investigadores y coautores (y John puede dar fe de eso!), pero los periodistas toman sus propias decisiones al respecto. Y desearía que hubiese mencionado el análisis conductual al menos una vez (se lo rogué!). Pero RFT está mencionado; y parte de la ciencia está ahí. Menciona de manera general a los estudiantes, investigadores y clínicos que están por todo el mundo. Y se mencionan las Conferencias Mundiales! Woo hoo! Y el sitio web está ahí… lo que quizá sea el motivo de que estés leyendo esto ahora.
Estoy muy agradecido de que no hubiera citas “anti-“ del lado de ACT acerca de nadie. La historia nos muestra (bueno, me muestra a mí), como un poco torpes, pero no negativos hacia los otros. Recibimos algunos golpes…pero eso es esperable, supongo.
La historia fue prematura? Quizá, pero la cultura decide sobre esas cosas, y a través de accidentes e intereses, aquí estamos.
Acerca del tema de la grandiosidad.
No hay ninguna predicción nuestra que sea grandiosa. Lo que hay allí es la disposición a ver que la cultura necesita mucho más de la ciencia conductual que lo que se está proporcionando. Dije “nuestra supervivencia está en juego”. Esto es así. Puede alguien que esté viendo la “guerra contra el terrorismo” no darse cuenta que los soldados en sí no bastan? Pero esto no significa que crea que podemos resolver el problema. No dije eso y no está en la cita. Sólo creo que debemos intentarlo. Tenemos que intentar resolver el problema del odio. Tenemos que encontrar una manera de ayudar a que las personas aprendan a amarse a sí mismas y a los otros, y actuar de acuerdo con sus valores más profundos. Y creo que quizá tengamos un camino posible dentro de este trabajo –veamos si es así. Juntos, veamos si es así. Es quizá una gran visión… pero no soy el único que sueña. Quién sabe cuál será el resultado?... pero podemos empezar el proceso?
Respecto a lo del culto… busquen la otra página del sitio web y la charla de James Herbert en el ACT Summer Institute.
Mi línea final.
A largo plazo lo que importará es la sustancia: la ciencia y el valor humano del trabajo que hacemos. Necesitamos cada gramo de la comunidad, los valores compartidos y el propósito que hemos reunido para hacer nuestro trabajo juntos a medida que se vuelve más visible y como resultado de las fuerzas centrífugas que se van generando. La razón por la cual este trabajo está siendo notado es porque hay una comunidad que se interesa. No es un culto. No hay un acuerdo forzado. Vean el sitio web! Cualquiera puede postear cualquier cosa, y para ser un miembro sólo debes unirte. Cuánto más abierto puede ser un grupo? No conozco ningún otro grupo científico que se haya desarrollado como una comunidad abierta, tal como este. Como puede ser un culto una comunidad compartida, abierta y autocrítica? Sólo es una palabra temida.
A los críticos que dicen eso, les digo: unanse al grupo y publiquen sus opiniones. Encontrarán razón, apoyo y compasión allí, no jerarquías.
De manera que mantengamos nuestros ojos en el horizonte y recordemos por qué empezamos con esto. No fue para obtener la atención de las revistas, halagador como pueda ser eso. A diferencia del temor que albergan algunos fuera de la comunidad, ésta no se rige por acuerdos artificiales o jerarquías –necesitamos a cada uno de nosotros para avanzar y crear algo que valoremos entre todos. Como individuos. Juntos.
A pesar de las preocupaciones, parece claro que estamos entrando en la conversación de una nueva manera. Esto es una oportunidad. También es una carga. Repercutirá de múltiples maneras.
Podría agregar a título personal que aprecio el apoyo que he recibido en este proceso de parte de muchos de ustedes que sabían lo que estaba pasando. Las cartas y los emails que estoy recibiendo de personas que sufren son suficientes para hacerme sollozar… como han visto mis estudiantes.
Recordémoslos. Este trabajo es para ellos.
The Epilepsy study
The Epilepsy studyPsychology Today: Negativity: Don't Even Think of It (October 2005)
Psychology Today: Negativity: Don't Even Think of It (October 2005)Negativity: Don't Even Think of It
By: Kathleen McGowan
Summary:
With practice, you can learn to recognize your repetitive and negative thoughts. And keep them from becoming all-consuming. Life would be much easier if we had perfect control over our thinking -- especially where emotions are concerned. We could quickly forget about the people who make us frustrated or angry and allow disappointments to fade into the past without recriminations. But in reality, this kind of emotional equanimity is rare. Most of us spend a lot of time thinking over unpleasant feelings and mulling over regrets and resentments.
Unfortunately, many of these mental interpretations of our feelings make us feel worse about the situation. What started out as a small hurt or frustration, amplified by a thought process that focuses on pain and anger, may balloon into a major preoccupation. Our minds often repeat painful thoughts or scenarios over and over, even when we'd much rather let them go.
If you start paying attention to your interior monologue, you may find that you are dwelling on the ways your parents let you down, angry at someone who has hurt you, afraid of the challenges you face in the future, or ashamed that you haven't yet done the things you'd planned to in life. You'd rather stop all of these thoughts in their tracks -- but that's much easier said than done. Instead, you're left feeling as if there's something wrong with you: Why can't I just get over it? Why can't I just relax and be happy?
Generally, when you try to squelch one of these distressing trains of thought -- or "just get over it" -- your strenuous efforts to suppress it only make things worse. Research has shown that if we actively try to prevent anxiety-provoking or frightening thoughts, they generally become more powerful and harder to ignore. As a result, mental "fix-it" strategies generally backfire, whether that's trying to deny your unhappiness, avoiding the situations or people that make you anxious, or drinking to numb the feelings. Accepting the negative feelings and learning to distance yourself from the thoughts that amplify them can be a much more effective coping strategy, says psychologist Stephen Hayes of the University of Nevada in Reno.
In his book Get out of Your Mind and Into Your Life, he outlines a number of techniques from cognitive psychology that can help you resist getting lost in painful thoughts. With practice, you can learn to recognize your repetitive thoughts, and hold them at arm's length.
A few of Hayes' suggestions:
- Practice noticing your thoughts. Try to be conscious of where your mind leads you, and label the type of thought you're having to yourself. For example, if you've made a mistake at work and are feeling bad about it, think to yourself: "I've noticed that I'm focused on my error right now." If you're feeling stupid about the mistake, say to yourself: "Right now, I'm criticizing myself."
- If you find that one particular thought or phrase is running through your head -- I'm a loser" or "She screwed me over," for example -- try saying your troubling thought out loud, and either very slowly or in a funny voice. It seems silly, but by doing this, you're actively separating yourself from your mental soundtrack. You remind yourself that these thoughts are being generated out of a mental habit.
- Try thinking of your mind as just another organ of your body. If you find yourself preoccupied by fears, imagine that your brain is just like your hungry stomach when it rumbles, or your feet when they're tired after a long day. Think: "There goes my mind again, worrying about something trivial."
- Think of your self-destructive or self-critical thoughts as Internet pop-up ads. Don't criticize them or yourself for having them. Just think of them as unnecessary, meaningless noise. All of these tactics are ways to become aware of your inner mental monologue without either getting caught up in it or trying to shut it down. Distancing yourself from your difficult thoughts can help you learn to stop turning small problems into dilemmas that seem all-consuming or hopeless.
Martha Beck column in O magazine: Get a New Leash on Life (2001)
Martha Beck column in O magazine: Get a New Leash on Life (2001)Martha beck Column "Beck on Call" in "O" - The Oprah Magazine
From: http://www.oprah.com/omagazine/get-happy
An innovative therapy argues that acceptance is the route to happiness. Martha Beck brings you a new leash on life!
I'm trying an exercise designed by psychologists to help me gain my sanity by gently losing my mind. This process is utterly different from typical attempts to pursue happiness, most of which depend on controlling events and feelings.
Think of a problem that has plagued you for a long time—your weight, a loved one's bad habits, fear of terrorism, whatever. No doubt you've tried valiantly to control this issue, but are your efforts working? The answer has to be no; otherwise you would have solved the problem long ago. What if your real trouble isn't the issue you brood about so compulsively, but the brooding itself?
Psychologists who subscribe to acceptance and commitment therapy (ACT) call "clean" pain what we feel when something hurtful happens to us. "Dirty" pain is the result of our thoughts about how wrong this is, how it proves we—and life—are bad. The two kinds of suffering occupy different sections of the brain: One part simply registers events, while another creates a continuous stream of thoughts about those events. The vast majority of our unhappiness comes from this secondary response—not from painful reality but from painful thoughts about reality. Western psychology is just accepting something saints and mystics have taught for centuries: that this suffering ends only when we learn to detach from the thinking mind.
Judge not...
Learning to detach starts with simply noticing our own judgmental thoughts. When we find ourselves using words like should or ought, we're courting dirty pain. Obsessing about what should be rather than accepting what is, we may try to control other people in useless, dysfunctional ways. We may impotently rage against nature itself, even—perhaps especially—when that nature is our own.
This amounts to mental suicide. Resisting what we can't control removes us from reality, rendering our emotions, circumstances and loved ones inaccessible. The result is a terrible emptiness, which we usually blame on our failure to get what we want. Actually, it comes from refusing to accept what we have.
Victory by Surrender
Surrendering allows the truth to set us free. And how do we surrender?
I recently watched television interviews with two actresses, both in their late fifties. Each was asked if she'd found anything good about aging. Both snapped, "No. Nothing. It's horrible." A few days later, I saw Maya Angelou on TV. She said that aging was "great fun" and gleefully described watching her breasts in their "incredible race to see which one will touch my waist first."
"Sure, the body is going," she said. "But so what?"
Ms. Angelou has said many wise things, but I thought "So what?" was one of her wisest. It expressed the sweet detachment of someone who has learned how to rest in her real being and knows that it is made not of flesh or thought, but of love.
The Fruits of Acceptance
There is enormous relief in detaching from our mental stories, but in my experience, the results go well beyond mere feeling. Surrendering leads directly to our right lives, our hearts' desires. Whenever I've managed to release my scary stories and accept the truth of my life, I've stumbled into more happiness than I ever dreamed possible.
When I stop trying to control my mind—that verbose, paranoiac old storyteller—my thoughts become clearer and more intelligent. It's a delicious paradox: By not trying to control the uncontrollable, we get what we thought we'd get if we were in control. This thought pleases me greatly.
Still not happy? Your mind might be your biggest obstacle.
CBS
CBS
Scientific progressivity: Choosing a path
Contextual Behavioral Science (CBS) is the research paradigm underlying the development of ACT and RFT. It is a coherent, multi-leveled system of philosophical assumptions, scientific values, and methodological commitments that drive theory and technology development. It reflects an appreciation for our place in the history of science and specifies standards against which progress is assessed. What becomes clear from the history of science is that there is no such thing as The Scientific Method and no one measure of scientific progress. In such a context it is essential to take ownership of the foundations of your work.
Science is a relatively recent development in our evolutionary history, and for much of it methodology was guided by sets of assumptions that would now seem absurd to us. Up until the mid to late 17th century, for example, scientists in the Western world were committed to maintaining theories that placed the Earth at the center of the universe (Kuhn, 1957). Amazingly such systems enjoyed a great deal of success. Perhaps scientists of the future will look back upon 21st century science and see our work as similarly absurd and inexplicably successful. Studying the history of science can indeed be rather humbling. Were not those early 17th century scientists just as certain about their methods as we are about ours?
A healthy skepticism about science does not entail that no measure of progress is possible (Laudan, 1977). Instead it leads us to recognize that we must choose a measure of progress. We must choose a scientific tradition to work within. And we must take ownership of these choices as the world will not tell us which path to follow. CBS is one such path, complete with its own values and measures of progress. Papers have been published that explicate this system, for example:
A book-length introduction can be found here:
Zettle, R. D., Hayes, S. C., Barnes-Holmes, D., & Biglan, A. (Eds.) (2016). The Wiley Handbook of Contextual Behavioral Science. West Sussex, UK: Wiley & Sons.
For a basic introduction, it is useful to understand the following points (click each one for more information).
CBS:
- Is based on a pragmatic worldview known as functional contextualism.
- Grows from behavior analysis in its methodology and assumptions.
- Is committed to developing basic behavioral accounts of complex behaviors.
- Aims to apply these advances in the alleviation human suffering and the advancement of human well-being.
Click here for a list of general purpose books on CBSContextualism
ContextualismPhilosophy consists of the pre-analytic assumptions and rules of evidence (or criteria for truth) that are used to create, assess, and evaluate knowledge claims and theories. There are many different ways to describe, interpret, and understand the events of our world, and philosophy guides how we choose to speak about these events. While philosophical assumptions are often left unstated, particularly in science, being clear and open about one's philosophical position can improve coherence, reduce misunderstandings, avoid pointless debate, and allow more productive comparisons and evaluations of theories.
The brand of psychology presented on this website is based on a philosophical worldview known as contextualism. In particular, it is based on a philosophy of science known as functional contextualism. Click on the links below to learn more about this philosophy and how it guides our science.
About Contextualism
About ContextualismIn his 1942 book World Hypotheses: A Study in Evidence, philosopher Stephen Pepper noted that philosophical systems tend to cluster around a few distinct "world hypotheses" or "world views." Each world view is characterized by a distinctive underlying root metaphor and truth criterion. Root metaphors are based on seemingly well-understood, common-sense, everyday objects or ideas, and serve as the basic analogy by which an analyst attempts to understand the world. Truth criteria are inextricably linked to their root metaphors, and provide the basis for evaluating the validity of analyses. While the details of Pepper's analysis are open to debate, his framework can prove very useful for revealing the essential components, assumptions, and concerns of different discourse communities. Pepper identifies only four "relatively adequate" world hypotheses, with adequacy determined by the world view’s degree of precision and scope. Precision refers to the number of ways a particular phenomenon can be explained by a world view’s concepts (the fewer, the better), and scope refers to the number of phenomena that can be explained using those concepts (the more, the better). All world hypotheses strive to achieve complete scope with absolute precision, but none fully reach this ideal. These four world views, however, come the closest: formism, mechanism, contextualism, and organicism. The vision of psychology represented on this website is based on contextualism. It is a world view in which any event is interpreted as an ongoing act inseparable from its current and historical context and in which a radically functional approach to truth and meaning is adopted. These two aspects represent contextualism’s root metaphor and truth criterion, respectively. Contextualism has its roots in philosophical pragmatism, and is also closely related to the view known as selectionism. To learn more about contextualism, clink on a link below.
Root Metaphor
Root MetaphorThe root metaphor of contextualism is often called the act-in-context or the historic event (Pepper, 1942, p. 232), and refers to the common-sense way in which we experience and understand any life event. Consider the simple event of brushing your teeth. What is our common-sense understanding of such an event? First, the event consists of a host of related features that all mutually define the event.The root metaphor of contextualism is often called the act-in-context or the historic event (Gifford & Hayes, 1999, p. 289). Of course, we could also analyze the act of "brushing your teeth" as a collection of individual components. But our everyday experience and understanding of the act is one of a complete and whole event, inseparable from its context. Our common-sense understanding of an event also includes a sense of the purpose, meaning, and function of the event, and all of these depend on past events—or the historical context of the present event. For example, you probably brush your teeth because you’ve been told that doing so will prevent tooth decay, or because not doing so has resulted in painful visits to the dentist, or because you are getting ready for a date, or because your mother or father asked you to clean your teeth. Likewise, you may brush your teeth in the bathroom because you’ve found it convenient to do so in the past, and you’ve probably learned that a toothbrush and toothpaste are good equipment to use for this task, and that a circular motion is effective. All of these past events or life experiences, and more, contribute to an everyday understanding of why and how you brush your teeth. This is why context in contextualism refers to both the current and historical context of an act. It seems Pepper was basing his use of the term "context" on Dewey’s notion of context as "the historical situatedness of the meaning and function of behavior" (Morris, 1997, p. 533). Contextualists analyze all phenomena as acts-in-context. Events and their contexts are separated into different parts by contextualists only to achieve some practical purpose. truth criterion of contextualism.
Truth Criterion
Truth CriterionAn analysis based on contextualism’s root metaphor essentially consists of a description of some event or phenomenon and its current and historical context. Such an analysis is evaluated by examining—not surprisingly—the context in which it was generated. In particular, contextualists determine the validity or "truth" of an analysis by looking at the purpose or function of the analysis. If the analysis includes enough features of the context to successfully achieve the goal of the analysis, then it is deemed "true." In other words, for contextualists the truth and meaning of an idea lies in its function or utility, not in how well it is said to mirror reality. The truth criterion of contextualism is thus dubbed successful working, whereby an analysis is said to be true or valid insofar as it leads to effective action, or achievement of some goal.
This notion of truth reveals contextualism’s roots in philosophical pragmatism, a tradition heavily influenced by the work of figures such as Charles Sanders Pierce, William James, Oliver Wendell Holmes, Jr., George Herbert Mead, and John Dewey. Pragmatists and contextualists are not concerned with the existence of absolute, foundational truths or assumptions about the universe. As James wrote, "the truth of an idea is not a stagnant property inherent in it. Truth happens to an idea. It becomes true, is made true by events" (1907, p. 161).
For the contextualist, ideas are verified by human experiences, with an idea’s "meaning" essentially defined by its practical consequences, and its "truth" by the degree to which those consequences reflect successful action. Contextualism’s extremely functional approach to meaning, with a heavy emphasis placed on the empirical consequences of ideas, reveals the influence of another figure who greatly affected the development of pragmatist thought: Charles Darwin. Pragmatism can be seen as an application of Darwin’s selectionism to epistemology: In pragmatism, ideas are "selected" (to be retained as true or valid) if they lead to successful action, just as in natural selection traits are "selected" (to be retained by the species) if they lead to reproductive success. This influence is not surprising, as Darwinism was just gaining widespread appeal among scholars during the era in which the early pragmatists were cutting their intellectual teeth (Menand, 2001).
Varieties of Contextualism
Varieties of ContextualismAnalytic goals are vitally important to the contextualistic world view. This is because the analytic tools of contextualism—its root metaphor and truth criterion—both hinge on the purpose of the analysis, and neither can be mounted effectively without a clearly specified analytic goal. (Reese, 1993, p. 77).
Likewise, the root metaphor of the "act-in-context" is rendered meaningless in an analysis without an explicit goal because there would be no basis on which to restrict the analysis to a subset of the infinite expanse of the act’s historical and environmental context (Hayes, 1993b). Without a clear analytic goal, the contextualist could analyze the endless context of an act in perpetuity, without ever knowing when the analysis was complete or good enough to be deemed
Contextualists can, and do, adopt different analytic goals, and the many different varieties of contextualism can be distinguished by their goals. Based on their overarching analytic goals, contextualistic theories can be divided into two general categories: descriptive contextualism and functional_contextualism
| Descriptive Contextualism | Functional Contextualism | |
| Example | Social Constructionism | Behavior Analysis |
|
Analytic goal |
To understand the complexity and richness of a whole event through an appreciation of its participants and features | To predict and influence events with precision, scope, and depth using empirically-based concepts and rules |
| Knowledge constructed | Personal, ephemeral, specific, local, and spatiotemporally restricted (e.g., a historical narrative) | General, abstract, and spatiotemporally unrestricted (e.g., a scientific principle) |
| Content and focus | Individual-in-context | Behavior-in-context |
| Preferred methods | Qualitative and narrative | Quantitative and experimental |
| Disciplinary type | Natural history | Natural science |
Descriptive Contextualism
Descriptive ContextualismDescriptive contextualists seek to understand the complexity and richness of a whole event through a personal and aesthetic appreciation of its participants and features. This approach reveals a strong adherence to the root metaphor of contextualism and can be likened to the enterprise of history, in which stories of the past are constructed in an attempt to understand whole events. The knowledge constructed by the descriptive contextualist is personal, ephemeral, specific, and spatiotemporally restricted (Morris, 1993).Descriptive contextualists seek to understand the complexity and richness of a whole event through a personal and aesthetic appreciation of its participants and features. This approach reveals a strong adherence to the root metaphor of contextualism and can be likened to the enterprise of history, in which stories of the past are constructed in an attempt to understand whole events. The knowledge constructed by the descriptive contextualist is personal, ephemeral, specific, and spatiotemporally restricted (Morris, 1993). Like a historical narrative, it is knowledge that reflects an in-depth personal understanding of a particular event that occurred (or is occurring) at a particular time and place. Most forms of contextualism, including social constructionism, dramaturgy, hermeneutics, and narrative approaches, are instances of descriptive contextualism. Descriptive contextualism is strong in its adherence to contextualism’s root metaphor of the act-in-context, but suffers from several weaknesses. The analytic goals of descriptive contextualists are somewhat ill-defined, and it is difficult to determine when such goals gave been accomplished. This problem is openly acknowledged by many descriptive contextualists (e.g., LeCompte, Millroy, & Preissle, 1992, p. xv). In addition, a personal, holistic appreciation of a specific event and its context may or may not yield any practical knowledge or benefits (Hayes, 1993b).
Functional Contextualism
Functional ContextualismFunctional contextualists seek to predict and influence events using empirically-based concepts and rules (Biglan & Hayes, 1996; Hayes, 1993b; Gifford & Hayes, 1999). This approach reveals a strong adherence to contextualism’s extremely practical truth criterion and can be likened to the enterprise of science or engineering, in which general rules and principles are used to predict and influence events. Rules or theories that do not contribute to the achievement of one’s practical goals are ignored or rejected. Knowledge constructed by the functional contextualist is general, abstract, and spatiotemporally unrestricted (Morris, 1993). Like a scientific principle, it is knowledge that is likely to be applicable to all (or many) similar such events, regardless of time or place.
In psychology, functional contextualism has been developed explicitly as a philosophy of science (Biglan, 1995; Gifford & Hayes, 1999; Hayes, 1993b). Specifically, it has been offered as the philosophical basis of the field known as <em>behavior analysis</em>. From the perspective of functional contextualism, behavior analysis is a natural science of behavior that seeks "the development of an organized system of empirically-based verbal concepts and rules that allow behavioral phenomena to be predicted and influenced with precision, scope, and depth" (Biglan & Hayes, 1996, pp. 50-51). By studying the current and historical context in which behavior evolves, behavior analysts strive to develop analytic concepts and rules that are useful for predicting and changing psychological events in a variety of settings. These same concepts and rules can also be used to describe and interpret psychological phenomena for which prediction and influence are presently impractical or impossible (Biglan & Hayes, 1996; Skinner, 1974).
The behavior-analytic approach to studying psychological events can be described as selectionistic. Essentially, "behavior analysts think of the shaping of behavior as working in just the same way as the evolution of species" (Baum, 1994, p. 64). In biological evolution, contingencies of survival in a given environment select which genetic traits will persist in a species; in behavioral evolution, contingencies of reinforcement in a given context select which class of responses will persist (or be likely to occur) for an individual. Both the evolution of species and the evolution of behavior can be described as selection by consequences (Skinner, 1981), and the same process has also proven useful for interpreting the evolution of cultural practices (Biglan, 1995; Harris, 1979; Skinner, 1981). Indeed, behavior analysts consider human behavior to be "the joint product of (a) the contingencies of survival responsible for the natural selection of the species and (b) the contingencies of reinforcement responsible for the repertoires acquired by its members, including (c) the special contingencies maintained by an evolved social environment [a culture]" (Skinner, 1987, p. 55). Contextualism and selectionism are closely related concepts, with selectionism being the causal mode inherent to contextual philosophy. Selectionism involves an emphasis on the role historical context and consequences play in shaping the form and function of the phenomenon of interest in the current setting—an emphasis that clearly reflects both the root metaphor and truth criterion of contextualism.
Implications of Functional Contextualism's Analytic Goal
Adopting the analytic goal of the prediction and influence of psychological events leads to several important ramifications for a psychological science. In fact, many of the distinctive characteristics of behavior analysis as a contextualistic science developed directly from this overarching goal. Behavior analysts’ rejection of mentalistic and cognitive explanations for behavior, emphasis on functional relations between behavior and environmental events, and preference for experimental research methods can all be linked to the field’s ultimate purpose. It is important to recognize that prediction and influence form a single goal, and functional contextualists thus value analyses that allow both the prediction and influence of psychological events. They seek to identify variables that "predict the event in question and would, if manipulated, affect the probability, incidence, or prevalence of the event" (Biglan, 1995, p. 34). Analyses which only allow the prediction of behavior, or which rely on variables that are not manipulable (at least in principle), are considered inadequate or incomplete.
Much of the research in psychology and education is based on the development of models that describe how hypothetical constructs and mediating cognitive (or neural) mechanisms determine overt behavior (Biglan & Hayes, 1996). These models generally attribute behavioral events to factors such as a person’s cognitive schema, information-processing mechanisms, brain activity, learning style, attitudes, expectations, knowledge constructions, emotions, thoughts, or feelings. Although these models can be quite accurate predictors of psychological events, they are not very helpful to those who also wish to know how to influence or change psychological events. When one type of psychological event is said to cause or explain another, with limited reference to the impact of environmental or historical variables, we are left with little knowledge of how to change or influence either type of psychological event. To change or influence the behavior or psychological events of another person, we must search for manipulable variables in the environment. Why? Because we are part of that other person’s environment. Anything we could possibly do to affect the performance of an individual, such as deliver psychotherapy or education, occurs in the environment of that individual—in the context of his or her behavior (Hayes & Brownstein, 1986).
In addition, the purported "causes" of behavior in cognitive and mentalistic models are themselves psychological events that require explanation. What caused the attitude, for example, and how can we change it? Once again, behavior analysts search for the answers to such questions in the environment, or—more specifically—in an individual’s lifelong history of interacting with his or her environment. Cognition and other internal events are interpreted by appealing to a person’s learning history, rather than assuming they are underlying processes causing and controlling overt behavior. To put this perspective in terms that may seem less controversial, behavior analysts simply believe that people learn how to think, reason, plan, construct meaning, problem-solve, and more through interactions with their natural, social, and cultural environments. Thus, behavior analysts attempt to identify aspects of the manipulable environment that influence the occurrence, incidence, prevalence, or probability of both private and overt psychological events.
The most effective strategy for identifying variables that both predict and influence behavior is controlled experimentation: events in the context of the behavior are manipulated in a systematic manner, and the resulting effects on the behavior’s occurrence are observed (Biglan, 1995; Hayes, 1993b). This orientation allows researchers to isolate which features of the context are functionally related to changes in the psychological event; purely descriptive or correlative research generally does not provide such knowledge. In behavior analysis, these procedures have traditionally involved the intensive study of individual organisms with time-series (or repeated measures) methodology (e.g., Barlow & Hersen, 1984; Sidman, 1960). While functional contextualists favor experimental techniques, they encourage the use of a diverse set of methodologies, provided that value is always measured against pragmatic goals (Biglan & Hayes, 1996). Group designs using between-subject comparisons can be employed effectively for the purposes of functional contextualism, for example, and even correlational or predictive research of the sort described above can provide clues about contextual variables that might impact behavior. Qualitative methodologies also have their uses in functional contextualism, but are not as effective as experimental procedures for testing the influence of environmental variables on behavior or for verifying the general utility of principles.
A Silly Poem About Contextualism and Behaviorism
A Silly Poem About Contextualism and BehaviorismWhy is Contextualism "a-ontological" and Why is Behavior Analysis Contextualistic?
Why is Contextualism "a-ontological" and Why is Behavior Analysis Contextualistic?Dermot Barnes-Holmes's fun PowerPoint (the BA pdf) below describes answers to both of these questions.
For a detailed paper on this general topic you might start with Hayes, S. C., Hayes, L. J., & Reese, H. W. (1988). Finding the philosophical core: A review of Stephen C. Pepper's World Hypotheses. Journal of the Experimental Analysis of Behavior, 50, 97-111. Like most key ACT / RFT / CBS publications it can be downloaded from the publications list on the site but for convenience it is attached below.
Contextualism FAQ
Contextualism FAQACBS Members: To provide a question and an answer to this FAQ, click on the "add child page" link at the bottom of this page.
Is contextualism synonymous with functional contextualism?
Is contextualism synonymous with functional contextualism?No. There are different types of contextualism based on their specific goals. Many forms of contextualism (such as hermeneutics, dramaturgy, social constructionism and so on) are forms of descriptive contextualism which seek to appreciate the participants in the whole. Functional contextualism has as its goal the prediction and influence of behavioral interactions with precision, scope, and depth. The best way to understand the difference is to go to the publications pages and download articles on contextualism. You need to be an ACBS member to do that, but it is cheap so the best thing to do is just to click here to learn how to join.
Education
EducationThe contextual approach to psychology presented on this website has important implications for educational practices. For example:
- Functional contextualism provides a coherent framework for developing a pragmatic science of learning and instruction. It also shares the same philosophical world view as most forms of constructivism, a perspective that dominates the educational landscape in America (Fox, 2006).
- Relational Frame Theory (RFT) outlines the kinds of core processes that may be key to the intellectual and social development of humans, and provides a technical language for analyzing most forms of complex human behavior. As such, RFT has important implications for both what we teach and how we teach. While RFT-based approaches to education are only recently beginning to be explored (e.g., Ninness et al., 2005; Strand, Barnes-Holmes, & Barnes-Holmes, 2003), the theory and its related research hold tremendous promise in this area.
- Acceptance & Commitment Therapy (ACT) is sometimes called Acceptance & Commitment Training when used in an educational context to emphasize its applicability beyond traditional therapeutic settings. At its core, ACT is focused on teaching people to be psychologically flexible and to live valued, meaningful lives. This focus overlaps broadly with several common educational goals, including the teaching of critical thinking, problem solving, reasoning, values, and "life skills." In addition, ACT may enhance instruction by helping individuals of all ages learn to "sit with" the discomfort of learning new or difficult things (e.g., Bond & Bunce, 2000) and by helping them value education as it relates to their own life goals and values.
Related Philosophical Systems
Related Philosophical SystemsChaos Theory versus control and univocal understanding of human beings. La théorie du chaos versus le contrôle
Chaos Theory versus control and univocal understanding of human beings. La théorie du chaos versus le contrôleThanks to Dr Pierre Cousineau who brought me on the explorative track of the Chaos Theory. Even if there are differences with contextual psychology, there are also similarities. Thanks to the mind too for those derived relational frames. Cannot do without it, so useful sometimes!
This video talks about seeking control, unpredictability, present moment and ..... It is summarizing chaos theory with some links to psychology. In english subtitled in french (approximately 9 minutes)
http://www.dailymotion.com/video/x5y2jh_la-theorie-du-chaos_news
Merci à Dr Pierre Cousineau ne m'avoir mise sur la piste de la théorie du chaos. Même s'il y a des différences avec la philosophie contextuelle, certains éléments s'en rapprochent. Ce vidéo est sous-titré en français et donne une vue d'ensemble de la théorie en lien avec la psychologie.
Pragmatism
PragmatismPragmatism is a largely American system of philosophical thought popularized by William James. It is related to contextualism in that it shares the same truth criterion of successful working. Feel free to add to this page if you are a fan.
Links
- The BBC has recently run a radio show on pragmatism that is pretty interesting and a good introduction to pragmatism. You can listen to it online if you are interested in the theory or a bit of its history.
Suggested Readings
Suggested Readings- Barnes-Holmes, D. (2000). Behavioral pragmatism: No place for reality and truth. The Behavior Analyst, 23, 191-202.
- Biglan, A. (1995). Changing culture practices: A contextualistic framework for intervention research. Reno, NV: Context Press.
- Biglan, A., & Hayes, S. C. (1996). Should the behavioral sciences become more pragmatic? The case for functional contextualism in research on human behavior. Applied and Preventive Psychology: Current Scientific Perspectives, 5, 47-57.
- Fox, E. J. (2006). Constructing a pragmatic science of learning and instruction with functional contextualism. Educational Technology Research & Development, 54(1), 5-36.
- Gifford, E. V., & Hayes, S. C. (1999). Functional contextualism: A pragmatic philosophy for behavioral science. In W. O’Donohue & R. Kitchener (Eds.), Handbook of behaviorism (pp. 285-327). San Diego: Academic Press.
- Hayes, S. C. (1993). Analytic goals and the varieties of scientific contextualism. In S. C. Hayes, L. J. Hayes, H. W. Reese, & T. R. Sarbin (Eds.), Varieties of scientific contextualism (pp. 11-27). Reno, NV: Context Press.
- Hayes, S. C., Hayes, L. J., & Reese, H. W. (1988). Finding the philosophical core: A review of Stephen C. Pepper’s World Hypotheses. Journal of the Experimental Analysis of Behavior, 50, 97-111.
- Morris, E. K. (1988). Contextualism: The world view of behavior analysis. Journal of Experimental Child Psychology, 46, 289-323.
- Morris, E. K. (1993). Contextualism, historiography, and the history of behavior analysis. In S. C. Hayes, L. J. Hayes, H. W. Reese, & T. R. Sarbin (Eds.), Varieties of scientific contextualism (pp. 137-165). Reno, NV: Context Press.
- Pepper, S. C. (1942). World hypotheses: A study in evidence. Berkeley, CA: University of California Press.
Teaching Resources
Teaching ResourcesBelow you will find resources for teaching contextualism, functional contextualism, and philosophy of science in general. Please note that many of these resources include file attachments that are only visible/downloadable to ACBS Members.
ACBS Members: To contribute additional resources to this section, click on the "add child page" link below.
A Philosophy of Science for Psychology
A Philosophy of Science for PsychologyThis is a presentation on philosophy of science I use for my courses at the National University of Ireland, Maynooth.
Introduction to Basic Assumptions
Introduction to Basic AssumptionsThese materials were developed for the second day of a undergraduate learning class. Many times during the semester a student will try to argue statements from the book (Catania, 1997) or class. Some of the time, these arguments are not about the data or statements but rather they are about differences in basic assumptions. I wanted a short-hand way of pointing this out (e.g., “yellin’ across islands”) so we can get back on track quickly – without having to spend a lot of class time telling them they could be right, just not in the context of the basic assumptions for the class. This is my attempt to accomplish that. Much of the material and slides are, as Eric put it, "blatantly stolen" from other people, including: Steve Hayes, Kelly Wilson, & Eric Fox. Your suggestions, comments, and criticisms are welcomed.
Role of Theory and Philosophy in Behavior Analysis
Role of Theory and Philosophy in Behavior AnalysisThis is a PowerPoint file I used when teaching my Skinner's Behaviorism graduate course here at Western Michigan University. I used it at the end of the class when students' heads were swimming with words like ontology, epistemology, contextualism, truth criteria, theory, philosophy, etc. and wondering what the hell the purpose and relevance of it all was. :) It was sort of my attempt to summarize the role and importance of theory and philosophy in behavior analysis. I should note that this was presented at the end of the course, and summarizes key issues we had been discussing and reading about all semester. It is probably less effective as a first-time introduction to these topics. Much of the content of the slideshow is based on Steve Hayes's work, and some of the examples are blatantly stolen from lectures he gave in an applied research methods course I took with him at the University of Nevada. I'm a damn academic bandit. A pedagogical pilferer. A scholarly shoplifter. A pedantic plunderer. A person who needs to get more sleep before posting weird things to this website.
Behaviorism and Private Events
Behaviorism and Private EventsHow can you be a behaviorist and embrace private events?
Behaviorism was originally a movement against consciousness as the subject matter of psychology and introspection as the method of its investigation. Watson (1924, e.g., p. 14) claimed behavior as the subject matter of psychology and defined it by its form: behavior was muscle movements and glandular secretions. From his perspective, all activities of the organism could be reduced to these events (a kind of metaphysical behaviorism); and even if mental or other non-movement activities existed, they could not constitute the subject matter of a scientific psychology because public agreement as to their occurrence was impossible (a kind of methodological behaviorism). Thus for Watson, scientific legitimacy was an issue of public observability.
Skinner deviated considerably from these views. Skinner distinguished the subjective/objective dichotomy (which he thought to be of fundamental scientific importance) from the private/public dichotomy (which he thought was not fundamental). Skinner, in his 1945 paper on operationism, defined scientific observations as those under the control of a certain kind of contingency. Only when an observation was controlled by particular stimulus events (largely those of a nonverbal sort) and a general history of reinforcement for speaking under the control of those events, as opposed to control by audience factors, states of reinforcability, and so on, was the observation scientifically valid. As such, observations could be private and objective (scientifically legitimate) or public and subjective (scientifically illegitimate), depending upon the contingencies controlling the observations. This is the sense in which "radical behaviorism" is radical or "to the root": Even its core concepts and observations are defined in terms of contingencies, specifically, those bearing on the behavior of the scientist. Skinner rejected methodological behaviorism because he did not believe that public agreement provided assurance of proper contingency control.
As in the example above, it is easy to find instances where whole groups of observers are similarly influenced by motivational states and other subjective conditions. But in solving this problem by way of contingency analysis, Skinner opened up behaviorism to the very thing Watson was trying to eliminate: Introspective observations of private events. For example, Skinner said that radical behaviorism "does not insist upon truth by agreement and can therefore consider events taking place in the private world within the skin. It does not call these events unobservable" (Skinner, 1974, p. 16).
In a fundamental sense, radical behaviorism is not part of the tradition of "behaviorism" at all because all psychological activities that are contacted in a scientifically valid manner are subject to analysis. Thus contextual behavioral psychologists use the term "behavior" to mean something more like "psychological activity" than "behavior as distinct from thoughts and feelings." Skinnerians did not move rapidly to investigations of thinking and feeling for another reason, however. Skinner felt that an understanding of private events was not necessary for a scientific understanding of overt activity. He made that claim in essence because of his analysis of language in which the behavior of the listener is not verbal. From an RFT prespective this was an error and RFT corrects it. According to RFT, understanding thinking in the form of relational operants is essential to an understanding of overt human activity in most situations.
CBS and Behavior Analysis
CBS and Behavior AnalysisIn essence, Contextual Behavior Science is part of an effort to create a new form of what has traditionally been called behavior analysis. We could just use that label, but unfortunately it is so widely misunderstood that ears simply close. The word "behavioral" can be a huge barrier.
Furthermore, it is dangerous to use that label because behavioral psychology contains conflicting elements. It is possible and even easy to find well-known behavior analysts who believe and say things that are fundamentally at odds with functional contextual psychology or any of the other behavioral sciences. Furthermore, behavior analysis itself begins to take on a very different appearance when you add in a comprehensive functional contextual account of language and cognition. RFT research is showing that almost every behavioral principle we know can be transformed by relational operants. As the work deepens, it is becoming more and more obvious that the new behavior analysis that emerges in the wake of RFT is at times almost unrecognizable, not because that was the purpose but because that is how profound the implications are to that tradition of an adequate account of language and cognition.
Nevertheless, it seem important to note that much of the work in the tradition represented by this site has been done within behavior analysis. The first RFT and ACT talks ever given were given at the Association for Behavior Analysis International (ABAI), and the ABA program is filled with ACT and RFT work. We invite people who would never think of themselves as "behaviorists," and yet for whom the world of ACT and RFT resonates, to come to a ACBS World Conference or a conference of similar societies world wide. You will be very comfortable with the contextualistic work presented at such meetings.
That is one reason we do not simply present the ACT / RFT work as behavior analytic, and why we have created the Association for Contextual Behavioral Science (ACBS) to further this work. The wheel is still in spin and it is not yet clear if behavior analysis writ large will fully embrace what it has produced. And there is no reason to have to be responsible for everything that goes on under that label, and to accept the barriers and misconceptions that come along with it. For example, why accept the almost universal belief that behavior analysts don't care about cognition, when RFT is one of the most viable and productive empirical approaches to cognition in modern psychology?
Nevertheless, teaching in behavioral concepts has gotten so weak that even very bright and open psychologists can go through their training without grasping the meaning of behavioral principles viewed contextualistically. You do need to know behavioral principles to understand ACT and RFT. In this section of the site we will help begin that process for those with limited contextual behavioral training.
ACBS has a Clinical Behavior Analysis Special Interest Group (SIG) that ACBS members can join.
Resources for Learning About Behavior Analysis
Resources for Learning About Behavior AnalysisBelow is a working list of resources available to learn about behavior analysis. If you know of other helpful resources please add a sub-page to this one with the relevant information.
Resources on this website:
Provides a basic description of behavior analysis.
Provides a list of recommended books on behavior analysis, including texts that you may find useful in studying for the BCBA exam.
Provides a list of empirical RFT studies (pre-2010) with links to the articles for downloading.
There are hundreds of articles on RFT and Behavior Analysis. (Filter by topic = RFT)
This section of the website provides a variety of resources to learn more about contextualism, which is strongly linked to radical behaviorism.
ACBS Clinical Behavioral Analysis Special Interest Group
ACBS members can join the ACBS Clinical Behavioral Analysis SIG and the SIG email listserv. The SIG has resources webpage that contains a list of books, articles, and other resources.
Other Websites:
The Cambridge Center for Behavioral Studies.
You can find a lot about behavior analysis at the Cambridge Center for Behavioral Studies, which is the oldest, best established, and best known publicly focused foundation in behavioral psychology.
Association for Behavior Analysis International (ABAI).
This is the main website for ABA.
Functional Analysis
Functional AnalysisRFT Email Listserv
RFT Email ListservThe RFT email listserv is a forum for scientists, scholars, practitioners, and students to discuss Relational Frame Theory (RFT), an explicitly psychological account of human language and cognition. RFT is an approach designed to be a pragmatically useful analysis of complex human behavior, providing empirical and conceptual tools to conduct an experimental analysis of substantive topics in this arena. It is based on the principles of behavior analysis and contextual behavioral science. RFT is looked to as the conceptual basis for Acceptance and Commitment Therapy, as well as an increasingly large array of other applied interventions such as language training program, or programs designed to develop a sense of self in developmentally delayed children.
The RFT listserv is restricted to professionals or graduate students in relevant fields. Paid ACBS membership (student or professional) is required to join the RFT Listserv and you must be logged into your ACBS account.
RFT
RFTSo you want to learn more about Relational Frame Theory….welcome! We imagine that you may have landed on this page because you are interested in understanding RFT as the underpinning of ACT, you are interested in potentially doing research on RFT or with an RFT lens, you are a student and learning more about RFT, you are a professor looking for resources for your students, or simply because you are just interested in language and cognition! Whatever your reason, on these pages you will find summaries of important RFT concepts, as well as suggested resources for more in-depth learning and professional development. You will also find important and helpful information on Contextual Behavior Science, the research paradigm underlying the development of ACT and RFT, in the CBS pages on this website.
Another way to learn more about RFT is to join the RFT SIG—there is a very active listserv, and we regularly hold community discussion events.
Read more about RFT and how you might apply an understanding of RFT to your work in various arenas in the pages listed below. We (the RFT SIG) are currently in process of adding to and updating these pages and the menu bar to the left, so some pages listed may not yet be created and linked—please keep checking back. If you get lost, just come back to this main page to find this table of contents:
- RFT Basics: What is RFT?
- Relating as an operant
- Non-arbitrary vs arbitrarily-applicable relational responding
- Defining properties of relational frames
- Patterns of relational framing
- Rule-governed behavior
- Selfing
- Metaphor and analogy
- Development of relational framing
- The HDML: a model of developmental complexity and dimensions of relational framing
- Glossary
- How to Apply RFT (coming soon)
- Why RFT?
- Resources for learning about RFT
- RFT Research
- RFT SIG
- RFT FAQs
About RFT
About RFTThis is where you can read about the basic principles in Relational Frame Theory and learn about its advantages over other theories of language and cognition.
Advantages of RFT
For suggestions on further reading, please visit Resources for Learning RFT. To learn more about RFT research and application, please visit the RFT Research section.
What is RFT?
What is RFT?There is a strong empirical and conceptual relationship between language and derived stimulus relations. An empirical relationship does not indicate that derived stimulus relations depend upon language or that such relations are mediated by language. When two dependent variables are correlated, one conservative strategy is to determine whether both variables are reflective of the same basic underlying psychological process. If the two areas do overlap at the level of behavioral process, then questions about human language may also be questions about derived stimulus relations, and vice versa.
This is the basic theoretical and empirical research strategy of RFT. The overarching aim of this behavioral research has been to integrate a range of apparently diverse psychological phenomena including, for example, stimulus equivalence, naming, understanding, analogy, metaphor, and rule-following.
Relational Frame Theory adopts the view that the core defining element in all of these, and many other inherently verbal activities, is arbitrarily applicable relational responding, and moreover that such responding is amenable to a learning or operant analysis.
RFT treats relational responding as a generalized operant, and thus appeals to a history of multiple-exemplar training. Specific types of relational responding, termed relational frames, are defined in terms of the three properties of mutual and combinatorial entailment, and the transformation of functions. Relational frames are arbitrarily applicable, but are typically not necessarily arbitrarily applied in the natural language context.
Mutual entailment refers to the derived bidirectionality of some stimulus relations, and as such it is a generic term for the concept of "symmetry" in stimulus equivalence. "Mutual entailment" applies if stimulus A is related to another stimulus B in a specific context, and as a result a relation between B and A is entailed in that context. Combinatorial entailment refers to instances in which two or more relations that have acquired the property of mutual entailment mutually combine. Combinatorial entailment is the generic term for what is called "transitivity" and "equivalence" in stimulus equivalence. Combinatorial entailment applies when, in a given context, A is related to B and B is related to C, and then in that context a relation is entailed between A and C and another between C and A. For example, if A is bigger than B, and B is bigger than C, then a bigger-than relation is entailed between A and C, and a smaller-than relation is entailed between C and A. A transformation of stimulus functions applies when functions of one event in a relational network is altered based on the functions of another event in the network and the derived relation between them. Mutual and combinatorial entailment are regulated by contextual cues (C rel). The transformation of stimulus functions are regulated by additional contextual cues (C func).
The development of relational responding can be organized into a rough list that gradually becomes more and more complex. We are not presenting this list as a set of stages or steps, and we would expect them to be sequenced only in broad terms and even then only if the training history is typical. Nevertheless, this list gives a sense of the complexity that emerges from the small set of core concepts in Relational Frame Theory.
- Contextually controlled mutual entailment in equivalence
- Contextually controlled combinatorial entailment in equivalence
- Contextually controlled transfer of stimulus functions through equivalence relations
- Integration of these response components into a functional response class: a frame of coordination
- Simple examples of verbal understanding
- Contextually controlled mutual entailment in additional types of stimulus relations
- Contextually controlled combinatorial entailment in additional types of stimulus relations
- Contextually controlled transformation of stimulus functions in additional types of stimulus relations
- Integration of these into additional relational frames
- Simple examples of genuinely verbal governance of behavior by others
- Conditional contextual control over the participation of given elements in relational frames
- The development of relational networks
- More complex examples of verbal understanding
- Verbal governance of the behavior of others (e.g., verbal mands and tacts)
- Transformation of stimulus functions across relational networks
- Increasing number and complexity of relational frames
- Increasing acquisition of specific participants in specific relational frames (e.g., vocabulary)
- Complex interactions between relations (training in one influences development of another)
- Integration of related types of relational frames into families of relational responses
- Elaborated and increasingly subtle contextual control over relational responding (e.g., syntax; number of relational terms)
- Elaborated and increasingly subtle contextual control over transformation of stimulus functions (e.g., number and specificity of functional terms)
- Nonarbitrary properties serve as a relational context for arbitrarily applicable relational responses
- Increasingly complex relational networks
- With acquisition of equivalence, time or causality, and evaluation, the development of relational sentences that function fully as rules
- Relating relational networks
- Transformation of stimulus functions based on the relating of relational networks
- Relating relational networks under the control of nonarbitrary properties of the environment
- More complex examples of rule understanding and rule-governance, particularly pliance and tracking
- Regulation of the behavior of the listener through the establishment of relational networks in the listener
- With the acquisition of hierarchical class membership, use of relational networks to abstract nonarbitrary properties and to have these properties participate in relational frames
- Abstracting properties of the nonarbitrary environment based on relational networks and the relating of relational networks
- With the acquisition of temporal, contingency, and causal relational frames, increased insensitivity to temporal delays
- Development of deictic relational frames
- Development of perspective-taking and sense of self
- Construction of the verbal other
- Construction of the conceptualized group
- Contextual control of relational responding by the nonarbitrary and arbitrary properties of the listener
- Further development of rule-following, particularly augmenting
- Regulation of the behavior of the listener by orienting the listener to abstracted features of the environment
- Acquisition of increasingly abstract verbal consequences
- Self-rule generation and self rule-following
- Pragmatic verbal analysis and increasingly complex forms of problem solving and reasoning
- Increasing dominance of the verbal functions of the environment
The foregoing provides a summary of the key features of RFT. The key concept that underlies Relational Frame Theory is extremely simple—try to think of relating per se as learned behavior. As the list above shows, however, applying this simple idea leads to many specific points—the nature of an arbitrarily applicable relational response, the role of context, the varieties of relational responses, the role of the nonarbitrary environment, networks of relations, the use of these abilities to solve problems, the development of self, and so on.
Why RFT?
Why RFT?There are many different theories—in many different disciplines—that attempt to explain or account for human language and cognition. With so many different theories available, what is unique or special about Relational Frame Theory? We believe the functional, contextualistic approach of RFT to understanding complex human behavior has led to a system of analysis that offers many advantages over the traditional structural and “information transmission” models of language and cognition (Blackledge, 2003). Among these advantages are that it is parsimonious, and focuses on analyzing behavior in a way that allows for precision, scope, and depth.
Advantages of RFT
Advantages of RFTWe believe the functional, contextualistic approach of RFT to understanding complex human behavior has led to a system of analysis that offers many advantages over the traditional structural and “information transmission” models of language and cognition (Blackledge, 2003). These advantages include:
- RFT is parsimonious, relying on relatively few basic principles and concepts to account for language and cognition.
- RFT is precise, allowing the study of human language to be conducted in accordance with the carefully-specified definitions of its component processes.
- RFT has broad scope, providing plausible explanations and new empirical approaches to a wide variety of complex human behaviors in both basic and applied domains (such as problem solving, metaphors, self, spirituality, values, rule-governed behavior, psychopathology, intelligence, etc.).
- RFT has depth, meaning that its analyses cohere with established treatments at other levels of analysis. For example, it provides plausible accounts of cultural phenomena such as knowledge amplification; recent neurological research indicates that the brain processes seen while subjects engage in derived relational responding fit with the RFT language claim; and connectionist models of the learning history needed to establish relational frames coheres with RFT.
- The principles of RFT are directly observable, especially under laboratory conditions, so no tenuous inferences about the existence of unseen structures or processes (such as cognitive schemas or language acquisition devices) are required.
- RFT is firmly based on empirical research that has without exception supported its tenets. In addition to the over 30 published empirical treatments of RFT, the theory also accounts for the data observed in hundreds of empirical studies on the concept of stimulus equivalence that have been published since 1971. RFT has withstood all empirical tests so far, and all of its core claims now have at least some supportive data. So far, no data has arisen in contradiction to the theory.
- RFT has direct applied and clinical applications that are not apparent in other accounts of human language and cognition. There are many successful empirical studies on applied methods based on RFT (particularly Acceptance and Commitment Therapy, but including other methods as well, such as methods of attitude change, or the treatment of stigma and prejudice, or increasing intelligence) and many clear applied implications yet to be pursued.
- RFT is generative. The account leads quickly to innovative and (so far) empirically successful approaches to virtually all of the important topics in the language and cognition domain.
- RFT is testable. Its core claim (that relating can be thought of as learned, operant behavior) is an empirical matter. If relational frames do not develop, come under contextual control, respond to shaping via multiple exemplar training, and respond to consequences, then the theory is false. Further, its claim that relational frames are the core of human language is testable both directly and pragmatically. For example, if RFT does not lead to more successful education interventions than those that currently exist, then it fails. (see section on research evidence).
- RFT is progressive. RFT supports what is within the "protective belt" of the behavioral paradigm and yet is generative in the sense described above (see Lakatos for this approach to progressivity). RFT is a behavioral theory that builds on everything that is known about basic behavioral principles, but takes this basic account into a fundamentally new direction with profound and exciting implications for almost every topic relating to complex human behavior. Yet it does so without any patchwork corrections to the basic assumptions of the behavioral paradigm. This has resulted in newer models that are being updated as well as changes in methodology to study topics of interest more precisely.
- RFT is coherent. Its philosophical basis is well articulated; its assumptions are clearly stated; its concepts are carefully defined; and all of these levels fit together.
Applications of RFT
Applications of RFTRFT has direct applied and clinical applications that are not necessarily apparent in other accounts of human language and cognition. Many of these applications fall within the broad realm of ACT, but RFT has also been applied to early childhood language intervention programs, the study of implicit bias, academic skills, and more.
Check back soon for updates to this page.
Free Videos: Learning About and Applying RFT
Free Videos: Learning About and Applying RFTAll ACBS members have access to a wide range of recordings of conference presentations and ACBS SIG sponsored events, many of which are relevant to RFT, in the video library; a subset of these is in this collection of RFT-specific conference videos. For the past several years, the RFT SIG has held a number of recorded webinar series exploring RFT articles and conceptual topics, which are available to all members:
Dissemination and Implementation of RFT in Behavior Analysis
Top 10 Research Articles Reading Group
In the child pages below, you will find additional free videos that can help you learn about RFT. These videos were not created for or by ACBS. We merely gathered the videos from various sources for your convenience. (There are additional RFT-relevant videos available to ACBS members).
If you are an ACBS member and have additional video resources of your own to add, please go ahead and add a child page here!
If you find others on Youtube or elsewhere, please let us know by Adding a Comment and include the URL for the video and we will add it.
Relational Frame Theory (RFT) - Your ACT Auntie Series
Relational Frame Theory (RFT) - Your ACT Auntie SeriesHere is a video on RFT from the Your ACT Auntie Series
Relational Frame Theory (RFT) Crash Course
Relational Frame Theory (RFT) Crash CourseJoseph Rhinewine offers a free, 1-hour, YouTube video "crash course" on RFT.
https://www.youtube.com/playlist?list=PLdc2ztLPj9fL1GkcNaAkWePKNAC8xulms
Relational Frame Theory: From Basic Science to Behavioral/Clinical application
Relational Frame Theory: From Basic Science to Behavioral/Clinical applicationRelational Frame Theory: From Basic Science to Behavioral/Clinical Application
In this presentation, Thomas G. Szabo, Ph.D., BCBA:
• Introduces basic RFT terminology
• Reviews applied RFT findings in the literature
• Suggests essential strategies for using RFT to promote
o Perspective-taking
o Relational responding
o Creativity
RFT Basics: What is RFT?
RFT Basics: What is RFT?What is RFT?
Relational Frame Theory (RFT) is an explicitly behavior analytic account of human language and cognition. It is an approach designed to be a pragmatically useful analysis of complex human behavior, and provides the empirical and conceptual tools to conduct an experimental analysis of virtually every substantive topic in this arena. Further, the contextual approach of RFT provides a functional account of the structure of verbal knowledge and cognition, creating an important link between the traditionally disparate perspectives of cognitive and behavioral psychology.
Relational Frame Theory, as a behavior analytic theory of language and cognition, adopts the view that the core defining element in verbal activities is arbitrarily applicable relational responding, and moreover that such responding is amenable to a learning or operant analysis.
RFT involves and addresses a number of theoretical concepts:
- Relating as an operant
- Non-arbitrary vs arbitrarily-applicable relational responding
- Defining properties of relational frames
- Patterns of relational framing
- Rule-governed behavior
- Selfing
- Metaphor and analogy
- Development of relational framing
- The HDML: a model of developmental complexity and dimensions of relational framing (coming soon)
- Glossary
Defining properties of relational frames
Defining properties of relational framesSpecific types of relational responding, termed relational frames, are defined in terms of the three properties of mutual and combinatorial entailment, and the transformation of functions. Relational frames are arbitrarily applicable, but are typically not necessarily arbitrarily applied in the natural language context.
Mutual entailment refers to the derived bidirectionality of some stimulus relations, and as such it is a generic term for the concept of "symmetry" in stimulus equivalence. "Mutual entailment" applies if stimulus A is related to another stimulus B in a specific context, and as a result a relation between B and A is entailed in that context.
Combinatorial entailment refers to instances in which two or more relations that have acquired the property of mutual entailment mutually combine. Combinatorial entailment is the generic term for what is called "transitivity" and "equivalence" in stimulus equivalence. Combinatorial entailment applies when, in a given context, A is related to B and B is related to C, and then in that context a relation is entailed between A and C and another between C and A. For example, if A is bigger than B, and B is bigger than C, then a bigger-than relation is entailed between A and C, and a smaller-than relation is entailed between C and A.
A transformation of stimulus functions applies when functions of one event in a relational network is altered based on the functions of another event in the network and the derived relation between them. Mutual and combinatorial entailment are regulated by contextual cues (C rel). The transformation of stimulus functions are regulated by additional contextual cues (C func).
Development of relational framing
Development of relational framingThe development of relational responding can be organized into a rough list that gradually becomes more and more complex. We are not presenting this list as a set of stages or steps, and we would expect them to be sequenced only in broad terms and even then only if the training history is typical. Nevertheless, this list gives a sense of the complexity that emerges from the small set of core concepts in Relational Frame Theory.
- Contextually controlled mutual entailment in equivalence
- Contextually controlled combinatorial entailment in equivalence
- Contextually controlled transfer of stimulus functions through equivalence relations
- Integration of these response components into a functional response class: a frame of coordination
- Simple examples of verbal understanding
- Contextually controlled mutual entailment in additional types of stimulus relations
- Contextually controlled combinatorial entailment in additional types of stimulus relations
- Contextually controlled transformation of stimulus functions in additional types of stimulus relations
- Integration of these into additional relational frames
- Simple examples of genuinely verbal governance of behavior by others
- Conditional contextual control over the participation of given elements in relational frames
- The development of relational networks
- More complex examples of verbal understanding
- Verbal governance of the behavior of others (e.g., verbal mands and tacts)
- Transformation of stimulus functions across relational networks
- Increasing number and complexity of relational frames
- Increasing acquisition of specific participants in specific relational frames (e.g., vocabulary)
- Complex interactions between relations (training in one influences development of another)
- Integration of related types of relational frames into families of relational responses
- Elaborated and increasingly subtle contextual control over relational responding (e.g., syntax; number of relational terms)
- Elaborated and increasingly subtle contextual control over transformation of stimulus functions (e.g., number and specificity of functional terms)
- Nonarbitrary properties serve as a relational context for arbitrarily applicable relational responses
- Increasingly complex relational networks
- With acquisition of equivalence, time or causality, and evaluation, the development of relational sentences that function fully as rules
- Relating relational networks
- Transformation of stimulus functions based on the relating of relational networks
- Relating relational networks under the control of nonarbitrary properties of the environment
- More complex examples of rule understanding and rule-governance, particularly pliance and tracking
- Regulation of the behavior of the listener through the establishment of relational networks in the listener
- With the acquisition of hierarchical class membership, use of relational networks to abstract nonarbitrary properties and to have these properties participate in relational frames
- Abstracting properties of the nonarbitrary environment based on relational networks and the relating of relational networks
- With the acquisition of temporal, contingency, and causal relational frames, increased insensitivity to temporal delays
- Development of deictic relational frames
- Development of perspective-taking and sense of self
- Construction of the verbal other
- Construction of the conceptualized group
- Contextual control of relational responding by the nonarbitrary and arbitrary properties of the listener
- Further development of rule-following, particularly augmenting
- Regulation of the behavior of the listener by orienting the listener to abstracted features of the environment
- Acquisition of increasingly abstract verbal consequences
- Self-rule generation and self rule-following
- Pragmatic verbal analysis and increasingly complex forms of problem solving and reasoning
- Increasing dominance of the verbal functions of the environment
Relating as an operant
Relating as an operantRelational responding involves generalized responding in accordance with a pattern of relations between stimuli, rather than responding to a stimulus on the basis of one or a limited number of associations. RFT proposes that relational framing, or relating, is generalized operant behavior.
Like all operants, relational framing is influenced by and can only be understood within its current and historical context. Relational framing also demonstrates the primary characteristics of all operant behavior:
- Acquisition and strengthening over time through a history of reinforcement/multiple exemplar training
- Flexibility/changes in response to changes in the environment
- Influence by antecedent stimulus control
- Influence by consequential stimulus control
Like any other operant, relational framing is a skill that can be fragile (e.g., less widely generalized, with a slow rate of responding) or stronger (e.g. more widely generalized, fluent). Thus, practice in relational framing would be expected to strengthen the operant and result in more fluent responding in any context in which deriving relations is relevant—that is, almost any language-based task. Research on relational training has suggested that not only can multiple exemplar training result in the acquisition of framing repertoires if not already present, but that strengthening existing relational repertoires can result in significant increases in standardized cognitive and academic measures across a range of populations. Such work supports the core RFT thesis that relational framing as an operant is central to human language in all its potential generativity and complexity.
For further reading on relating as an operant, see:
Hayes, S. C., Law, S., Assemi, K., Falletta-Cowden, N., Shamblin, M., Burleigh, K., Olla, R., Forman, M., & Smith, P. (2021). Relating is an Operant: A Fly Over of 35 Years of RFT Research. Perspectivas em Análise do Comportamento. https://doi.org/10.18761/pac.2021.v12.rft.02
Hughes, S., & Barnes‐Holmes, D. (2015). Relational Frame Theory: The Basic Account. In R. D. Zettle, S. C. Hayes, D. Barnes-Holmes, & A. Biglan (Eds.), The Wiley handbook of contextual behavioral science (pp. 129-178). John Wiley & Sons.
RFT FAQ
RFT FAQThis section provides frequently asked questions and answers about RFT and its applications. This section is being updated and added to by the RFT SIG, please keep checking back!
ACBS Members: To provide a question and an answer to this FAQ, click on the "add child page" link at the bottom of this page and contribute a page to the website. If you have a question but do not have an answer, please "add a new comment" and we will endeavor to find an answer for you!
How does Relational Frame Theory (RFT) relate to traditional CBT-theories?
How does Relational Frame Theory (RFT) relate to traditional CBT-theories?That question is a huge one. RFT seeks a broad understanding of cognition. In the long run it could be more important than ACT because if it works the whole of psychology could change.
RFT is developmental, contextual, and behavioral. It gives you ideas about what to change to make things happen. It is so basic that it goes all the way down to animal behavior and human infants; and yet so broad in scope that it has clear implications for our understanding of social processes or such human activities as religion.
We have never had an empirically adequate behavioral, contextual account of cognition. Now we have at least the beginnings of one and it seems to be braking down the artificial barriers between cognitive and behavioral science.
The theories underlying CBT and CT are not like that. They have relatively low scope and they emerged typically from clinical concerns. They do not pretend to be the functional equivalent in cognition for what “behavioral principles” are in non-verbal behavior.
You have to be impressed with what the traditional behavior therapists were able to do with traditional behavioral principles, in part because these principles emphasized manipulable contextual variables. Imagine what we might do with a theory of cognition that emphasized manipulable contextual variables, if the theory was relatively adequate. Maybe a lot.
How is RFT different from stimulus equivalence?
How is RFT different from stimulus equivalence?I often hear behavior analysts comment that RFT is essentially the same thing as stimulus equivalence, or that RFT does not add anything new to the equivalence literature.
Here are a few points to help clarify the difference between RFT and stimulus equivalence:
1) Stimulus equivalence is an empirical phenomenon; RFT is a behavioral theory about how that phenomenon (and other phenomena) comes about. In other words, RFT provides an operant analysis of how/why people are able to form equivalence classes. I cringe when I hear behavior analysts try to use stimulus equivalence as an explanation for some other behavioral event without recognizing that equivalence itself is a behavioral event that requires a technical analysis! This is especially true because the phenomenon of equivalence doesn't readily make sense from a direct contingency analysis (i.e., the "derived" or "emergent" relations are interesting because they're somewhat unexpected based on the organism's history of reinforcement in the presence of the "equivalent" stimuli...that is why we call the relations "derived" or "emergent").
2) Murray Sidman, a pioneer in behavior analysis and stimulus equivalence research, provided some of the earliest behavioral accounts of stimulus equivalence. Sidman's approach, however, was/is primarily a descriptive one: "My own theorizing has been directed not so much at an explanation of equivalence relations but rather, at the formulation of a descriptive system -- a consistent, coherent, and parsimonious way of defining and talking about the observed phenomena" (Sidman, 1994). A precise, coherent description of an empirical phenomenon is important, but it is not the same as a functional, behavioral explanation. RFT attempts to offer such an explanation.
3) In my view, RFT is a more scientifically conservative way to account for equivalence (as compared to Sidman's approach) because it does not require any new behavioral principles at the level of process (in Chapter 2 of the RFT book, we do propose a new behavioral principle at the level of outcome, but that is simply due to the unusual effects we see from the transformation of stimulus functions). Sidman, on the other hand, suggests that equivalence is probably a basic stimulus function "not derivable from more fundamental processes." RFT claims that it IS derivable from more fundamental processes -- basically, a history of multiple-exemplar training and differential reinforcement for relational responding.
4) The terms RFT uses to describe equivalence and other derived stimulus relations (e.g., mutual entailment, combinatorial entailment, transformation of stimulus functions) are more general than the terms used by Sidman (e.g., reflexivity, symmetry, transitivity, etc.). RFT introduced these new terms so that we could have a language to talk about all different types of stimulus relations (bigger than, before-after, opposites, darker than, etc.). Sidman's terms were taken from mathematical set theory and apply to equivalence relations, but do not work for other types of stimulus relations. In other words, RFT folks did not create new terms just for the hell of it or just because they sounded kewl.
5) RFT, as suggested in point 4, also emphasizes research on types of derived stimulus relations other than equivalence. This is important because stimulus functions can be changed on the basis of these derived relations, and the functions will be changed differently based on different relations. It has been demonstrated many times now that stimulus functions can transfer between members of an equivalence class (i.e., if one stimulus becomes a conditioned reinforcer, other stimuli in the equivalence class may also become reinforcers). But it has also been demonstrated that a stimulus can acquire new functions on the basis of a derived relation other than equivalence to another stimulus. For example, if stimulus A is a conditioned reinforcer and the learner derives a relation of opposition between stimulus A and B, stimulus B is likely to acquire aversive functions (the stimulus functions are transformed on the basis of its derived relation to stimulus A). This has been demonstrated with quite a few different types of stimulus functions and with quite a few different types of relations. Many researchers studying derived relations focus on equivalence relations exclusively, but RFT suggests knowledge of these other types of relations and their impact on the psychological functions of stimuli is also vitally important to a comprehensive theory of language and cognition.
Research: Basic & Applied
Research: Basic & AppliedThe core of the contextual behavioral science (CBS) model of science is work that is inherently translational in nature; basic research informing interventions and vice versa.
Therefore RFT researchers are comprised of basic scientists who possess an interest in RFT’s application to human behavior, or are also clinicians or applied behavior analysts who are interested in understanding clinically-relevant phenomena. As such, RFT principles and processes have been useful for influencing and optimizing performance and functioning across a broad range of human phenomena.
In the Publications section of this website, you will find articles and books about RFT.
JCBS had a Special Issue on Conceptual Developments in Relational Frame Theory: Research and Practice; Guest Edited by Dermot Barnes-Holmes, Yvonne Barnes-Holmes, Ian Stewart and Thomas Parling
Also, the ACBS community has has a list of research labs all over the world where you might:
- gain a better understanding of the current lines of research in RFT that is ongoing;
- network with others doing similar work as yours;
- foster collaboration between researchers and labs;
- follow up with researchers on the status of projects.
Please click here to find a comprehensive list of RFT laboratories.
Empirical Support
Empirical SupportThis list includes research articles that contain original data relevant to RFT up until 2010. As the number of RFT articles has increased greatly since then, updating this list has become challenging.
For the most up-to-date list, visit the publications database and choose "RFT: Empirical" as a search term. To search for RFT articles by year type in "RFT 2011" or "Relational 2011" on the publications database search.
When logged in, ACBS members can add child pages to update this with new literature -- learn how here.
As of the beginning of 2009, there are about 150 empirical articles that are either on RFT ideas, or very closely related.
2011 - 2021
Hayes, S. C., Law, S., Assemi, K., Falletta-Cowden, N., Shamblin, M., Burleigh, K., Olla, R., Forman, M., & Smith, P. (2021). Relating is an Operant: A Fly Over of 35 Years of RFT Research. Perspectivas Em Análise Do Comportamento, 12(1). DOI: 10.18761/PAC.2021.v12.RFT.02
RFT was first formally described in 1985 and in the 35 years since, hundreds of studies have been conducted on relational learning from an operant point of view. This paper briefly summarizes that history and examines some of its key claims. So far, the empirical program delineated by RFT has held up remarkably well.
O'Connor, M, Farrell, L, Munnelly, A., and McHugh, L. (2017). Citation analysis of relational frame theory: 2009–2016. Journal of Contextual Behavioral Science, Volume 6, Issue 2, Pages 152-158.
This article contains a list of Empirical RFT articles in the Supplementary material for Empirical RFT articles
2010
Barnes-Holmes, D., Murphy, A., Barnes-Holmes, Y., & Stewart, I., (2010). The Implicit Relational Assessment Procedure: Exploring the impact of private versus public contexts and the response latency criterion on pro-white and anti-black stereotyping among white Irish individuals. The Psychological Record, 60, 57-80.
Barnes-Holmes, D., Murtagh, L., Barnes-Holmes, Y., & Stewart, I. (2010). Using the Implicit Association Test and the Implicit Relational Assessment Procedure to measure attitudes towards meat and vegetables in vegetarians and meat-eaters. The Psychological Record.
One of the first two empirical studies to test the validity of the IRAP by comparing it to the IAT using a "known-groups" approach. The studies also introduce the use of the D-IRAP algorithm.
Cassidy, S., Roche, B., & O’Hora, D. (2010). Relational Frame Theory and human intelligence. European Journal of Behavior Analysis, 11(1), 37-51.
An early conceptual look at the relationship between derived relational responding and intelligence.
Dymond, S., May, R. J., Munnelly, A., & Hoon, A. E. (2010). Evaluating the evidence based for relational frame theory: A citation analysis. The Behavior Analyst, 33, 97-117.
A total of 174 articls were identified between 1991 and 2008, 62 (36%) of which were empirical and 112 (64%) were nonempirical articles. Further analyses on these articles are conducted.
Dymond, S., & Roche, B. (2010). The impact of derived relational responding on gambling behavior. Analysis of Gambling Behavior, 4, 1-16.
Gore, N. J., Barnes-Holmes, Y., & Murphy, G. (2010). The relationship between intellectual functioning and relational perspective-taking. International Journal of Psychology and Psychological Therapy, 10(1), 1-17.
Guinther, P. M., & Dougher, M. J. (2010). Semantic False Memories In The Form Of Derived Relational Intrusions Following Training. Journal of the Experimental Analysis of Behavior, 93(3), 329.
Hinton, E. C., Dymond, S, Von Hecker, U. & Evans, C. J. (2010). Neural correlates of relational reasoning and the symbolic distance effect: Involvement of parietal cortex. Neuroscience, 168, 138-148.
Hooper, N., Saunders, S., & McHugh, L. (2010). The derived generalization of thought suppression. Learning and Behavior.
Levin, M. E., Hayes, S. C., & Waltz, T. (2010). Creating an implicit measure of cognition more suited to applied research: A test of the Mixed Trial - Implicit Relational Assessment Procedure (MT-IRAP). International Journal of Behavioral Consultation and Therapy, 6, 245-261.
Moran, L., Stewart, I., McElwee, J., & Ming, S. (2010). Brief Report: The Training and Assessment of Relational Precursors and Abilities (TARPA): A Preliminary Analysis. Journal of Autism and Developmental Disorders.
Munnelly, A., Dymond, S., & Hinton, E. C. (2010). Relational reasoning with derived comparative relations: A novel model of transitive inference. Behavioral Processes, 85, 8-17.
Vahey, N., Boles, S., & Barnes-Holmes, D. (2010). Measuring Adolescents' Smoking-related Social Identity Preferences with the Implicit Relational Assessment Procedure (IRAP) for the First Time: A Starting Point that Explains Later IRAP Evolutions. International Journal of Psychology and Psychological Therapy, 10, 453-474.
Villatte, M., Monestès, J. L., McHugh, L., Freixa i Baqué, E., & Loas, G. (2010). Adopting the perspective of another in belief attribution: Contribution of Relational Frame Theory to the understanding of impairments in schizophrenia. Journal of Behavior Therapy and Experimental Psychiatry, 41, 125-134.
Villatte, M., Monestès, J. L., McHugh, L., Freixa i Baqué, E., & Loas, G. (2010). Assessing perspective taking in schizophrenia using Relational Frame Theory. The Psychological Record, 60, 413-424.
2009
Barnes-Holmes, D., Waldron, D., Barnes-Holmes, Y., & Stewart, I. (2009). Testing the validity of the Implicit Relational Assessment Procedure (IRAP) and the Implicit Association Test (IAT): Measuring attitudes towards Dublin and country life in Ireland. The Psychological Record, 59, 389-406.
One of the first two empirical studies to test the validity of the IRAP by comparing it to the IAT using a "known-groups" approach. The studies also introduce the use of the D-IRAP algorithm.
Dawson, D. L., Barnes-Holmes, D., Gresswell, D. M., Hart, A. J. P., & Gore, N. J. (2009). Assessing the implicit beliefs of sexual offenders using the Implicit Relational Assessment Procedure: A First Study. Sexual Abuse: A Journal of Research and Treatment, 21, 57-75.
Power, P. M., Barnes-Holmes, D., Barnes-Holmes, Y., & Stewart, I. (2009). The Implicit Relational Assessment Procedure (IRAP) as a measure of implicit relative preferences: A first study. The Psychological Record, 59, 621-640.
The first IRAP study that involved using comparative relations as a means of determining implicit relative preferences for different social groups. This was also the first study to show a clear divergence between responses on the IRAP and an explicit measure.
Gross, A. C., & Fox, E. J. (2009). Relational frame theory: An overview of the controversy. The Analysis of Verbal Behavior, 25, 87-98.
Vahey, N. A., Barnes-Holmes, D., Barnes-Holmes, Y., & Stewart, I. (2009). A first test of the Implicit Relational Assessment Procedure (IRAP) as a measure of self-esteem: Irish prisoner groups and university students. The Psychological Record, 59, 371-388.
The first empirical study that aimed to develop a self-esteem IRAP.
Lipkens, G. & Hayes, S. C. (2009). Producing and recognizing analogical relations. Journal of the Experimental Analysis of Behavior, 91, 105-126.
Article shows for the first time that relating relations can be the basis of producing related events, selecting relations, or selecting related events.
Murphy, C. & Barnes-Holmes, D. (2009). Establishing derived manding for specific amounts with three children: An attempt at synthesizing Skinner's verbal behavior and relational frame theory. Psychological Record, 59(1), 75-91.
O'Connor, J., Rafferty, A., Barnes-Holmes, D. & Barnes-Holmes, Y. (2009). The role of verbal behavior, stimulus nameability and familiarity on the equivalence performances of autistic and normally developing children.Psychological Record, 59(10), 53-74.
O'Toole, C., & Barnes-Holmes, D. (2009). Three chronometric indices of relational responding as predictors of performance on a brief intelligence test: The importance of relational flexibility. The Psychological Record, 59(1), 119-132.
The first empirical study that used the IRAP to investigate the relationship between relational responding and IQ. Although not reported in the article, the research allowed us to determine that the D-IRAP algorithm appears to control for individual differences in cognitive ability.
2008
Barnes-Holmes, D., Hayden, E., Barnes-Holmes, Y., & Stewart, I. (2008). The Implicit Relational Assessment Procedure (IRAP) as a response-time and event-related-potentials methodology for testing natural verbal relations: A preliminary study. The Psychological Record, 58, 497-516.
The first empirical study of the IRAP. The article also provides a brief potted history of the research that led to the development of the procedure.
Dymond, S., Roche, B., Forsyth, J.P., Whelan, R. & Rhoden, J. (2008). Derived avoidance learning: Transformation of avoidance response functions in accordance with same and opposite relational frames. The Psychological Record, 58, 269-286.
This interesting study demonstrated that participants will demonstrate avoidance based on the stimulus relations of “same” and “opposite.” Control participants provided evidence that the transformation was a direct product of a relational learning history. Although equivalence may account for the finding, the explanation is circuitous.
Gavin, A., Roche, B., & Ruiz, M. R. (2008). Competing contingencies over derived relational responding: A behavioral model of the implicit association test. The Psychological Record, 58, 427-441.
Ju, W. C. & Hayes, S. C. (2008). Verbal establishing stimuli: Testing the motivative effect of stimuli in a derived relation with consequences. The Psychological Record, 58, 339-363.
McHugh, L., & Reed, P. (2008). Using Relational Frame Theory to build grammar in children with Autistic Spectrum Conditions. The Journal of Speech-Language Pathology and Applied Behavior Analysis, 2.4-3.1, 60-77.
O'Hora, D., Pelaez, M., Barnes-Holmes, D., Rae, G., Robinson, K., & Chaudhary, T. (2008). Temporal relations and intelligence: Correlating relational performance with performance on the WAIS-III. The Psychological Record, 58, 569-584.
Pérez-González, L.A., Herszlikowicz, K. & Williams, G. (2008). Stimulus relations analysis and the emergence of novel intraverbals. Psychological Record, 58, 95-129.
Roche, B. T., Kanter, J. W., Brown, K. R., Dymond, S., & Fogarty, C. C. (2008). A comparison of "direct" versus "derived" extinction of avoidance responding. The Psychological Record, 58, 443-464.
Roche, B. & Dymond, S. (2008). A transformation of functions in accordance with the nonarbitrary relational properties of sexual stimuli. Psychological Record, 58, 71-94.
Vitale, A., Barnes-Holmes, Y., Barnes-Holmes, D., & Campbell, C. (2008). Facilitating responding in accordance with the relational frame of comparison: Systematic empirical analyses. The Psychological Record, 58, 365-390.
Weinstein, J. H., Wilson, K. G., Drake, C. E., & Kellum, K. K. (2008). A Relational Frame Theory Contribution to Social Categorization. Behavior and Social Issues, 17, 39-64.
2007
Berens, N. M., & Hayes, S. C. (2007). Arbitrarily applicable comparative relations: Experimental Evidence for relational operants. Journal of Applied Behavior Analysis, 40, 45-71.
In a combined multiple baseline (across responses and participants) and multiple probe design (with trained and untrained stimuli), it was shown that reinforced multiple exemplar training facilitated the development of arbitrary comparative relations, and that these skills generalized not just across stimuli but also across trial types.
Cahill, J., Barnes-Holmes, Y., Barnes-Holmes, D., Rodríguez-Valverde, M., Luciano, C., & Smeets, P. M. (2007). The derived transfer and reversal of mood functions through equivalence relations II. The Psychological Record, 57, 373-389.
Dougher, M. J., Hamilton, D., Fink, B., & Harrington, J. (2007). Transformation of the discriminative and eliciting functions of generalized relational stimuli. Journal of the Experimental Analysis of Behavior, 88(2), 179-197.
Transformation of respondent stimulus functions via more-than/less-than direct and derived relations.
Gómez, S., López, F., Martín, C.B., Barnes-Holmes, Y. & Barnes-Holmes, D. (2007). Exemplar training and a derived transformation of functions in accordance with symmetry and equivalence. Psychological Record, 57(2), 273-294.
This is a very straightforward study programming transformation of function with young children. The first experiment simply exposed four children to action-object exemplar training and tested for symmetry. Experiment two enhanced transformation via multiple exemplar training; effectively demonstrating the ability to program stimulus relations via exemplar training.
Gaynor, S. T., Washio, Y. & Anderson, F. (2007). The conjunction fallacy: A derived stimulus relations conceptualization and demonstration experiment. The Psychological Record, 57, 63-85.
Luciano, M. C., Gómez, I., & Rodríguez, M. (2007). The Role of Multiple-Exemplar Training and Naming in Establishing Derived Equivalence in an Infant. Journal of Experimental Analysis of Behavior.
McHugh, L., Barnes-Holmes, Y. & Barnes-Holmes, D. (2007). Deictic relational complexity and the development of deception. Psychological Record, 57(4), 517-531.
McHugh, L., Barnes-Holmes, Y., Barnes-Holmes, D., Whelan, R. & Stewart, I. (2007). Knowing me, knowing you: Deictic complexity in false-belief understanding. Psychological Record, 57(4), 533-542.
McKenna, I. M., Barnes-Holmes, D., Barnes-Holmes, Y., & Stewart, I. (2007). Testing the fake-ability of the implicit relational assessment procedure (IRAP): the first study. International Journal of Psychology and Psychological Therapy, (7)2, 123-138.
The first empirical study that sought to determine if the IRAP can be readily faked.
O'Toole, C., Barnes-Holmes, D. & Smyth, S. (2007). A derived transfer of functions and the Implicit Association Test.Journal of the Experimental Analysis of Behavior, 88(2), 263-283.
Rehfeldt, R., Dillen, J. E., Ziomek, M. M. & Kowalchuk, R. K. (2007). Assessing Relational Learning Deficits in Perspective-Taking in Children with High Functioning Autism Spectrum Disorder. The Psychological Record, 57, 23-47.
Rosales, R. & Rehfeldt, R.A. (2007). Contriving transitive conditioned establishing operations to establish derived manding skills in adults with severe developmental disabilities. Journal of Applied Behavior Analysis, 40(1), 105-121.
Schlund, M.W., Hoehn-Saric, R. & Cataldo, M.F. (2007). New knowledge derived from learned knowledge: Functional-anatomic correlates of stimulus equivalence. Journal of the Experimental Analysis of Behavior, 87(2), 287-307.
2006
Barnes-Holmes, D., Barnes-Holmes, Y., Power, P., Hayden, E., Milne, R., & Stewart, I. (2006). Do you really know what you believe? developing the implicit relational assessment procedure (IRAP) as a direct measure of implicit beliefs. The Irish Psychologist, (32)7, 169-177.
Dixon, M.R., Rehfeldt, R.A., Zlomke, K.R. & Robinson, A. (2006). Exploring the development and dismantling of equivalence classes involving terrorist stimuli. Psychological Record, 56, 83-103.
This paper describes 2 studies that present a conceptual interpretation and experimental findings involving developing and dismantling of equivalence classes consisting of terrorist stimuli. Results of experiment 1 showed that participants made predictable responses to stimuli during pretest, however made fewer culturally controlled responses after training. Experiment 2 showed that it was easy to acquire relations involving terrorist stimuli when compared to two other conditions. Implications are discussed.
Dixon, M. R., Zlomke, K. M., & Rehfeldt, R. A. (2006). Restoring Americans’ Nonequivalent Frames of Terror: An Application of Relational Frame Theory. The Behavior Analyst Today, 7(3), 275-289.
Haas, J. R., & Hayes, S.C. (2006). When knowing you are doing well hinders performance: Exploring the interaction between rules and feedback. Journal of Organizational Behavior Management, 26, 91-111.
The effect of two types of verbal consequences, rule-following feedback and task performance feedback, on rule-induced insensitivity to programmed schedules of reinforcement were examined. Rule-following feedback could be either accurate or non-contingently positive. The task involved moving a sign through a grid using telegraph keys operating on a multiple DRL 6/FR 18 schedule of reinforcement in the presence of an initially accurate rule. After acquisition, the multiple schedule was changed without notice to a FR 1/FI Yoked schedule. Accurate rule-following feedback plus feedback on task performance produced striking insensitivity to the DRL 6 to FR 1 schedule change, the opposite of what might be expected by a common sense analysis of task performance feedback, even after controlling for contact with the changed contingency. It is argued that findings such as these can only be understood by considering the mutual verbal relations evoked by the combinations of rules and feedback, rather than treating feedback as a simple consequential event or as a verbal consequence whose effects do not depend on the relations sustained with other events.
McHugh, L., Barnes-Holmes, Y., Barnes-Holmes, D. & Stewart, I. (2006). Understanding false belief as generalized operant behavior. Psychological Record, 56(3), 341-364.
Ninness, C., Barnes-Holmes, D., Rumph, R., McCuller, G., Ford, A. M., Payne, R., et al. (2006). Transformations of mathematical and stimulus functions. Journal of Applied Behavior Analysis, 39, 299-321.
Smeets, P. M., Barnes-Holmes, D., & Striefel, S. (2006). Establishing and reversing equivalence relations with precursor to the relational evaluation procedure. The Psychological Record, 56(2), 267-286.
Smyth, S., Barnes-Holmes, D., & Forsyth, J. P. (2006). A derived transfer of simple discrimination and self-reported arousal functions in spider fearful and non-spider fearful participants. Journal of the Experimental Analysis of Behavior, 85(2), 223-246.
This article used the stimulus paring observation procedure to demonstrate transformation of arousal functions, and provided further evidence that anxiety responses can participate in arbitrary relational frames and produce problematic clinical outcomes.
Valdivia, S., Luciano, C., & Molina, F. J. (2006). Verbal regulation of motivational states. The Psychological Record, 56, 577-595.
Whelan, R., Barnes-Holmes, D. & Dymond, S. (2006). The transformation of consequential functions in accordance with the relational frames of more-than and less-than. Journal of the Experimental Analysis of Behavior, 86(3), 317-335.
2005
Barnes-Holmes, D., Regan, D., Barnes-Holmes, Y., Commins, S., Walsh, D., Stewart, I., et al. (2005). Relating derived relations as a model of analogical reasoning: reaction times and event-related potentials. Journal of the Experimental Analysis of Behavior, 84(3), 435-451.
This study used event related potentials to test the RFT prediction that same-same relations are simpler and functionally distinct different-different analogical reasoning. Reaction times were significantly longer, and waveforms were significantly more negative for different-different than they were for same-same relations. This is consistent with the prediction based on RFT.
Dixon, M.R. & Zlomke, K.M. (2005). Implementación del precursor del procedimiento de evaluación relacional en el establecimiento de marcos relacionales de igualdad, oposición y diferencia. = Using the precursor to the relational evaluation procedure (PREP) to establish the relational frames of sameness, opposition, and distinction. Revista Latinoamericana de Psicología, 37(2), 305-316.
Gutiérrez-Martí¬nez, O., Luciano-Soriano, M. C., & Valdivia, S. (2005). Change of self-efficacy verbalizations and derivation of functions. Psicothema, 17, 625-630.
Merwin, R.M. & Wilson, Kelly G. (2005). Preliminary findings on the effects of self-referring and evaluative stimuli on stimulus equivalence class formation. Psychological Record, 55, 561-575.
Murphy, C., Barnes-Holmes, D., & Barnes-Holmes, Y. (2005). Derived manding in children with autism: Synthesizing Skinner's verbal behavior with relational frame theory. Journal of Applied Behavior Analysis, 38(4), 445-462.
Ninness, C., Rumph, R., McCuller, G., Harrison, C., Ford, A. M., & Ninness, S. K. (2005). A functional analytic approach to computer-interactive mathematics. Journal of Applied Behavior Analysis, 38 , 1-22.
One of the first uses of RFT in higher education. Here is the abstract: Following a pretest, 11 participants who were naive with regard to various algebraic and trigonometric transformations received an introductory lecture regarding the fundamentals of the rectangular coordinate system. Following the lecture, they took part in a computer-interactive matching-to-sample procedure in which they received training on particular formula-to-formula and formula-to-graph relations as these formulas pertain to reflections and vertical and horizontal shifts. In training A-B, standard formulas served as samples and factored formulas served as comparisons. In training B-C, factored formulas served as samples and graphs served as comparisons. Subsequently, the program assessed for mutually entailed B-A and C-B relations as well as combinatorially entailed C-A and A-C relations. After all participants demonstrated mutual entailment and combinatorial entailment, we employed a test of novel relations to assess 40 different and complex variations of the original training formulas and their respective graphs. Six of 10 participants who completed training demonstrated perfect or near-perfect performance in identifying novel formula-to-graph relations. Three of the 4 participants who made more than three incorrect responses during the assessment of novel relations showed some commonality among their error patterns. Derived transfer of stimulus control using mathematical relations is discussed.
Ninness, C., Rumph, R., McCuller, G., Vasquez III, E., Harrison, C., Ford, A.M., et al. (2005b). A relational frame and artificial neural network approach to computer-interactive mathematics. Psychological Record, 55, 135-153.
O'Hora, D., Â Pelaez, M., & Barnes-Holmes, D. (2005). Derived relational responding and performance on verbal subtests of the WAIS-III. The Psychological Record, 55(1), 155-175.
Rehfeldt, R.A. & Dymond, S. (2005). The effects of test order and nodal distance on the emergence and stability of derived discriminative stimulus functions. Psychological Record, 55(2), 179-196.
Rehfeldt, R. A. & Root, S. L. (2005). Establishing derived requesting skills in adults with severe developmental disabilities. Journal of Applied Behavior Analysis, 38, 101-105.
Reilly, T., Whelan, R., & Barnes-Holmes, D. (2005). The effect of training structure on the latency responses to a five-term linear chain. The Psychological Record, 55(2), 233-249.
Smeets, P.M., & Barnes-Holmes, D. (2005a). Auditory-visual and visual-visual equivalence relations in children. The Psychological Record, 55(3), 483-503.
Smeets, P. M., & Barnes-Holmes D. (2005b). Establishing equivalence classes in preschool children with many-to-one and one-to-many training protocols. Behavioural Processes, 69(3), 281-293.
Whelan, R., Cullinan, V. & O'Donovan, A. (2005). Derived same and opposite relations produce association and mediated priming. = Mismas Relaciones derivadas y Opuestas Producen la Asociación y la Preparación Mediada.International Journal of Psychology & Psychological Therapy, 5(3), 247-264.
2004
Barnes-Holmes, Y., Barnes-Holmes, D., & Smeets, P. M. (2004). Establishing relational responding in accordance with opposite as generalized operant behavior in young children. International Journal of Psychology and Psychological Therapy, 4, 559-586.
Barnes-Holmes, Y., Barnes-Holmes, D., Smeets, P. M., & Luciano, C. (2004). The derived transfer of mood functions through equivalence relations. The Psychological Record, 54, 95-114.
Barnes-Holmes, Y., Barnes-Holmes, D., Smeets, P. M., Strand, P., & Friman, P. (2004). Establishing relational responding in accordance with more-than and less-than as generalized operant behavior in young children.International Journal of Psychology and Psychological Therapy, 4, 531-558.
Barnes-Holmes, D., Staunton, C., Barnes-Holmes, Y., Whelan, R., Stewart, I., Commins, S., et al. (2004). Interfacing Relational Frame Theory with cognitive neuroscience: Semantic priming, The Implicit Association Test, and event related potentials. International Journal of Psychology and Psychological Therapy, 4, 215-240.
Carpentier, F., Smeets, P. M., & Barnes-Holmes, D. (2004). Equivalence-equivalence: Matching stimuli with same discriminative functions. The Psychological Record, 54, 145-162.
Carpentier, F., Smeets, P. M., Barnes-Holmes, D., & Stewart, I. (2004). Matching derived functionally-same relations: Equivalence-equivalence and classical analogies. The Psychological Record, 54, 255-273.
McHugh, L., Barnes-Holmes, Y., & Barnes-Holmes, D. (2004). Perspective-taking as relational responding: A developmental profile. The Psychological Record, 54, 115-144.
This article describes traditional tasks that relate to what developmental literature calls “Theory of Mind. ” Its goals were to develop and test a protocol across groups in several different developmental stages (young children through adulthood) that indicated that perspective taking could be described in terms of relational responding (arbitrarily applicable, mutually entailed, combinatorily entailed, and showing transformation of stimulus function) and that added but did not contradict the traditional and developmental literature. Study 1 tested the protocol, Study 2 tested whether young children’s poor response was an artifact of word length, and Study 3 tested whether the experimenter’s cues affected responding. Results from three studies indicated indeed that perspective taking can be viewed as an operant, and that deictic frames across three levels of complexity were functionally distinct classes of behavior. A developmental profile emerged, showing that derived relational responding develops with age as well as relational complexity. Further, I-YOU relations emerge before HERE-THERE and NOW-THEN relations, and NOW-THEN relations produced the most errors in all participants regardless of age.
O'Hora, D., Barnes-Holmes, D., Roche, B., & Smeets, P. M. (2004). Derived relational networks and control by novel instructions: A possible model of generative verbal responding. The Psychological Record, 54, 437-460.
Results from two studies examining instructional control on novel stimulus situations are described. The researchers employed the Relational Evaluation Procedure to train relations and then tested these in novel situations. Results support the idea that novel instructions can control behavior and that RFT provides an adequate model for the generativity of language.
Roche, B., Linehan, C., Ward, T., Dymond, S., & Rehfeldt, R. (2004). The Unfolding of the Relational Operant: A Real-time Analysis Using Electroencephalography and Reaction Time Measures. International Journal of Psychology & Psychological Therapy, 4(3), 587-603.
Valverde, M., Luciano, M. C., Gutiérrez Martí nez, O., & Hernández López, M. (2004). Tranfer of latent inhibition of aversively conditioned autonomic responses through equivalence classes. International Journal of Psychology and Psychological Therapy, 4, 605-622.
Stewart, I., Barnes-Holmes, D., & Roche, B. (2004). A functional-analytic model of analogy using the relational evaluation procedure. The Psychological Record, 54, 531-552.
This study provides an empirical demonstration of analogy using the Relational Evaluation Procedure (REP), a recently developed technique for the rapid training and testing of derived stimulus relations. The experiment involved 9 stages in which 5 adult male subjects were exposed to a complex series of REP training and testing protocols, by the end of which they each readily demonstrated 24 completely novel instances of responding in accordance with analogical relations as conceptualized by RFT.
Smeets, P. M., van Wijngaarden, M., Barnes-Holmes, D., & Cullinan, V. (2004). Assessing stimulus equivalence with a precursor to the relational evaluation procedure. Behavioural Processes, 65, 241-251.
Whelan, R., & Barnes-Holmes, D. (2004a). The transformation of consequential functions in accordance with the relational frames of same and opposite. Journal of the Experimental Analysis of Behavior, 82, 177-195.
Formative augmenting, behavior due to relational networks that establish given consequences as reinforcers or as punishers, was demonstrated in accordance with Same and Opposite relational networks. Some stimuli acquired reinforcing functions, based on the derived relation of Opposite, although in some cases no such function had actually been established for any member of the network. These effects were also observed across ABA reversals in the baseline contingencies.
Whelan, R., & Barnes-Holmes, D. (2004b). Empirical models of formative augmenting in accordance with the relations of same, opposite, more-than, and less-than. International Journal of Psychology and Psychological Therapy, 4, 285-302.
Authors demonstrated through two experiments that stimuli acquired reinforcing functions based on derived relational networks. This research supports the idea of formative augmenting: the degree to which events function as consequences was altered based on relational networks of Same and Opposite and more-than and less-than.
2003
Carpentier, F., Smeets, P. M., & Barnes-Holmes, D. (2003a). Equivalence-equivalence as a model of analogy: Further analyses. The Psychological Record, 53, 349-372.
This study attempted to train equivalence-equivalence relations with 5-year-old children. Only 8 of 18 showed equivalence-equivalence relations when tested. The procedure was then tested with adults and was successful with all of them.
Carpentier, F., Smeets, P. M., & Barnes-Holmes, D. (2003b). Matching unrelated stimuli with same discriminative functions: Training order effects. Behavioural Processes, 60, 215-226.
Carr, D. (2003). Effects of exemplar training in exclusion responding on auditory-visual discrimination tasks with children with autism. Journal of Applied Behavior Analysis, 36, 507-524.
Showed that multiple-exemplar training with auditory-visual exclusion tasks facilitated nonreinforced exclusion performances which reduced error rates on subsequent novel stimulus sets.
Smeets, P. M., & Barnes-Holmes, D. (2003). Children's emergent preferences for soft drinks: Stimulus-equivalence and transfer. Journal of Economic Psychology, 24, 603-618.
Smeets, P. M., Barnes-Holmes, Y., Akpinar, D. & Barnes-Holmes, D. (2003). Reversal of equivalence relations. The Psychological Record, 53, 91-120.
2002
Carpentier, F., Smeets, P. M., & Barnes-Holmes, D. (2002a). Establishing transfer of compound control in children: A stimulus control analysis. The Psychological Record, 52, 139-158.
Carpentier, F., Smeets, P. M., & Barnes-Holmes, D. (2002b). Matching functionally-same relations: Implications for equivalence-equivalence as a model for analogical reasoning. The Psychological Record, 52, 351-312.
This study tested equivalence-equivalence and nonequivalence-nonequivalence relations with adults, 9-year-olds, and 5-year-olds. Most of the adults and 9-year-olds demonstrated these relations, but the 5-year-olds did not.
Dougher, M., Perkins, D. R., Greenway, D., Koons, A., & Chiasson, C. (2002). Contextual control of equivalence-based transformation of functions. Journal of the Experimental Analysis of Behavior, 78, 63-94.
Transformation of functions among members in equivalence classes
Gomez, S., Barnes-Holmes, D., & Luciano, M. C. (2002). Generalized break equivalence II: Contextual control over a generalized pattern of stimulus relations. The Psychological Record, 52, 203-220.
Building on the work of Gomez et al (1999; 2001), the authors established effective contextual control over the Generalised Break Equivalence Pattern (GBEP) which provides further support for the generalized operant nature of derived relational responding.
Luciano, C., Barnes-Holmes, Y., & Barnes-Holmes, D. (2002). Establishing reports of saying and doing and discriminations of say-do relations. Research in Developmental Disabilities, 23, 406-421.
Markham, M.R., Dougher, M.J. & Augustson, E.M. (2002). Transfer of operant discrimination and respondent elicitation via emergent relations of compound stimuli. Psychological Record, 52(3), 325-350.
O'Hora, D., Roche, B., Barnes-Holmes, D., & Smeets, P. (2002). Response latencies to multiple derived stimulus relations: Testing two predictions of Relational Frame Theory. The Psychological Record, 52, 51-75.
The authors measured response latencies to mutually entailed same, opposite, more-than, and less-than relations. Response latencies to same and opposite relations were significantly faster than more-than and less-than relations. A second experiment showed a gradual decrease in response latency for more/less relations across a novel stimulus set.
Stewart, I., Barnes-Holmes, D., & Roche, B., & Smeets, P. M. (2002a). Stimulus equivalence and non-arbitrary relations. The Psychological Record, 52, 77-88
Stewart, I., Barnes-Holmes, D., Roche, B., & Smeets, P. M. (2002b). A functional-analytic model of analogy: A relational frame analysis. Journal of the Experimental Analysis of Behavior, 78, 375-396.
This study explored a behavior-analytic model of analogical reasoning, defined as the discrimination of formal similarity via equivalence-equivalence responding. Equivalence classes were trained, and subjects responded according to equivalence-equivalence relations. Subjects discriminated by shape or color of a relata. Transformation of stimulus functions of a block-sorting task based on this model of analogy was also shown.
2001
Barnes-Holmes, Y. Barnes-Holmes, D. Roche, B, & Smeets, P. M. (2001a). Exemplar training and a derived transformation of function in accordance with symmetry: I. The Psychological Record, 51, 287- 308.
This paper demonstrates that multiple exemplar training provides the necessary history to establish transformation across symmetry relations. Four studies confirmed that after relatively few exemplar training sessions, transformation could occur even across response modalities.
Barnes-Holmes, Y. Barnes-Holmes, D. Roche, B, & Smeets, P. M. (2001b). Exemplar training and a derived transformation of function in accordance with symmetry II. The Psychological Record, 51, 589-603.
This study clears some questions raised by Part I. Specifically, the authors found that naming is not a critical component of transformation, and children could readily demonstrate transformed functions in accordance with symmetry with no history of naming. The third part of the study examined the effects of pre-training. Results suggest that pre-training may be effective, but if not, to forgo additional pre-training and move immediately to multiple exemplar training.
Cullinan, V. A., Barnes-Holmes, D., & Smeets, P. M. (2001). A precursor to the relational evaluation procedure: Searching for the contextual cues that control equivalence responding. Journal of the Experimental Analysis of Behavior, 76, 339-349.
Fitzgerald, D. L. (2001). The effects of fluency in the acquisition of conditional, symmetric, and equivalence relations on the emergence of derived relational responding and the contextual control of relational behavior. Dissertation Abstracts International: Section B: The Sciences and Engineering, 61(9-B).
Gomez, S., Barnes-Holmes, D., & Luciano, M. C. (2001). Generalized break equivalence I. The Psychological Record, 51, 131-150.
The objective of this study was to produce responding in accordance with symmetry and transitivity but not with equivalence across novel stimulus sets. Building on the work of Gomez et al (1999), the authors employed several new procedures to generate ‘broken’ equivalence relations which provides support for the generalized operant nature of derived relational responding.
Leader, G., & Barnes-Holmes, D. (2001). Establishing fraction-decimal equivalence using a respondent-type training procedure. The Psychological Record, 51, 151-166.
Leader, G., & Barnes-Holmes, D. (2001). Matching-to-sample and respondent-type training as methods for producing equivalence relations: Isolating the critical variable. The Psychological Record, 51, 429-444.
Luciano, M. C., Herruzo, J., & Barnes-Holmes, D. (2001). Generalization of say-do correspondence. The Psychological Record, 51, 111-130.
Lyddy, F., Barnes-Holmes, D., & Hampson, P. J. (2001). A transfer of sequence function via equivalence in a connectionist network. The Psychological Record, 51, 409-428.
O'Hora, D., Barnes-Holmes, D., & Roche, B. (2001). Developing a procedure to model the establishment of instructional control. Experimental Analysis of Behavior Bulletin, 19, 13-15.
The authors measured response latencies to mutually entailed same, opposite, more-than, and less-than relations. Response latencies to same and opposite relations were significantly faster than more-than and less-than relations. A second experiment showed a gradual decrease in response latency for more/less relations across a novel stimulus set.]
Smeets, P. M., Barnes-Holmes, D., & Roche, B. (2001). Derived stimulus-response and stimulus-stimulus relations in children and adults: Assessing training order effects. Journal of Experimental Child Psychology, 78, 130-154.
Osborne, J.G. & Koppel, L. (2001). Acquisition, generalization, and contextual control of taxonomic and thematic relational responding. Psychological Record, 51(2), 185-205.
Stewart, I., Barnes-Holmes, D., Roche, B., & Smeets, P. M. (2001). Generating derived relational networks via the abstraction of common physical properties: A possible model of analogical reasoning. The Psychological Record, 51, 381-408.
This study demonstrated equivalence-equivalence responding based on the abstraction of common formal properties.
2000
Augustson, E.M., Dougher, M.J. & Markham, M.R. (2000). Emergence of conditional stimulus relations and transfer of respondent eliciting functions among compound stimuli. Psychological Record, 50(4), 745-770.
Transfer of respondent eliciting functions occurs even among compound stimuli.
Barnes-Holmes, D., Keane, J., Barnes-Holmes, Y., & Smeets, P. M. (2000). A derived transformation of emotive functions as a means of establishing differential preferences for soft drinks. The Psychological Record, 50, 493-511.
Carpentier, F., Smeets, P. M., & Barnes-Holmes, D. (2000). Matching compound samples with unitary compounds: Derived stimulus relations in adults and children. The Psychological Record, 50, 671-686.
Carr, D., Wilkinson, K. M., Blackman, D., & McIlvane, W. J. (2000). Equivalence classes in individuals with minimal verbal repertoires. Journal of the Experimental Analysis of Behavior, 74, 101-115.
Cullinan, V. A., Barnes-Holmes, D., & Smeets, P. M. (2000). A precursor to the relational evaluation procedure. II.The Psychological Record, 50, 467-492.
Healy, O., Barnes-Holmes, D., & Smeets, P.M. (2000). Derived relational responding as generalised operant behaviour. Journal of the Experimental Analysis of Behaviour, 74, 207-227.
Demonstrated that response patterns on novel stimulus sets was controlled by the feedback delivered for previous stimulus sets.
Leader, G., Barnes-Holmes, D., & Smeets, P. M. (2000). Establishing equivalence relations using a respondent-type training procedure III. The Psychological Record, 50, 63-78.
Similar to the study above but with young children as subjects.
Roche, B., Barnes-Holmes, D., Smeets, P. M., Barnes-Holmes, Y., & McGeady, S. (2000). Contextual control over the derived transformation of discriminative and sexual arousal functions. The Psychological Record, 50, 267-291.
Following on from Roche and Barnes (1997) and McGeady and Roche (1997), the authors demonstrate four distinct contextually-controlled transformations of function by presenting the contextual cue along with the derived stimuli. Skin resistance responses and operant discriminations are measured. Still the only study to employ such a testing format.
Smeets, P.M., Barnes-Holmes, D., & Cullinan, V. (2000). Establishing equivalence classes with match-to-sample format and simultaneous-discrimination format conditional discrimination tasks. The Psychological Record, 50, 721-744.
Smeets, P. M., Dymond, S., & Barnes-Holmes, D. (2000). Instructions, stimulus equivalence, and stimulus sorting: Effects of sequential testing arrangements and a default option. The Psychological Record, 50, 339-354.
1999
Gomez, S., Huerta, F., Barnes-Holmes, D., & Luciano, C. (1999). Breaking equivalence relations. Experimental Analysis of Human Behavior Bulletin, 17, 1-4.
The objective of this study was to produce responding in accordance with symmetry and transitivity but not with equivalence, across novel stimulus sets.
Smeets, P. M., Barnes, D., & Luciano, C. M. (1999). Reversal of emergent simple discrimination in children: A component analysis. Journal of Experimental Child Psychology, 60(3), 327-343.
1998
Cullinan, V. A., Barnes, D., & Smeets, P. M. (1998). A precursor to the relational evaluation procedure: Analyzing stimulus equivalence.The Psychological Record, 48, 121-145.
Dymond S. & Barnes D. (1998). The effects of prior equivalence testing and verbal instructions on derived self-discrimination transfer: A follow-up study. Psychological Record 48(1), 147-170.
A follow-up study to Dymond & Barnes (1994). Subjects were not given equivalence training this time but were instead trained in a series of conditional discriminations. Also, some subjects were given extensive instructions and others were given minimal instructions. Neither of these factors affected the subjects performance and the results from previous experiments were replicated.
Hayes, S. C., & Bissett, R. (1998). Derived stimulus relations produce mediated and episodic priming. The Psychological Record, 48, 617-630.
Showed that priming effects that are well known in semantically related words also occurred in nonsense stimuli related through equivalence.
Healy, O., Barnes-Holmes, D., & Smeets, P.M. (1998). Derived relational responding as an operant: The effects of between-session feedback. The Psychological Record, 48, 511-536.
Delivering accurate or inaccurate feedback to subjects following a test for derived equivalence relations produces responding on subsequent tests that is consistent with that feedback. One of the first to demonstrate the operant nature of relation responding.
1997
Barnes, D., Hegarty, N., & Smeets, P. M. (1997). Relating equivalence relations to equivalence relations: A relational framing model of complex human functioning. The Analysis of Verbal Behavior, 14, 57-83.
This study examined the RFT approach to analogical reasoning. Subjects were trained on several equivalence relations. They were then shown pairs of relata in which both of the relata were from the same relation or in which both relata were from different relations. The subjects successfully matched pairs of same with same and different with different.
McGeady, S. & Roche, B. (1997). A contextually controlled transformation of operant response functions in accordance with arbitrarily applicable relations. Experimental Analysis of Human Behavior Bulletin, 15, 12-13.
Roche, B., & Barnes, D. (1997). A transformation of respondently conditioned sexual arousal functions in accordance with arbitrary relations. Journal of the Experimental Analysis of Behavior, 67, 275-301.
The first study to show a transformation of respondently conditioned sexual arousal functions, measured as skin resistance responses, through same and opposite relations. An excellent demonstration of how to conduct complex electrodermal research within an RFT framework.
Roche, B., Barnes, D., & Smeets, P. M. (1997). Incongruous stimulus pairing and conditional discrimination training: Effects on relational responding. Journal of the Experimental Analysis of Behavior, 68, 143-160.
Smeets, P., & Barnes, D. (1997). Emergent conditional discrimination in children and adults: Stimulus equivalence derived from simple discriminations. Journal of Experimental Child Psychology, 66, 64-84.
Smeets, P., Barnes, D., & Roche, B. (1997). Functional equivalence in children. Derived stimulus-response and stimulus-stimulus relations. Journal of Experimental Child Psychology, 66, 1-17.
Smeets, P.M., Leader, G., & Barnes, D. (1997). Establishing stimulus classes with adults and children using a respondent training procedure: A follow-up study. The Psychological Record, 47, 285-308.
1996
Barnes, D., Lawlor, H., Smeets, P. M., & Roche, B. (1996). Stimulus equivalence and academic self-concept in mildly mentally handicapped and non-mentally handicapped children. The Psychological Record, 46, 87-107.
Using educationally-relevant real world stimuli such as "slow" and "able" as well as the subject's own name, the authors show how developmentally-delayed children come to fail tests for equivalence when the predicted outcome is in contrast to their learning history. That is, subjects did not relate their own name to "able." A neat study on prior-learning effects in equivalence formation.
Dymond, S. & Barnes, D. (1996). A transformation of self-discrimination response functions in accordance with the arbitrarily applicable relations of sameness and opposition. The Psychological Record, 46, 271-300.
Demonstrates a transformation of functions in accordance with sameness and opposition, using several matching-to-sample control tasks to prevent formation of simple equivalence and nonequivalence relations.
Grey, I., & Barnes, D. (1996). Stimulus equivalence and attitudes. The Psychological Record, 46, 243-270.
Leader, G., Barnes, D., & Smeets, P.M. (1996). Establishing equivalence relations using a respondent-type training procedure. The Psychological Record, 46, 685-706.
The first in a series of studies investigating a new procedure for the derivation of equivalence relations. “Training” merely involves observing on-screen presentations of stimulus pairs and then testing for equivalence using a match-to-sample format. More effective in establishing equivalence than standard MTS arrangements.
Roche, B., & Barnes, D. (1996). Arbitrarily applicable relational responding and sexual categorization: A critical test of the difference relation. The Psychological Record, 46, 451-475.
After Steele & Hayes, the first study to systematically examine the relational frame of distinction using socially-loaded stimuli. This study inspired a series of exchanges between the authors and Richard Saunders in the same volume on the relationship between equivalence and RFT.
Smeets, P., Barnes, D., & Schenk, J., & Darcheville, J., (1996). Emergent simple discriminations and conditional relations in children, adults with mental retardation, and normal adults. Quarterly Journal of Experimental Psychology, 49(B), 201-219.
Wilson, K. G. & Hayes, S. C. (1996). Resurgence of derived stimulus relations. Journal of the Experimental Analysis of Behavior, 66, 267-281.
1995
Barnes, D., Browne, M., Smeets, P., & Roche, B. (1995). A transfer of functions and a conditional transfer of functions through equivalence relations in three- to six-year-old children. The Psychological Record, 45, 405-430.
Transfer and contextually-controlled transfer in kids of different ages with the older subjects passing the more complex tests. A nice example of a nonautomated transfer study.
Dymond, S. & Barnes, D. (1995). A transformation of self-discrimination response functions in accordance with the arbitrarily applicable relations of sameness, more-than, and less-than. Journal of the Experimental Analysis of Behavior, 64, 163-184. Erratum, 66, 348.
The first study to show three patterns of derived relational responding in accordance with sameness, more-than, and less-than. Alternative explanations for the transformation test outcomes are considered and found wanting. The relational network figure has been reproduced in several different publications
Smeets, P. M., & Barnes, D. (1995). Emergent simple discrimination via transfer from differentially reinforced S+ stimuli: A further test of the stimulus-response interaction model. Quarterly Journal of Experimental Psychology, 48B(4), 329-345.
Smeets, P., Barnes, D., & Luciano, C. (1995). Total reversal of emergent simple discrimination in children: A component analysis. Journal of Experimental Child Psychology, 60, 327-343.
Smeets, P., Schenk, J., & Barnes, D. (1995). Establishing arbitrary stimulus classes via identity matching training and non-reinforced matching with complex stimuli. Quarterly Journal of Experimental Psychology, 48B(4), 311-328.
1994
Barnes, D. (1994). Stimulus equivalence and relational frame theory. The Psychological Record, 44, 91-124.
A cogent introduction to RFT in which the author compares "Sidman equivalence" with RFT, offers a respondent analysis of symmetry, and predicts various outcomes of training designs. Good for an undergraduate introduction to the area
Cullinan, V., Barnes, D., Hampson, P. J., & Lyddy, F. (1994). A transfer of explicitly and nonexplicitly trained sequence responses through equivalence relations: An experimental demonstration and connectionist model. The Psychological Record, 44, 559-585.
Dougher, M. J., Augustson, E., Markham, M. R., Greenway, D. E., & Wulfert, E. (1994). The transfer of respondent eliciting and extinction functions through stimulus equivalence classes. Journal of the Experimental Analysis of Behavior, 62, 331-351.
One of the early articles studying the transfer of respondent eliciting functions.
Dymond, S., & Barnes, D. (1994). A transfer of self-discrimination response functions through equivalence relations.Journal of the Experimental Analysis of Behavior, 62, 251-267.
Four subjects were trained in matching-to-sample tasks and equivalence relations. They showed the expected transfer of self-discrimination response functions. Four control subjects either received training in matching to sample but were not tested on equivalence or were trained and tested using stimuli not used in the transfer test. None of these showed the transfer of self-discrimination response functions.
Hayes, L. J., Brenner, K., & Hayes, S. C. (1994). Assessing pre-existing stimulus relations via stimulus equivalence.Mexican Journal of Behavior Analysis, 20, 146-166.
1993
Barnes, D., & Hampson, P. (1993). Stimulus equivalence and connectionism: Implications for behavior analysis and cognitive science. The Psychological Record, 43, 617-638.
Barnes, D., & Keenan, M. (1993). A transfer of functions through derived arbitrary and non-arbitrary stimulus relations. Journal of the Experimental Analysis of Behavior, 59, 61-81.
An elegant demonstration of transfer of functions through equivalence relations, with and without a prior equivalence test, and a generalised transfer through non-arbitrary relations. One of the most-cited transfer articles.
Lipkens, R., Hayes, S. C., & Hayes, L. J. (1993). Longitudinal study of the development of derived relations in an infant. Journal of Experimental Child Psychology, 56, 201-239.
Showed the development of derived stimulus relations, including equivalence and exclusion, in a human infant.
Schusterman, R. J. & Kastak, D. (1993). A California sea lion (Zalophus californianus) is capable of forming equivalence relations. The Psychological Record, 43, 823-840.
Zentall, T. R., & Urcuioli, P. J. (1993). Emergent relations in the formation of stimulus classes in pigeons. The Psychological Record, 43, 795-810.
1991
Hayes, S. C., Kohlenberg, B. K., & Hayes, L. J. (1991). The transfer of specific and general consequential functions through simple and conditional equivalence classes. Journal of the Experimental Analysis of Behavior, 56,119-137.
Showed the transfer of consequential functions through equivalence relations, both simple and conditional.
Kohlenberg, B. S., Hayes, S. C., & Hayes, L. J. (1991). The transfer of contextual control over equivalence classes through equivalence classes: A possible model of social stereotyping. Journal of the Experimental Analysis of Behavior, 56, 505-518.
Showed that transfer effects extended to conditional stimuli that themselves regulated derived relational responding. Extends the analysis to social stereotyping
Steele, D., & Hayes, S. C. (1991). Stimulus equivalence and arbitrarily applicable relational responding. Journal of the Experimental Analysis of Behavior, 56, 519-555.
The first experimental demonstration that establishing cues that controlled non-arbitrary stimulus relations later produced multiple forms of derived relational responding with arbitrary stimulus sets. One of the first clear experimental demonstrations of RFT.
Watt, A., Keenan, M., Barnes, D., & Cairns, E. (1991). Social categorization and stimulus equivalence. The Psychological Record, 41, 33-50.
This study examined whether social categorization could be explored in terms of stimulus equivalence by testing whether equivalence training could be transferred to untrained social stimuli. The study had Irish Protestants, Irish Catholics and English Protestants go through a series of matching-to-sample procedures in which they were trained to match Protestant or Catholic stimuli with non-sense syllables. The findings suggest that previous learning might interfere with equivalence responding in the experimental training.
1990 and earlier
Barnes, D., McCullagh, P. D., & Keenan, M. (1990). Equivalence class formation in non-hearing impaired children and hearing impaired children. The Analysis of Verbal Behavior, 8, 19-30.
Hayes, L. J., Thompson, S., & Hayes, S. C. (1989). Stimulus equivalence and rule following. Journal of the Experimental Analysis of Behavior, 52, 275-291.
Authors describe results of two studies attempting to specify the relationship between verbal and nonverbal behavior in the context of rule following. Two stimulus equivalence relationships were trained and then subjects were tested for production of novel behavior. Novel behavior was produced in both the presence and absence of names provided for the equivalence classes.
De Rose, J. C., McIlvane, W. J., Dube, W. V., Galpin, V. C., & Stoddard, L. T. (1988). Emergent simple discrimination established by indirect relation to differential consequences. Journal of the Experimental Analysis of Behavior, 50, 1-20.
One of the early articles studying the transfer of stimulus functions among members in equivalent classes.
Wulfert, E., & Hayes, S. C. (1988). Transfer of a conditional ordering response through conditional equivalence classes. Journal of the Experimental Analysis of Behavior, 50, 125-144.
Hayes, S. C., Brownstein, A. J., Devany, J. M., Kohlenberg, B. S., & Shelby, J. (1987). Stimulus equivalence and the symbolic control of behavior. Mexican Journal of Behavior Analysis, 13, 361-374.
Showed the transfer of discriminative functions through equivalence relations
Devany, J. M., Hayes, S. C., & Nelson, R. O. (1986). Equivalence class formation in language-able and language-disabled children. Journal of the Experimental Analysis of Behavior, 46, 243-257.
Showed a correlation between receptive language skills and the derivation of equivalence. Interpreted this correlation in RFT terms, suggesting that the correlation was due to the functional overlap of the two tasks.
Derived Relations Task With a Chimpanzee (video)
Derived Relations Task With a Chimpanzee (video)http://www.youtube.com/watch?v=NcgI-rxJOP8
Description: This is an old clip that's been used in a number of introductory RFT / derived relations slideshows. The video shows a chimpanzee having great difficulty in her efforts to solve a bidirectional task (after having learned a correspondence between different people and different letters on a keyboard, she has to «say» who goes to who by using a symbol meaning «to go to»).
RFT Videos
RFT VideosYou must sign into your ACBS account to watch these videos.
ACBS World Conference Videos
- How to do an RFT- Enlighted Functional Analysis of Clinical Work (ACBS World Conference 17, Dublin, Ireland)
- Mastering the Clinical Conversation with RFT (ACBS World Conference 16, Montréal, Canada)
- Implications of Relational Frame Theory for Early Childhood Language Development (ACBS World Conference 16, Montréal, Canada)
- How RFT can make you smarter (ACBS World Conference 16, Montréal, Canada)
- An Experiential Introduction to Relational Frame Theory (ACBS World Conference 16, Montréal, Canada)
- Mastering the Clinical Conversation (ACBS World Conference 15, Seville, Spain)
- The RFT of Meditation (ACBS World Conference 11, Sydney, Australia)
- Do you know your ABCs from your RFTs?: A Workshop on Relational Frame Theory (ACBS World Conference 11, Sydney, Australia)
- Deriving RFT: How to spread the visibility of our research and how to make its applications more accessible (ACBS World Conference 10, Washington D.C., USA)
- Social Communication and RFT (ACBS World Conference VIII, Reno, Nevada)
- Using RFT to Create Powerful Therapeutic Metaphors (ACBS World Conference II, London, UK)
More RFT Videos
-
Click here for the full list of RFT videos (must sign into your ACBS account to view the videos)
Advances in Relational Frame Theory: Research and Application -- Book Interview
Advances in Relational Frame Theory: Research and Application -- Book InterviewEdited by leading Relational Frame Theory (RFT) scholars, Simon Dymond, PhD, and Bryan Roche, PhD, Advances in Relational Frame Theory presents advances in all aspects of RFT research over the last decade, and provides a greater understanding of the core principals of acceptance and commitment therapy (ACT). The book also contains chapters written by Steven C. Hayes and Kelly Wilson, both research-active experts from the RFT community around the world.
Below, the book's editors Simon Dymond and Bryan Roche discuss the book, as well as the future of RFT.
Q: So what in a nutshell is Relational Frame Theory (RFT)?
Relational Frame Theory (RFT) is a contextual behavioral theory of language and cognition. It holds that the essence of language and cognitive thought is relational in nature.
Q: Why did you produce this book and why now?
As we outline in the Preface, it's been more than ten years since the publication of the first edited volume on RFT: the so-called, "purple book" (Hayes, Barnes-Holmes, & Roche, 2001).
Q: Who is the target audience?
Everyone with an interest in behaviour analysis, verbal behaviour, language and cognition, and clinical therapy. Really, there's something for everyone in the book, be they students, researchers, clinicians or just interested in what modern behaviour analysis has got to say about complex human behaviour.
Q: What might therapists, or other practitioners, and researchers get from the book?
RFT has truly emerged from a very healthy applied-basic research agenda. The theory has been informed from the beginning by the concerns of those trying to explain real world phenomena in the clinic, work or social setting. But it has also been built from the ground up based on sound principles of behavior analysis. So this theory speaks very well to therapists and practitioners in the work or clinical setting. RFT is not an esoteric theory – we always have our eye on the prize, which is not surprising given that we are pragmatists.
Several chapters in the book deal with clinical issues, and explain what RFT has to offer by way of well worked out functional explanations of clinical phenomena. These analysis have very real and immediate implications for the practice of therapy and show how RFT feeds directly into clinical practice. A further chapter illustrates the application of RFT to understanding behavior and behavior change in the workplace. These chapters will help practitioners get a grip on how it is precisely that RFT underpins therapeutic practices such as those used in Acceptance and Commitment Therapy (ACT) and other mindfulness based treatments. It is an excellent primer for a practitioner who wants a one-stop-shop for everything you needed to know about ACT and RFT.
But researchers will also get a lot from this book. Several chapters outline the verbal/relational underpinnings of clinical problems, which has the potential to better inform novel therapeutic interventions and to inspire exciting translational research endeavours. It represents the latest compendium of advances made in basic RFT research this past decade and is an essential book for any basic researchers interested in cutting edge changes in the experimental analysis of language and cognition. In other words, it's sssential reading for all those interested in clinical issues!
Q: What are some highlights of the book?
That's a hard question; there are so many highlights! Perhaps one of the most exciting advances made in RFT in recent years is its interfacing with neuroscience. The use of fMRI and EEG measures have complimented the development of RFT and some very impressive studies and analyses have been conducted since the publication of the first RFT book in 2001. These studies allow us to speak directly to neuroscientists and to validate some of the predictions of RFT regarding the verbal nature of the transformation of functions and to identify the neural correlates of language and cognitive phenomena in behavioral terms. Many readers will also be keen to read the chapter on the Implicit Relational Assessment Procedure (IRAP), which has also been developed since the 2001 RFT book. The IRAP uses an RFT approach to implicit testing to develop a test that allows researchers to measure implicit attitudes with an empirical integrity that probably outshines that achieved by the eponymous Implicit Association Test. This an excellent example of the application of RFT in domains of research (in this case social cognition) that were typically avoided by behavior analysts. It also represents an excellent example of bridge-building across the various domains of psychology and an impressive example of the kinds of translational research behavior analysts need to be doing.
We should also point out that there is an important conceptual chapter in the book in which the approach to science that we call contextual behavioral science (CBS), is integrated into a larger body of selectionist and contextualistic scientific approaches, namely evolution theory. This is an important new illustration of the fact that contextual behavioral science is quite an all-encompassing approach to science that can move us closer to a single, but multi-level and unified account of individual’s behavior. These types of conceptual advances are very exciting and very important for assessing the maturity and progressiveness of the CBS approach.
But, there are 11 chapters in the book, and all are worth highlighting!
Q: What are the future challenges and opportunities for RFT?
RFT is still a young theory in terms of the number of basic researchers who employ it as a paradigm in their basic research. It has come a long way but we need to see more translational work being done so that researchers and practitioners in other fields sit up and take notice. This has already started to happen in the fields of experimental psychopathology and implicit testing, and of course it has already happened for ACT in the world of therapy.
Numerous challenges lie ahead, such as ensuring new organisations like ACBS and journals such as JCBS are able to continue to "spread the word" about RFT to a wider audience, especially given ongoing changes in scholarly publishing models and the growth of open access solutions. This is balanced, however, by numerous emerging opportunities such as the widespread acceptance that verbal/relational processes may play an important role in causing and maintaining human suffering (and the potential for RFT to inform such clinical theories), the fact that RFT is uniquely positioned to contribute its own functional account of language and cognition to debates underway in cognitive science and clinical psychology (Jan De Houwer, in the Foreword to the book, makes a great point in this regard), and the momentum behind ACBS and other organisations in reaching out and developing a genuine community of researchers, clinicians and students interested in RFT and its implications. We think the best service we can do for behavior analysis is to showcase RFT as our crowning achievement to date, and to do our best to use it to bring a behavior-analytic perspective to all and any behavior, regardless of their apparent level of complexity.
Implicit Relational Assessment Procedure (IRAP) Website
Implicit Relational Assessment Procedure (IRAP) WebsiteWeb Address (URL):
An implementation of the IRAP is now freely available in open source form, running in PsychoPy (www.psychopy.org), and is now compatible with OSX, Windows, and Linux platforms at the above address. The original implementation of the IRAP in Visual Basic 6 can still downloaded using the attachment on the bottom of this page.
Description:
The IRAP was built out of RFT, the central postulate of which is that higher-cognitive functioning is composed of relational acts. Initial studies have shown that the IRAP may be used to measure relational networks or beliefs that are not readily accessible to the researcher or perhaps even the participant. The IRAP appears to offer advantages over other methods that use reaction time measures to assess beliefs or attitudes (e.g. the Implicit Association Test; IAT), both in its theoretical rationale and its ability to measure many types of relationships. This website provides an introduction to the IRAP research programme and access to the IRAP software and supporting materials.
RFT Research Archives
RFT Research ArchivesApplied RFT
Applied RFTThe most obvious form of "applied" RFT is Acceptance and Commitment Therapy. However, ACT is only one small portion of the applied work being done that utilizes RFT concepts.
Indeed, the principles of RFT and procedures that RFT researchers are honing can be widely applicable to learning, education, child and adult development, clinical problems, and much more.
Below are some areas in which RFT is being used to predict and influence complex human phenomena and to help improve interventions in many clinically relevant areas.
RFT and Perspective Taking
Perspective-taking is a word that refers to a common experience in every one’s life. Behavioral scientists have talked about perspective-taking in many different ways, but the field tends to conceptualize that skill as an intrinsic capacity very often not susceptible to direct manipulation or training, which from a functional contextual point of view is not very useful. Additionally, RFT links this skill to other diverse psychological phenomena such as intelligence or experiential avoidance and it does it from a unique and theoretically coherent framework.
Nowadays, although the RFT started with work on children and kids with developmental disabilities, the literature is expanding to phenomena such as stigma (see Vilardaga et al. 2008 ppt), social anhedonia and psychosis (see Villatte et al, papers in the publication section). Perspective taking is a central aspect of what makes us most human: our ability to interact effectively with other human beings and to form groups, communities, countries and coalitions of countries. Work on deictic framing is a good example of the broad applicability of behavioral principles to human affairs.
RFT and Intervention in Autism Spectrum Disorder
A key aspect of language, and one that is at the core of communication deficits for children with autism, is generativity—put simply, the ability to produce or understand totally new sentences. Understanding and accounting for linguistic generativity is critical to any account of language development (Malott, 2003), and to the creation of programs for teaching flexible and fully functional language repertoires. RFT provides new insight into the issue of generativity, by conceptualizing the core skill in language as learned contextually controlled relational responding (referred to as relational framing).
Typically developing children learn relational framing through natural language interactions during which they are exposed to contingencies that establish these response patterns (e.g., Lipkens, Hayes & Hayes, 1993; Luciano, Gómez & Rodríguez, 2007). However, children with autism spectrum disorders (ASD) do not easily learn this key form of responding (e.g., Rehfeldt, Dillen, Ziomek, & Kowalchuk, 2007) —while many children with ASD are able to learn functional language skills through explicit training, language use for many remains rote, despite intensive intervention (see, e.g., Luciano, Rodriguez, Manas, Ruiz, Berens, & Valdivia-Salas, 2009).
A number of recently published RFT-based studies, however, (e.g., Murphy, Barnes-Holmes & Barnes-Holmes, 2005; O’Connor, Rafferty, Barnes-Holmes & Barnes-Holmes, 2009) have begun to show that relational framing can be successfully trained in developmentally delayed populations including individuals with ASD. This work holds great promise for the future.
REFERENCES
- Lipkens, R., Hayes, S.C., & Hayes, L.J. (1993). Longitudinal study of the development of derived relations in an infant. Journal of Experimental Child Psychology, 56, 201-239.
- Luciano, C., Gomez Becerra, I. & Rodriguez Valverde, M. (2007). The role of multiple- exemplar training and naming in establishing derived equivalence in an infant. Journal of the Experimental Analysis of Behavior, 87, 349-365.
- Luciano, C., Rodriguez, M., Manas, I., Ruiz, F., Berens, N., & Valdivia-Salas, S. (2009). Acquiring the earliest relational operants: coordination, distinction, opposition, comparison and hierarchy. In Rehfeldt, R.A. & Barnes-Holmes, Y. (Eds.). Derived Relational Responding: Applications for Learners with Autism and other Developmental Disabilities. CA: New Harbinger.
- Malott, R. W. (2003). Behavior analysis and linguistic productivity. Analysis of Verbal Behavior, 19, 11-18.
- Murphy, C., Barnes-Holmes, D. & Barnes-Holmes, Y. (2005). Derived manding in children with autism: Synthesizing Skinner's Verbal Behavior with relational frame theory. Journal of Applied Behavior Analysis, 59(1), 445-462.
- O’Connor, J., Rafferty, A., Barnes-Holmes, D. & Barnes-Holmes , Y. (2009). The role of verbal behavior, stimulus nameability and familiarity on the equivalence performances of autistic and normally-developing children. The Psychological Record, 59(1), 53-74.
- Rehfeldt, R.A. & Barnes-Holmes, Y. (2009). Derived Relational Responding: Applications for Learners with Autism and other Developmental Disabilities. CA: New Harbinger.
- Rehfeldt, R. A., Dillen, J. E., Ziomek, M. M., & Kowalchuk, R. E. (2007). Assessing relational learning deficits in perspective-taking in children with high functioning autism spectrum disorder. The Psychological Record, 57, 23-47.
Additional information will be added soon.
Research Procedures & Computer Programming
Research Procedures & Computer ProgrammingThis section of the site is for researchers to share custom computer programs, files, instructions, information, and data useful for running computer-controlled experimental procedures. It is our hope that in sharing such information we can develop best practices to reduce the influence of extraneous variables on the results of computer-controlled RFT studies. Please share with the community what you and your lab do.
Disclaimer: All software and files provided on this site are distributed on an "as is" basis. The webmaster or authors of the programs assume no responsibility for problems or damage resulting from the use of these products.
Features of Well-Controlled Experimental Analogs
Features of Well-Controlled Experimental AnalogsThere have been a number of tightly controlled experimental studies, both on RFT and ACT processes. There are resources within the RFT section of the site that will help you with your own studies, but there are a few that are currently posted to the ACT section of the site that you might find useful as well.
Please visit the Component Studies Information page for information on features of experimental analogs and sample files (visual basic command code, videos, instructions, etc.) from an ACT component study.
GO-IRAP Software and Manual
GO-IRAP Software and Manual
Welcome to the Ghent-Odysseus Implicit Relational Assessment Procedure (GO-IRAP)!
- Training and Traditional Testing IRAPs
- Traditional (Label and Target) and Natural Language (Sentence) IRAP formats
- The easy input of complex languages and characters for stimuli and instructions
- The use of text or images as labels, targets, and response options
- Block level or trial-type level application of mastery criteria
- Label-Target-Response Option stimuli locking
- Incorrect and Correct responding feedback options
- One easily readable .txt data and experimental file
The 2 program files (32 bit and 64 bit versions) and the PDF of the manual are attached for all ACBS members to download.
We are also attaching a folder named 'Training IRAP' which was recently used at a workshop presented at the Division of Behavior Analysis Conference in Dublin to demonstrate how the Training IRAP can easily be used in ABA settings to teach both basic and complex relational skills (Barnes-Holmes, McEnteggart, & Kavanagh, 2017). This folder also contains a paper entitled 'Teaching Important Relational Skills for Children with Autism Spectrum Disorder and Intellectual Disability Using Freely Available (GO-IRAP) Software' which followed on from this workshop (Murphy & Barnes-Holmes, 2017).
Note: Bug Testing. We have been using the GO-IRAP in our research lab without encountering any problems, however, bug testing of the GO-IRAP is ongoing, so no guarantees can be made that no bugs or errors can be found within the program.
Note: Source Code. Because the GO-IRAP is still in the testing phase and there are additional features that we plan to add to the final version, we cannot make the source code available at this time, however we intend to make the source code open access in late 2020.
Also see the https://go-rft.com/ website!
Mixed Trial IRAP Software
Mixed Trial IRAP SoftwareAn introduction to the Mixed Trial Implicit Relational Assessment Procedure (MT-IRAP)
We designed this program to hopefully provide a more flexible and sensitive tool for examining implicit relational responding. In particular, we are interested in developing/refining an implicit measure that is sensitive and reliable for measuring implicit relational responding at the level of individual stimuli and individual participants (as opposed to implicit effects at the level of stimulus categories and participant groups).
Preliminary data suggests the MT-IRAP can be used to measure implicit relational responding at both the stimulus category and individual stimulus level (Levin, Hayes & Waltz, 2010). It is unclear whether this measure is sensitive and reliable at the level of individual participants and whether it is more or less effective than the standard IRAP. Further research is needed to determine the reliability and validity of this measure, particularly with more ambiguous stimuli (e.g., where participants may be unsure of what is “truth” and what is a “lie”).
At this point, the exact configuration of the MT-IRAP is somewhat of a moving target and depends on the specific research questions being asked. Due to this, the program we have created provides a wide variety of configuration options. The flexibility in this program will hopefully be helpful to you as a researcher, though it may also require more time figuring out how to use it and the most appropriate configuration for a given study.
Please log in and download the MT-IRAP instructions (attached to the bottom of this page), this document contains a great deal more information about the procedures strengths and limitations.
Also, for further information about the MT-IRAP, we’d recommend you read the following article:
Levin, M.E., Hayes, S.C. & Waltz, T. (2010). Creating an implicit measure of cognition more suited to applied research: A test of the Mixed Trial – Implicit Relational Assessment Procedure (MT-IRAP). International Journal of Behavioral Consultation and Therapy, 6, 245-262.
Disclaimer: This program is still being developed so you may run into errors while using it. Although we have tried to make it user friendly when possible, due to limited resources and the complexity of the program, it does require some time to get used to using.
National University of Ireland, Maynooth IRAP software
National University of Ireland, Maynooth IRAP softwareThe Implicit Relational Assessment Procedures (IRAP)
This software has been used extensively to assess implicit relational responding, or responding that is outside of conscious awareness. This program was developed as an alternative to the Implicit Assessment Test (IAT) which was developed with social psychology as a way to assess implicit biases. While the IAT requires participants to categorize lists of words, the IRAP is designed to assess relational responses using contextual cues of interest. There are numerous studies that have used the IRAP, compared its results to that of (explicit) self-reported beliefs, and some that have compared it directly to the IAT. See the Empirical Support page for a detailed list of studies.
Ole Miss IRAP software
Ole Miss IRAP softwareBelow is a zip file containing the Ole Miss IRAP (version 3.5). The program is easy to learn and readily adapted for your own research interests. The pdf file is the current manual for installing and using the program. I recommend reading this manual before anything else (it's only six pages). In addition to installation instructions and explanations of the program features, it also contains some useful information about handling participants and accessing data.
While the Ole Miss IRAP is copyrighted, this was done to keep it freely available. I encourage researchers to use, distribute, and modify the program as they see fit. Feel free to contact me if you encounter technical problems installing or using the program, or even if you would just like to bounce a study idea off of me. I'm all about the research and will do what I can to help.
Have fun!
Ole Miss Matching-to-Sample software
Ole Miss Matching-to-Sample softwareThe lab at the University of Mississippi has made software available for the traditional matching-to-sample procedure. Below is an attachment containing a Visual Basic.NET program for a three-member, three class procedure. You will need to be logged into the ACBS website as a member in order to see and download the attachment.
PsyScope: (Mac only) Easy-to-Use Software for Running Computer-Controlled Experiments
PsyScope: (Mac only) Easy-to-Use Software for Running Computer-Controlled ExperimentsPsyScope: Easy-to-Use Software for Running Computer-Controlled Experiments in Psychology
PsyScope is for the Macintosh Platform only but several FREE Apple Macintosh emulators are available for download on line. PsyScope (Cohen, MacWhinney, Flatt, & Provost, 1993) is a user-friendly freeware Macintosh application which undergoes on-going development by psychologists for psychologists. It is the easiest to use and most versatile experiment generation software available, and it’s free.
PsyScope allows researchers to design complex psychology experiments without the need for programming skills. As the user constructs spider diagrams in a graphic interface using a limited number of graphic tools, PsyScope writes a scripting file which can be accessed directly by users familiar with scripting.
Relational Completion Procedure (Dymond & Whelan, 2010)
Relational Completion Procedure (Dymond & Whelan, 2010)An alternative to match-to-sample procedures, the Relational Completion Procedure is available below.
The article is available in the publications section of the site, and by clicking directly here.
The "Relational Completion Procedure.zip" file below is the more recent of the two files. Updates may be available at Simon Dymond's website as well.
Training and Assessment of Relational Precursors and Abilities (TARPA)
Training and Assessment of Relational Precursors and Abilities (TARPA)Understanding and accounting for the ability to produce and understand completely novel sentences--accounting for the generativity of language--is critical to any account of language development (Malott, 2003), and to the creation of programs for teaching flexible and fully functional language repertoires.
RFT explains linguistic generativity in terms of learned contextually controlled relational responding referred to as relational framing. Typically developing children learn relational framing through natural language interactions during which they are exposed to contingencies that establish these response patterns (e.g., Lipkens, Hayes & Hayes, 1993; Luciano, Gómez & Rodríguez, 2007). However, children with autism spectrum disorders (ASD) do not easily learn this key form of responding (e.g., Rehfeldt, Dillen, Ziomek, & Kowalchuk, 2007). Nonetheless, they can benefit from training of this repertoire (e.g., Murphy & Barnes-Holmes, 2009).
The Training & Assessment of Relational Precursors & Abilities (TARPA) is a recently developed computer-based protocol for the assessment of a progression of key domains of responding critical to the development of generative language. The TARPA is comprised of ten stages as follows: (i) basic discrimination; (ii) conditional discrimination involving similarity; (iii) conditional discrimination involving non-similarity (2 comparisons); (iv) conditional discriminations involving non-similarity (3 comparisons); (v) mutually entailed relational responding [e.g., deriving the symmetrical relation B --> A from the trained relation A --> B] (2 comparisons); (vi) mutually entailed relational responding (3 comparisons); (vii) combinatorial entailed relational responding [e.g., deriving the combinatorial relations A --> C and C --> A when trained with A--> B and B--> C] (2 comparisons); (viii) transfer of function [responding to a stimulus in a new and appropriate way based on it’s participation in a derived sameness relation] (2 comparisons); (ix) combinatorial entailed relational responding (3 comparisons); (x) transfer of function (3 comparisons). Each stage is further subdivided into multiple levels, and in the stages assessing derived relations (i.e., Stages 5-10), levels are subdivided into training sections and derivation sections.
A preliminary version of the TARPA has been correlated with the Vineland Adaptive Behavior Scale (VABS; Sparrow, Cicchetti & Balla, 2005). Currently ongoing research is using the most up-to-date version to assess the emergence of relational responding with typically developing children and children with autism in order to correlate performance on this protocol with level of functioning as assessed using standardized measures of language and cognition (e.g., PLS-4; Zimmerman, Steiner & Pond, 2002) as well as to gain some insight into the hierarchical structuring and other features of the protocol to aid its further development and refinement. For access to the TARPA and the TARPA manual, please email Siri Ming at [email protected]
REFERENCES
- Lipkens, R., Hayes, S.C., & Hayes, L.J. (1993). Longitudinal study of the development of derived relations in an infant. Journal of Experimental Child Psychology, 56, 201-239.
- Luciano, C., Gomez Becerra, I. & Rodriguez Valverde, M. (2007). The role of multiple- exemplar training and naming in establishing derived equivalence in an infant. Journal of the Experimental Analysis of Behavior, 87, 349-365.
- Malott, R. W. (2003). Behavior analysis and linguistic productivity. Analysis of Verbal Behavior, 19, 11-18.
- Murphy, C. & Barnes-Holmes, D. (2009). Derived more-less relational mands in children diagnosed with autism. Journal of Applied Behavior Analysis, 42, 253–268.
- Rehfeldt, R. A., Dillen, J. E., Ziomek, M. M., & Kowalchuk, R. E. (2007). Assessing relational learning deficits in perspective-taking in children with high functioning autism spectrum disorder. The Psychological Record, 57, 23-47.
- Sparrow S. S., Cicchetti D.V & Balla D. A. (2005). Vineland II Adaptive Behavior Scales. (2nd ed.) American Guidance Service, Inc., Circle Pines, MN.
- Zimmerman, I. L., Steiner, V. G., & Pond, R. E. (2002). Preschool language scale-4. San Antonio, TX: Harcourt Assessment.
Training relational operants
Training relational operantsBelow and attached includes a listserv discussion on training relational operants.
THIS IS A DISCUSSION FROM A POST BY DARIN CAIRNS ON THE RFT LISTSERVE (I HAVE ATTACHED IT AS A WORD DOCUMENT AS WELL IN CASE THE FORMATTING IS TOUGH TO READ HERE.)
Hi there all I’m currently putting a curriculum together for working with children with Autism and have been getting remarkable success using exemplar based relational frame procedures.
Currently we are;
1) Using exemplar training (altering certain elements to highlight distinctions etc and using familiar labels etc – eg for Dad we’ll use child’s Dad’s name first then moving to less familiar names)
2) targeting specific frames - mainly hierarchical and didactic
3) using specified entailment and transformation of functions as performance goals
4) Using mastery criteria is still hard to pin but functionality is the goal anyway so we’re using RESA(A); Retention, Endurance, Stability and Application (we view the Entailment as Adductions) – for those familiar this from the Precision Teaching guys (sans the response rate at this stage – but very soon will have that).
We are messing around with prompting strats, errorless learning preparations, different ways to present the exemplars to vary the ease of acquisition of the response and then moving to framing (not sure if this is right as over selectivity may actually be enhanced and framing hindered), also looking at how to present exemplars in different orders to make the relational aspect more apparent etc etc etc….
My questions for the list are;
a) Other than coordination which seems to have to come first; do people have any thoughts on the order frames should be taught in?
b) Has anyone studied how one frame impacts upon another frame?
c) Is anyone aware of what sort of exemplars are better for teaching relational frames
d) Has anyone studied how the acquisition of a set of frames (or just a specific one) facilitates a learners ability to move through a curriculum or other tests eg how the acquisition of condionality and causality impacts on problem solving in general)
e) Has anyone studied how to ‘pull part’ relational networks (ie to identify how a person is making reasoning errors from an RFT perspective we could identify the required frames and then assess if they are functioning for the learner/performer)
Lots of questions. Any thoughts, references, ideas would be much appreciated.
All the best (and congrats on the Time article Steve – I think it will resonate with many by being presented the way it was, and engender curiosity even from those who thought it was ‘kooky’)
D
Darin Cairns
Clinical Psychologist Supervisor
Country Autism Services
Country Services Coordination
Hi Darin -- the attached three articles are relevant to questions a, b, c,
and e (nothing on d yet). Ian Stewart, John McElwee, Yvonne and I have
been looking at broadly similar issues -as those below, but in the context
of producing relevant educational software. Ian and John ran a workshop at
last year's ABA.
D.
Darin,
As Dermot mentioned in his post, myself, John McElwee, Dermot and Yvonne
put together a protocol for training up arbitarily applicable relational
responding in learning disabled children, which we've been refining for
the last year or so. This protocol is computer-based, and, drawing on a
database of electronic pictures and sounds, it allows a teacher to lead
a child through various stages which train and test mutual and
combinatorial entailment via multiple exemplars.
John and myself have been involved in workshops on Early Intensive
Behavioral Intervention and RFT the previous few ABAs and this summer
we're giving a similar one with the same theme - demonstrating to EIBI
people the effectiveness of RFT-type interventions for training language
generativity in learning disabled children. This summers workshop we'll
be discussing the extension of the original computer protocol via the
creation of a protocol that trains and tests relational pre-cursors from
simple dicriminations, through non arbitrary relational conditional
discriminations, through arbitrary relational conditional
discriminations. We'll also be discussing how this work relates to the
ABLA, and the ABLLS early learning protocols, and more specifically, how
RFT predicts the type of patterns that are seen in terms of the
correlations between ABLA and stimulus equivalence and language
performance. We are currently writing a paper on the latter and applying
for funding to test specific RFT-based predictions with regard to the
difficulty of various stages of the ABLA.
Your questions are very important ones. In our RFT-based analysis of the
ABLSS curriculum we are stressing the importance of the order of
training particular frames and how particular types of frames are indeed
necessary precursors of others. For example, flexible contextual control
over same/different responding may be an important precursor of
hierarchy. If you or others are interested I can send you past ABA
workshop .ppt presentations on EIBI and RFT.
Best,
Ian.
Hey Darin;
I think the work you are doing is important. In terms of the
sequence of which frames should be taught first, I am not sure the
data is there to guide us on this issue. Thus, put on your
clinicians hat and monkey around. Choose a frame that will have the
greatest impact for the child in his or her environment. In other
words, what frames will the child's environment immediately support
and what frames, once established will be of most use for that child
to more effective participate and operate in his/her environemnt.
This is a logical exercise. But, I suspect that a) the logic will
steer you right in many cases & b) you will hit walls that will
require troubleshooting. These successes and temporary walls are
perhaps the most important bits of information for the field. Keep
us posted so the basic minded folks can help work out the issues
that will assuredly crop up.
Question: Do have non-arbitrary tasks built into your training
sequences? Whether these are absolutely necessary pre-requisites is
still uncertain. Several studies they have definitely shown to
facilitative or the development of arbitrarily applicable derived
relational responding. But I suspect when working with language
delayed indivduals non-arbitrary tasks will be particularily useful
in making the targeted relation more salient. There are a lot of
good old studies (50'-70's) showing how MET can facilitate what's
been labeled transposition. Which is, crudely put, responding in
terms of a relation and not an absolute value.
TONY;
I agree the mistakes may be very enlightening. Again, I think the
early transposition literature sheds light on the issue of these
mistakes and implicitly (not explicity because authors often
relegate these mistakes and sucesses to the realm of schemas or
language as mediator) demonstrates ways to program training
materials such as to promote derived relational responding.
I agree that errorless procedures are often times great remedies. I
found it VERY difficult, during my pilot work for my thesis that
when dealing with derived relational responding, it is very hard to
get kids ("typically developing") to "get" the target relation and
not some other absolute property of the stimulus conditions.
FINAL NOTE (I half-heartedly promise): Would it be alright if I
posted these contributions to this thread on the RFT list to the
education section of contextualpsychology.com
Hi Nick hows it going?
I think it would be fine to put this on the education list. The more ideas and insight the better.
Choose a frame that has greatest impact for the child;
1) To me Baer’s behavioural cusp concept applies here. But it’s interesting to consider how one identifies a required frame. We could do an example of cusp analysis with frames.
2) Cusps also apply to ‘bang for your buck’ in terms of what the curriculum sequence will benefit from the most. Ie the PT guys look at tool skills to promote generative learning. I wonder what the ‘tool’ frames are in a given curriculum context?
Do we have non arbitrary tasks built in to help language delayed individuals target relation more salient?
1) We’re messing around with it but this is definitely something that interests me. If I’m interpreting you correctly, what I can feedback at this point is that the non-arbitrary tasks have proven the fastest road to relational framing for the learner. We kinda think of it as a sort of ‘within stimulus’ prompt as the answer lay in explicit previous learning and then we lead them to more purely relational situations where they must entail. When we don’t prep this way the children become anxious and start guessing.
2) Can you throw me some refs? Interested in the MTS examples you are referring to.
3) The issue of protecting the learner from over-selectivity pops up at this point too as the non arb stuff can play right into the hands of non relational behaviour being reinforced at the expense of relational…
Mistakes…
1) Have been fascinating to watch and have directed our approach with the learner quite a lot.
2) I wonder if IRAP procedures can be used here to give us insights into the relevant networks and construct the instructional design from there…?
3) What errorless learning strats (ie prompts) did you try in your thesis Nick? It’s a real struggle here too. Non arb being the only real strat we have (I’m wary of visuals). We have tried to conmstruct a hierarchy based on how previous learning will support the correct answer (ie non arb), not impact directly on framing (ie we use hypothetical examples), to impacting against framing relationally (Ie use examples where the entailment is logically true but experientially wrong – ie the child has to ‘trust’ the entailment not his explicit learning history)
Here’s a question. If we forget the order issue what is the process (I have avoided the word mechanism ) by which a frame effects another frame? What is necessary for a frame to ‘bump’ into another frame and then change it? This will go a long way to helping us understand generative learning and adductions I’d think. Real bang for your buck instructional designing.
D
Darin Cairns
Clinical Psychologist Supervisor
Country Services Coordination
The cusp concept looks like another way of saying “increases psychological flexibility” (“behavioral cusp” is in a frame of coordination with “increases psychological flexibility”?)
Re: “Here’s a question. If we forget the order issue what is the process (I have avoided the word mechanism ) by which a frame effects another frame? What is necessary for a frame to ‘bump’ into another frame and then change it?”
Along the lines of a comment in Ian’s earlier post, it seems to me that coordination and difference are essential for hierarchy. In broader RFT/ACT terms, once coordination and difference are established – which respectively have the most precision and the broadest scope, hierarchical relations serve to attenuate/balance precision and scope in context - and thus to increase behavioral flexibility. In other words, frames don’t bump into other frames unless/until we relate relations….relate multiple exemplars qua correspondence AND difference and you get hierarchy….
Once you get correspondence, difference, hierarchy, only then are more complex relations possible - deictic, conditional, and beyond…
Seems right
One thing
It seems to me that as soon as you have multiple frames you can
leverage training by demanding several simultaneously.
In other words, you can make them "bump into" each other
usefully
For example
Once a kid has coordination and difference, you can
a) use exclusion to train new material so that it simultaneously
strengthens frames of cooridination and differnce.
For example, saying "where's the gug-gub" in the presence of a
novel object and a ball (that is in a frame of coordination with "ball")
is a good way to have another "ball trial" AND distinguish balls and gub-gubs
AND train a frame of coordination between the novel object and "gub-gub."
b) similarly you can train using deliberate errors. Once the kid relaly knows Mommy, point to
Ma-Ma and say "there's Daddy" and pause. The kid will laugh or otherwise
indicate the error. "That right, That's not Daddy ... that's Mommy!"
You simultaneously apply a frame of coordination twice and a frame of distinction
c) similarly you can early on play with flexible contextual control.
(If Ma Ma was Da Da, where's Ma Ma?). This is cool because it simultaneously
strenghtens two instances of a FoC and a FoD, plus it makes the Crel control
more arbitrary
To do these kinds of things you need multiple frames ... and I think even in
the earliest training of FoC, it should be done along of training others frames.
it makes the relational feature more likely to be the invariant. For example,
why just train "Da Da" when you can also train "not Da Da."
Lots of discrete trail programs seem to ignore the benefits this can provide
- S
Steven C. Hayes
Right on! And... In defense of training just "da da." I think
there are two issues.
1) Thinking that way has not hit the main pipeline just yet. It is
out of the box. I do not believe that training "not da da" is in
most peoples realm of importance let alone possibility.
2) (this one may take me a while). Discrete trials are most commonly
used in the world ABA with autism. Initially, it is often difficult
to get any kind of vocal responding under stimulus control. With
some kids it is a real pain in the @** struggle.
As such, I think that a large part of the field has been or is
quite impressed by the POWER of reinforcement to train just about
behavior (yes yes not sophisticated language behavior like I am
displaying right here before your very eyes) that we just plug on to
see what else we can bring to strength. This is done, without
looking at the broader desired repertiore. Sometimes I feel that we
are engaging in a modern form of S-R psychology. Call it R-S
psychology. By the way this statement is not meant to indeminfy any
individual/s. As I have the utmost respect for the work I just
described.
Nick B
Research Failures
Research FailuresIt seems important to let the world know about RFT research failures or disconfirmations of the theory. If you have any, please add a daughter page and describe the study as well as you can to let the community know about it. If you have ideas about why it might have failed, feel free to list them. If you think that it did not work because RFT is incorrect, feel free to state that and to suggests necessary changes to the theory, both big and small.
If few pages are added, do not jump to the conclusion that there are few failures. This page is designed to invite them into the light but often researchers hold failures back.
To this date, I confess I know of no RFT failures. But if they are there, we want them to be known, and given good visibility here on the ACBS website.
Communication au symposium Pleine Conscience des 37èmes Journées Scientifiques de l'AFTCC, Paris 12 décembre 2009
Communication au symposium Pleine Conscience des 37èmes Journées Scientifiques de l'AFTCC, Paris 12 décembre 2009Étude pilote ouverte d’un groupe de psychoéducation à la pleine conscience et l’acceptation à l’intention de personnes vivant avec un trouble bipolaire.
J. GRAND (1), B. PUTOIS (2), B. SCHOENDORFF (3)
(1) Psychothérapeute libérale, Lyon
(2) Université Louis Lumière, Lyon
(3) Université Claude Bernard, Lyon
Problématique:
Conception, mise en place et évaluation d’un programme de groupe ouvert de psychoéducation à la pleine conscience et l’acceptation pour personnes bipolaires.
Méthode:
Étude pilote sous forme de groupe ouvert de psychoéducation (6 séances d’intervention et deux de suivi) au sein d’une association de personnes bipolaires à Lyon. 21 personnes ont participé, mais seulement 5 aux 4 points de mesures (7 à trois points). Du fait de la nature de groupe ouvert, le choix avait été fait de limiter les évaluations.
Seulement deux mesures ont été utilisées : le questionnaire d’Acceptation et d’Action-AAQ2 (Hayes 2004) et la « Cible des valeurs » (Lundgren 2005).
Résultats:
L’augmentation moyenne des scores AAQ n’était pas significative.
Les résultats au questionnaire de la cible des valeurs pré-post (N=7) montraient une augmentation des actions dans le domaine travail/formation (ANOVAChi² = 8,00 p=0,018; d=1,61), mais pas de différence au suivi à 6
mois (N=5). Il n’y avait pas de différence dans le domaine du soin physique personnel (sauf entre pré et mid,
N=7). Dans le domaine des relations, il y avait une différence significative (N=5) entre post et suivi à 6 mois
(p=0,04). Globalement, il y avait un effet tendanciel pré-post sur la cible des valeurs (p=0,063).
Cette intervention n’a donc pas eu d’effet sur la capacité d’acceptation des participants ni leurs actions en
direction de leurs valeurs dans le domaine des loisirs, elle n’a eu d’effet sur les actions dans le domaine des soins
personnels qu’au début de l’intervention (pré-mid), et dans le domaine du travail qu’entre le début et la fin de
l’intervention (pré-post). Ces effets n’étaient pas maintenus au suivi. Enfin, pour 5 sujets, il y avait un effet sur
les relations entre la fin du traitement et le suivi à 6 mois.
Discussion:
Cette étude pilote suggère que la forme de groupe ouvert choisie n’est pas une façon adaptée de délivrer l’ACT à
une population bipolaire. Nous avons tenu à faire connaître ces résultats négatifs et proposerons quelques pistes
pour une meilleure adaptation d’un traitement, qui semble donner de bons résultats dans notre pratique
individuelle chez cette population.
Research Predictions
Research PredictionsPlease add a child page describing any predictions you may have based on RFT. You should state the reasons for the prediction clearly, and be sure to leave your name.
By putting it on the page you are giving away the idea -- anyone is free to test it. However, we would ask if anyone does that, they ask the individual if they want to be acknowledged in the article that may result (not necesarily as an author, but perhaps in a footnote ... such as "The core ideas tested in this article was first suggested to us by Bessy Bluebottom, and we would like to thank her for the suggestion." Something like that.)
IRAP
IRAPSome theoretical questions and question-hypotheses concerning the IRAP and RFT:
The IRAP seems to be a measure of implicit preferences, in contrast with the explicit preferences. Explicit preferences are more influenced by social control (eg political correctness).
1. Does relational framing influence the more implicit preferences as well as the explicit? And if yes, how?
2. Can we say it’s good to be aware of our implicit preferences (as revealed by the IRAP) and make choices without bringing them into account? The implicit is good to know, to realize it’s there. But the explicit is the more important? We can learn to live our life in the direction of our explicit preferences. E.g.: ‘Muslims are terrorists’ vs ‘I want to live with all kinds of people. Not all Muslims are equal. I do respect them.’ IRAP might reveal the first relation, but the second could be more important.
3. When existing relational networks are extended with new S, will these S influence the implicit functions or the explicit or both (depending on context)?
4. when the implicit preferences and the explicit preferences are different, contextual influences are responsible for these differences? Experiential avoidance, political correctness, … If these contextual S are not present, the implicit and explicit preferences are growing more toward each other?
5. cognitive therapy is working on the explicit relations by social control? After cognitive therapy the implicit positions might stay unchanged?
6. when the social pressure is very high (IRAP on ‘Muslims are terrorists’ taken by a clearly Muslim researcher and without anonymity) even the implicit measures could be influenced? (contextual cues are stronger).
7. explicit, but perhaps also implicit preferences can reverse? E.g. the Muslim-experiment described above: when after a while the apparently-Muslim researcher says he’s anti-Muslim (eg political refugee) – after this the IRAP-scores might reverse?
Francis De Groot
RFT and Basic Social Research
RFT and Basic Social ResearchFirst, I would like to say that, from my reading of Part I. in the RFT book, it seems the overall program of research has a stable foothold within behavior analysis. This is further accentuated by the fact that applied research is beginning to appear in the Journal of Applied Behavior Analysis (see Ninness et al.)in which RFT principles are built into a computer program which teaches trigonomic functions and their graphical representations in an efficient manner. Believe me, it works...I am a co-author on the latest of these RFT/math studies, and, coming into the project, I knew pretty much nothing about functions and their graphical representations but after approx. an hour in the program as a pilot subject I had a firm grasp on the concepts...as well as many novel formulae and graphs never before seen.
Because work like this is emerging along side a strong basic research program, I think RFT is here to stay. As for its future, I have been working on a way to study meta/macrocontingencies and cultural materialism in a basic laboratory setting. This area is the domain of "cultural analysis," or "behavioral anthropology," and even crosses over into OBM. When studied behavior-analytically the phrase "culture" is really synonymous with "social behavior."
If this basic research catches on, I predict the future could see a merging of both research programs in order to study how relational framing operates in relation to social behavior. The beauty about this particular social-behavioral research program is that it begins (presumably) in a laboratory setting analogous to the most basic contexts which give rise to interlocking contingencies as they occur in nature, and as they (presumably) occurred in the evolution of cultures. So, this program would (presumably) be the most thourough, inductive, investigation of social behavior to-date. This is similar to the beginnings of the behavior-analytic research program in general: Skinner started with the most basic contexts and slowly built upon them until now, where we can study language and cognition, and do so in an inductive, non-hypothetical, manner.
Perhaps combining RFT with such research could reveal principles relevant to symbolic behavior, myths, taboos, and "norms" etc... but would do so with the precision of a basic behavioral laboratory. Other basic researchers are already hard at work developing an equation of choice behavior, perhaps a few decades will reveal equations of norms, taboos, and even a "terrorism equation." It seems pretty far-fetched, but what an exciting way to earn a living!
Shawn Boles added on 4/25/2006:
Tony Biglan has written on this as well.
Hardcover: 464 pages
Publisher: Context Press (January 1, 1995)
Language: English
ISBN: 1878978225
RFT and magical thinking in childhood
RFT and magical thinking in childhoodRFT and magical thinking: hypothesis
A hypothesis: is it possible that the period of ‘magical thinking’ in the development of children (enduring until adulthood) is depending on the development of processes central in RFT: developing of mutual entailment, literality of thoughts, reason giving and causal thinking? When children are developing those skills, but aren’t fully acquainted with them, they might more easily fall in the traps of magical thinking.
Possible test: children who are later in developing those skills, should show delayed magical thinking too (and vice versa).
Francis De Groot
Whole Lotta Predictions
Whole Lotta PredictionsI challenged the RFT list serve to come up with some good solid predictions that went beyond the several dozen in the RFT book.
This list, raw and unfiltered, is the result. Some of these ideas are great. Some seem off. And anyone was and is allowed to play. But it seemed more important to get people thinking than to get it right if "right" meant that some "leader" says "this is right."
If you have ideas, back up to the next highest level and add a child page and put yours out there!
- S
Steve Hayes
Predictions from Steve
- Responding in accordance with a coherent relational network will take less time (on average) than responding in accordance with an incoherent network (subject, of course, to the usual caveats concerning individual histories).
- Relating derived relations will produce some of the same effects that have been observed for analogical reasoning
- RFT models of semantic relations, analogy, executive function tasks, perspective-taking and the like should produce neural effects that overlap to some degree with the effects observed in the mainstream neuro-cog literature.
- Increasing the extent, flexibility, and fluency of relational frames, relational networks, relating relations, relating relational networks, the transformation of functions, and contextual control over each of these, should impact positively on a variety of standard measures of human language and cognition.
Steve posted a list of new things RFT does to the Academy of Cognitive Therapy
June 2005. The list was:
RFT:
- Provides new ways to do language training
-
Has lead to a new and increasingly empirically supported psychotherapy
(ACT) and to quite number of new psychotherapy techniques
- Suggests how to establish a sense of self in children
- Shows some of how to train children in "theory of mind"
- Gives a process account of mindfulness
- Predicts how many basic cognitive skills form
- Predicts new ways to increase openness to new learning
- Explains some of where psychological rigidity comes from
- Leads to a new model of psychopathology
- Suggests some of the core skills involves in language and its subskills such as analogy and metaphor
- Shows why existing information processing research in specific areas (e.g., analogy) is flawed and show how to correct that flaw
- Predicts new methods how to increase some intellectual abilities
- Predicts new methods for how to increase motivation verbally
- Predicts some new methods to decrease motivation verbally
- Has lead to new ways we might assess current cognitive relations
- Explains some of why cognitive fusion emerges, why it is harmful, and what to do about it
- Explains some of why experiential avoidance emerges, why it is harmful, and what to do about it
- Provides unexpected predictions about neurobiological responses to specific cognitive tasks
----------
What happens to Crel and Cfun in RFT studies when you teach folks to apply defusion during testing, and or when you teach defusion, train, and then test? I am thinking of M Dougher's recent study with > or < relations with shock. I wonder whether defusion would alter the transformation, perhaps leading subjects to not rip off the shock electrodes in the context of > relation. I wonder whether defusion would strengthen or perhaps weaken Crel and/or Cfun. My guess is that it may result in more rapid learning of Crel, but knock out Cfun. This would be cool to show. Maybe someone has done this, but if not we really should cook up some experiments along these lines.
-j forsyth
------------
1. Additional corollary hypotheses:
(A) Speed of acquisition of AARR during an REP task (i.e., number of trials needed to respond consistently correctly) will correlate significantly and inversely with verbal IQ. (can’t recall off hand if Denis O’Hora has already tested this specifically yet).
(B) This one would be a doozie to quantify and test, but it follows from RFT: Subjects presented with a novel metaphor who generate higher numbers of apt comparisons (especially in shorter amounts of time) will perform better (i.e., will respond correctly more frequently and given less training trials) in an REP task that assesses their ability to correctly derive relations after two previously trained frames are brought into coordination.
2. Additional corollary hypotheses:
(A) AARR in fully verbal subjects will fail to occur over time within an experimental context, given a consistent lack of reinforcement for AARR and/or consistent punishment of AARR within that context.
3. Additional corollary hypotheses:
(A) The same established verbal relation (e.g., A is similar to B, which is similar to C) can be shown to accompany different functional transformations across different experimental contexts.
(B) Identical functional transformations can be shown to be achieved through the training of different verbal relations.
J T
---------------
read some RFT-research on the change of psychological function of stimulus C by putting it in relation with A-B (sexual excitement, taste preference, mood). What if C is relationally framed with 2 different classes: A-B-C, and X-Y-C. And let's say A is experienced a bit negative, and X also a bit negative. Would C become experienced more negative, than when it's framed with only one class? This might be an operationalisation of multiple small life experiences leading to a larger reaction.
De Groot, Francis [[email protected]]
Suggested Readings pre-2010
Suggested Readings pre-2010Understanding RFT: A few simple articles and presentations
- Blackledge, J. T. (2003). An introduction to Relational Frame Theory: Basics and applications. The Behavior Analyst Today, 3(4), 421-433.
- Blackledge, J.T. & Moran, D.J. (2009). Introduction to relational frame theory for clinicians. Japanese version published in Kokoro no Rinsho.
- Törneke, N. & Luoma, J. (2009, July). RFT: Basic concepts and clinical implications. Paper presented at the 3rd World Conference for Contextual Behavioral Science, Enschede, Netherlands.
- Blackledge, J. T. (2009). How is RFT Relevant to Clinical Psychology? Audio and handouts from a teleconference given to the Psychotherapy Research Network in March, 2009.
The role of RFT in Contextual Behavioral Science
- Vilardaga, R., Hayes, S. C., Levin, M. E., & Muto, T. (2009). Creating a strategy for progress: A contextual behavioral science approach. The Behavior Analyst, 32, 105-133.
- Levin, M. E., & Hayes, S. C. (2009). ACT, RFT, and contextual behavioral science. In J. T. Blackledge, J. Ciarrochi, & F. P. Deane (Eds.), Acceptance and Commitment Therapy: Contemporary research and practice (pp. 1 – 40). Sydney: Australian Academic Press.
- Hayes, S. C. (2009, July). The importance of RFT to the development of contextual behavioral science. Presidential address given at the 3rd World Conference on Contextual Behavioral Science, Enschede, Netherlands.
- Cannonical Works: Looking at the Roots of CBS
Reviews & Situating RFT in the Larger Literature
- Gross, A. C., & Fox, E. J. (2009). Relational frame theory: An overview of the controversy. The Analysis of Verbal Behavior, 25, 87-98.
- Vilardaga, R. (2009, May). A systematic review of the RFT literature on deictic framing. Paper presented at the Annual Meeting of the Association of Behavior Analysis International conference, Phoenix, AZ.
ACT/RFT Reader Update
- ACT/RFT Reader Update is a review by CBS reseachers of recent research in both ACT and RFT that was published from 2018 - 2011. Each of the articles reviewed is available on this site.
Books on Applying RFT
- Rehfeldt, R. A., & Barnes-Holmes, Y. (2009). Derived relational responding: Applications for learners with autism and other developmental disabilities. Oakland, CA: New Harbinger Publications, Inc.
Derived Relational Responding offers a series of revolutionary intervention programs for applied work in human language and cognition targeted at students with autism and other developmental disabilities. It presents a program drawn from derived stimulus relations that you can use to help students of all ages acquire foundational and advanced verbal, social, and cognitive skills.
- Woods, D. W., & Kanter, J. W. (Eds.). (2007). Understanding behavior disorders: A contemporary behavioral perspective. Reno, NV: Context Press.
This volume presents a contemporary behavioral model of behavior disorders that incorporates the findings of current RFT and ACT research. Rich in possibilities for clinical work, this view of disordered behavior is an important milestone in clinical psychotherapy - an opportunity for behavioral clinicians to reintegrate their clinical practice with an experimental analysis of behavior.
- Dahl, J. C., Plumb, J. C., Stewart, I., & Lundgren, T. (2009). The Art and Science of Valuing in Psychotherapy: Helping Clients Discover, Explore, and Commit to Valued Action Using Acceptance and Commitment Therapy. Oakland, CA; New Harbinger Publications, Inc.
This book is an applied volume in purpose, but includes an RFT account of each of the ACT processes, and in particular an in depth RFT perspective on personal values and the clinical interventions employed to enhance them and promote committed action.
- Dougher, M. J. (Ed.). (2000). Clinical Behavior Analysis. Reno, NV: Context Press.
While not explicitly a volume on RFT, this book is an excellent resource on clinical behavioral approaches to common problems and includes several chapters with an RFT perspective on clinical problems.
News & Other Media
- DJ Moran's Functionally Speaking Podcast
- Does Language Influence Culture? Article from Wall Street Journal highlights the importance of language practices
Study Guides for RFT Books
Study Groups for RFT Books
Study Groups for RFT BooksLearning RFT (the book) Study Group - Winter 2010/2011
Learning RFT (the book) Study Group - Winter 2010/2011

 Interest in Niklas Torneke's new book Learning RFT has spawned a discussion group on the listservs.
Interest in Niklas Torneke's new book Learning RFT has spawned a discussion group on the listservs.
Here, Joe Parsons has generously supplied a Powerpoint for getting folks started on Chapter 1.
You'll need to be logged into your current, paid ACBS member account to view/download it. (Can't remember if your membership is current? Login then click on "Dashboard" on the right, then see your membership expiration date on the right side of the screen.)
Relational Frame Theory (the book) Study Group for Beginners - 2006
Relational Frame Theory (the book) Study Group for Beginners - 2006PLEASE NOTE: This study group is not longer running, but we have left the information gathered here for your perusal. You may find the information in these pages of some use to you. Also, you may consider starting your own study group by asking colleagues and others on the listservs of their interests and then using these pages or asking ACBS staff to help you update them for your current purposes.
This is a place for people who are perhaps not behaviourally trained to learn RFT. We are primarily a group of clinicians and others who have been drawn to RFT through our exposure to ACT. Together, with each other's help, we are walking through the Relational Frame Theory: A Post-Skinnerian account of human language and cognition book chapter by chapter and discussing both our understandings and our struggles. Please join in if you like. Beginning June 2006, our plan is to read one chapter a month, commenting on it as we go. We are particularly open to people who may know more than we do. So if you read something here that seems as if we're barking up the wrong conceptual tree, please, don't hold back. For those who are participating, let's try to remember that the only stupid question is the one not asked.
There are two basic ways to contribute to our ongoing discussion: by adding child pages or by adding comments. The differences between these are described below. Child Pages Child pages are used to create entirely new web pages that are connected to a "parent" page. For example, this page that you're reading is a child page of the "About RFT" page (likewise, the "About RFT" page is the "parent page" of this page). "RFT Book Summary & Discussion" is a child page of this page. You can add a child page to any existing page by clicking on the "add child page" link at the bottom of the page. When you add a child page, several things happen:
- A new web page is created with whatever title and content you give it
- A link to your new page will be listed at the bottom of the parent page (like the link to "RFT Book Summary & Discussion" seen at the bottom of this page)
- A link to your new page will appear in the menu hierarchy on the left side of the screen (like the link to "RFT Book Summary & Discussion" seen on the left side of the screen below "RFT Study Group for Beginners"
So when should use add a child page? When you are contributing a new summary or question or discussion point. If you are just responding to something someone else has already posted, you should add a comment to their page (see below). For example, if you wanted to add a summary of Chapter 4 of the RFT book, you would go to the Chapter 4 page (RFT > About RFT > RFT Study Group for Beginners > RFT Book & Discussion > Chapter 4) and then click on the "add child page" link at the bottom of that page. A link to your summary page would then appear at the bottom of the Chapter 4 page and below Chapter 4 in the hierarchical menu on the left. Comments Unlike a child page, a comment is not a new web page. It is simply a comment added to the bottom of an existing page. Each page can have an unlimited number of comments, and users can reply to existing comments. In this way, every page can be like a whole discussion board with a primary post (the "child page" that has been added) and a discussion listed below it that consists of a series of comments. If you are just responding to something someone else has already posted, you should probably just add a comment to the page by clicking on the "add new comment" link at the bottom of that page. If you are responding to an existing comment, you can click on the "reply" link listed in the comment itself. Happy commenting, child paging, discussing, and learning!
RFT Book Summary & Discussion
RFT Book Summary & DiscussionThis section is for individuals to offer their summaries, questions, and comments about the Relational Frame Theory book.
Chapter 1
Chapter 1- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
1.3.1 Rule governed behaviour
1.3.1 Rule governed behaviour
What's hardest for me in all of this is learning the language. It's very precise, and not intuitive for me. Okay, enough whining.
Questions:
1. Autoclitic frames?
Autoclitic: a unit of verbal behaviour that depends on other verbal behaviour for its occurrence and that modifies the effects of that behaviour on the listener. (Catania)
Ex:if-then?
So in Skinner's quote on pg 15 he's pointing to relational framing as a behaviour without explicitly delineating it?
2. Language hypothesis-the idea that differences between instructed and uninstructed performances could be accounted for by human language.
...the behaviour is verbal in Skinner's approach because a specially conditioned listener mediates reinforcement of this behaviour. (p.16)
I'm still struggling with this. So, for Skinner, if a tree falls in the forest and no one hears it, it doesn't make a sound?
Another question: For Skinner, can the listener and the speaker be the same person?
How can listening not be verbal? "The role of the listener in any verbal episode was thus "not necessarily verbal in any special sense.""
I think I understand the unworkability of this definition, I just want to understand Skinner's conceptualization.
Please don't tell me I have to read Verbal Behaviour.
I'm not quite understanding Skinner's dilemma regarding a functional definition of "specifying". He cannot refer to reference. I understand that, but am not getting the inability to refer to verbal behaviour. Is this why? "(Skinner)did not distinguish between verbal rules and regularities observed in other complex antecedents." p17
thanks
Joanne
Summary of Chapter One
Summary of Chapter OneHere is my summary of chapter one. I know i am a little behind schedule :(
but would be grateful if anyone could point out any fundamental misunderstandings before i get too far with ch 2. Unfortunately the formatting of headings has disappeared but i guess that doesn't make much difference to how much sense it makes.
Chapter 1
Why a behavioural approach is a good idea.
This chapter opens by (briefly) making a case for a behavioural approach to language. It points to the progress made the behavioural approach in other areas, and to the difficulty the cognitive approach has had in stepping outside common sense assumptions (e.g. that words can be understood as representing ideas). The cognitive approach is said to provide a reasonable account within its own assumptions (i.e. that the task is to describe how words and sentences etc. are perceived, encoded, produced etc.). However, a behavioural approach may have something different and useful to offer.
The chapter continues by saying that language is, or should be, of fundamental importance to behaviour analysts, pointing out that the early focus on the behaviour of non-verbal organisms was only ever intended to be a starting place.
What sort of behavioural approach we are talking about.
The authors outline the assumptions of their particular brand of behaviour analysis, i.e. functional contextualism. This is really very simple. If you start from the goals (predict and influence) everything else follows. These goals (predict and influence) mean that the independent variables must be in the environment of the person/system/group being studied (else, obviously, the theory cannot tell you how to change the person/group/system). Hence the importance of context or environment. Also, ‘truth’ has to be what works in achieving those goals. There is no other criterion. That’s all there is to it. (??)
Why the previous attempts of behaviourists (even Skinner’s) to provide an account of language didn’t work and why this one will be better.
The next few sections of the chapter are concerned with outlining previous attempts by people working within the behavioural tradition to develop accounts of human language. Since these appear to have come unstuck in some way or other, it is important to understand what went wrong, and perhaps to explain the ways in which the current approach is different and stands a better chance of success.
The first to be considered is Kantor’s interbehavioural approach, which apparently did not generate a viable programme of research. The case is made that this is because it was based on descriptive rather than functional contextualism. In other words, the lesson is look what happens if you do not have your goals in place. (?) Some valuable and influential aspects of his work are also outlined: specifically, the importance of context and the idea that the stimulus functions of an event should be seen as part of the response to the event and that stimulus functions can be transferred from one event to another.
The chapter then looks at Skinner’s approach to language, and two attempts (those of Willard Day and Kurt Salzinger) to obtain the empirical data that would be needed to test and develop this model. The main point of this section is to argue that Skinner’s work, although an enormous step forward at the time, is not up to the job of moving us forward now. Basically if it was going to work we’d be a lot further ahead by now. The authors say that if you are happy to accept this conclusion you can skip the next few pages, but if you need to be convinced then you have to read them. I guess people who are familiar with Skinner’s Verbal Behaviour would find this section easy to follow, but I’m not and I didn’t. However the main point seems to be that there is problem with his definition of verbal behaviour: you decide whether or not a piece of behaviour is verbal by seeing how it is reinforced. If it is reinforced by someone who has been trained to reinforce it in this way by the verbal community then the behaviour is verbal. However, the behaviour of the listener/reinforcer is not itself necessarily verbal (it could be reinforced in some other way). This is a problem, because trained ‘listeners’ who deliver the reinforcement could be reinforcing all sorts of different behaviours that we wouldn’t generally consider verbal, such as the behaviour of rats in operant conditioning experiments. This makes the definition both too broad (it includes rats in operant conditioning experiments) and too narrow (it excludes the behaviour of the listener).
The research has led to RFT
The last part of the chapter outlines the work in behaviour analysis that paved the way for RFT. There are two main strands of research.
The first to be considered is research on rule-governed behaviour. Basically, instead of having to learn contingencies by trial and error you can just be told them and that way you get them much quicker, but you tend to take longer to notice if they turn out not to be what you were told they were. This would seem to be something to do with language (the “language hypothesis”). However, an account of rule-governed behaviour as verbal behaviour could not be accommodated within Skinner’s approach because a) the function of a stimulus as a rule depends on the history of the listener rather than the speaker and Skinner’s definition of verbal behaviour concerned only the speaker, and b) he could only say a rule was a discriminative stimulus which specifies a contingency, but this is inadequate (because it does not distinguish rules from other types of discriminative stimuli) unless you can specify what is meant by ‘specify’ which he was not able to do (following his own rules).
The second is derived relational responding. This section starts by outlining a famous paper by Sidman (1971) in which he reports that a person (child?) with learning difficulties who had been taught to match spoken words to pictures and separately taught to match the same set of spoken words to printed words was then able to match pictures to the corresponding printed words without actually being trained to do this. [NB I think there is an error in book near the top of page 18 in the sentence that begins, “Sidman’s (1971) …”?]. Because the picture-written words relationships had not been trained they are called derived. The next paragraph summarises how equivalence relations were studied using matching to sample procedures. If, having learnt that selecting X from X, Y and Z is correct in the presence of A, A is then selected from an array from stimuli such as A, B and C in the presence of X, then this is said to show symmetry. Further, if having learnt that selecting X is correct in the presence of A, and selecting P is correct in the presence of X, when then presented with an array of say P, Q and R in the presence of A, you pick P, well then that shows transitivity.
This was exciting because it seems very like language (e.g. the relationships between words and things are symmetrical). It was also puzzling because this symmetry does not generally apply in other situations, and the example of approaching thicket in the presence of a lion, but not a lion in the presence of a thicket is given.
The chapter ends by claiming that taking this idea of derived relational responding further (in the next chapters) leads to a more adequate definition of verbal behaviour, allows rule-governed behaviour to be understood as verbal, and lays the ground for a ‘vibrant research agenda’.
Thanks,
Janet
questions on 1.1.3 and 1.2.1
questions on 1.1.3 and 1.2.1Okay, help. Can someone give me a real life example that will help me distinguish a mand from a tact?
Tact: A verbal operant in which a response (from the person emitting the operant or from the environment) of a given form is evoked.. by a particular object or event or property of an event of an oject or event."
There is an excellent summary of the core ideas of Verbal Behavior in Kohlenberg and Tsai's 1991 FAP Book. The whole of chapter 3 is about these issues and is very interesting as is the whole book. I copy a few lines from it since they tell it much better than I could :
A tact is defined as a verbal response that is under the precise control of discriminative stimuli, and that is reinforced by generalized secondary reinforcers. For example, if you are shown a red ball and asked, "What is this?" and you say "A red ball," you would be tacting because the form of your response ("red ball") is controlled by the object and is reinforced by a conditioned generalized reinforcer such as "uh-huh," "right" or "thank you," or any of hundreds of reactions that indicate you were understood. Notice that the contingency or reinforcer is borad and general, whereas the prior discriminative stimulus (Sd) is specific. The tact is thus brought about by the presence of a particular stimulus (e.g., a red ball) and an audience (the therapist or parent). Tacts, in this sense, are similar to the notion of labels or names ( p.54)
1.1.3 Skinner's Approach p9
Mand: A verbal operant in which the response, (whose? the person emitting the operant or the environment?) is reinforced by a characteristic consequence and is therefore under the functional control of relevant conditions of deprivation or aversive stimulation.
Stil from the FAP book : Mands are the speech involved in demands, commands, requests, and questions. A mand is behavior with the following characteristics: (1) it occurs because it was followed by a particular reinforcer, (2) its strength varies with the relevant deprivation or aversive stimulation, and (3) it appears under a very broad range of discriminative stimuli. Thus, if you were to say, "I would like some water" because you were thirsty, this would be a mand because it would be reinforced by a very specific reinforcer - someone hearing you and giving you water or showing you were to get some. Your "I want some water" response would not be reinforced by a generalized secondary reinforcer such as someone saying "That's right," or "Thanks for sharing that with me," or "I understand what you said". It's strength would also vary with how water deprived you were. Your mand for water can occur in almost any setting where you are thirsty and there is another person who can hear you. (p.56)
1.2.1 The definition of verbal behavior is not functional.p12
I'm not sure I understand this sentence in the last PP on the page
The behavior is not superstitious: the contingency is non arbitrary and is produced by the rat's behaviour.
Hope this is correct behavioralese : If you give arbitrary reinforcement to a pigeon, the frequency of the behavior closely preceding the reinforcement (it could be odd !) will rise. Thus, the probability that this particular behavior will occur short before the next instance of arbitrary reinforcement will rise, so it will be reinforced again and so on. As a final result, the pigeon will in the end emit this particular behavior with a high frequency, although the behavior in itself has no effect whatsoever on the reinforcing contingency. Which is not the case in the described example : As I understand it, by pressing the lever, the rat slightly shakes the feedbag and as a result, every five presses in average, a food pellet is jarred loose. This reinforcement is not arbitrary and is produced by the rat's behavior.
Here's another one on p13.
...Leighland cited Skinners ...theorising that the restricted contingencies required for abstraction ( a highly precise form of stimulus control) could only arise from an extensive history of social mediation.
The whole next paragraph just compounds the murk.
I find it difficult too. Maybe the important thing is to understand the critic made to Skinner's VB : Making appeal to the history of the listener in order to understand the behavior of the speaker is said to be a «conceptual error» making the design of fruitful experimental strategies extraordinarily difficult.
Okay enough for now. My mind is acting up.
Joanne
So does mine
Philippe
Below is a conversation regarding these questions:
RE: 1.2.1 The Definition of verbal behavior is not functioning. (Submitted by JT Blackledge on June 7, 2006 - 8:42pm.)
Hi Joanne & all--
This can be a tough one to convey and grasp, but I'll give it a shot anyway. The issue is this: Skinner (1957) defined verbal behavior as any behavior emitted by a speaker that is reinforced through the mediation of a listener trained by a verbal community to mediate such reinforcement. In other words, a given behavior is verbal if it is reinforced by someone else who has been specifically trained by a "verbal community" to reinforce such behavior in certain ways.
From this perspective, the lever-pressing behavior of every rat & pigeon that has gone through an operant conditioning experiment is verbal, because the reinforcement they receive (often in the form of a food pellet, for example) for pressing the lever depends on the mediation of the experimenter (specifically trained by a "verbal community" to mediate such reinforcement) who programs when the machine dispenses reinforcers. An odd (but true) statement, and one that makes you wonder "why define verbal behavior in such a way that it includes the behavior of apparently 'non-verbal' organisms?"
But that's not the biggest problem with the definition--Skinner's definition of VB actually violates one of the central tenets of behaviorism: What matters is the FUNCTION of a behavior, which refers to a reliable relationship between the emission of a response and the delivery of a reinforcer. From a functional perspective, it doesn't matter what the response looks like. My good friend Pete Linnerooth describes it this way: You can walk to the fridge to get a beer, run to the fridge to get a beer, or crawl to the fridge to get a beer. Either way you get a beer. The form of the behavior doesn't matter. What holds a variety of different-looking behaviors together in the same class is their ability to receive the same kind of reinforcement--and we're interested in changing classes of behavior, not just specific instances (e.g., stop someone from running to the fridge to get a beer, and they can still walk, crawl, or swing from the rafters to get one...). From a functional perspective, it also doesn't matter how the reinforcement is delivered (e.g., if it magically drops from the Heavens, is delivered by Sue or Joe, or results from more 'natural' contingencies). What matters is that, in a given context, there is a reliable and predictable relationship between behavior and subsequent reinforcement. Hence the two examples on p. 12. If a rat gets a food pellet after pressing a lever 5 times (on average), it doesn't matter if this result is mediated by an experimenter, or if it simply occurs due to a more 'natural' set of cirucmstances (i.e., a hole in the food bag that releases a pellet after the bag is jarred every five times or so by a lever). The lever-pressing behavior will be shaped up and maintained regardless of the 'source' of the reinforcement, as long as the contingencies are relatively stable. To ascribe importance to anything other than this basic functional issue in a definition of verbal behavior doesn't make sense from a behavioral perspective, and places Skinner's definition of VB in contrast to virtually every functional definition within behavior analysis. (That being said, I still dig Skinner for the brilliant contributions he made....).
Hope this helps.
Best,
JT
JT Blackledge
Lecturer
University of Wollongong
New South Wales, Australia
The functional nature of Tacts and Mands. (Submitted by Aidan Hart on June 9, 2006 - 5:23am.)
I’m still attempting to understand many of the concepts in the RFT book and Skinners definition of verbal behaviour. So far, my contact with Skinners system has been primarily within the chapter contained within Kohlenberg and Tsai (1991).
However, it seems to me that Skinners system, (and in particular Tacts and Mands as verbal response classes) is indeed a functional one. How one distinguishes a tact from a mand is not based on the content of the verbal statement but on the function it serves. Does this not make it functional?
For example, a client recently remarked to me that they found aspects of our sessions difficult (I can’t remember the exact phrase that they used and I suppose the exact phraseology is not important). Skinners system, as explained by Kohlenberg and Tsai, provides a framework in which I can I attempt to understand the function of the clients statement.
Is the client’s verbal behaviour a Tact? If so, in this case the clients verbal behaviour is under the discriminative control of me as a therapist, the questions I might be asking (and have asked) and possibly the setting events of the therapy session itself, the clients description may then be reinforced by my response (“Yes, these are difficult things to talk about”) If the client has a history of being under assertive or does not like to admit when they are struggling, this Tact may also serve as a CRB2 and my response to them may help reinforce and build their ‘self-tacting’ and ‘tacting’ to others behaviour.
However, I also considered that the clients verbal statement may have been a Mand, albeit a disguised one. In tacting that the sessions were sometimes difficult, the client may also have been Manding that they wished to talk about something else. The client may have wanted recognition or praise for their efforts. So even though the content remains the same, the distinction between the tact and the mand in this case surely lies in the function of the verbal statement itself which itself can not be understood independent of my (and others) history of responding to such statements.
I think that there is merit in Skinners position concerning appealing to the history of the listener in order to understand the behaviour of the speaker. I think potentially what Skinner may have been arguing for here is an ‘appeal to the contingencies’. In attempting to understand the function of any verbal interaction and in particular the function of the speakers verbal behaviour we must understand the context in which the verbal behaviour has occurred. The listener is part of this context. Understanding the function of the listener in that context will indeed require an understanding of the history of the listener. If the speaker’s behaviour is under the discriminative or consequential control of the listener and the listener’s response, then we need to understand the behaviour of the listener and their history of interacting with the speaker, if we are to understand the function of the speaker’s behaviour in the first place.
In the example above, distinguishing between a tact and mand and determining the function of the mand in terms or appetitive or aversive control will require understanding our history of interaction. This requires understanding my history of responding to such descriptions or request from clients or this client in particular. Therefore understanding the clients (speakers) behaviour is surely contingent upon a functional understanding of my (the listeners) behaviour.
Just some musings.
re: the functional nature of tacts and mands. (Submitted by JT Blackledge on June 10, 2006 - 8:24pm.)
Hi Aidan--
Very clever observation, me thinks. Tacts and mands may point to functional distinctions as they can describe responses made in the presence of different discriminative stimuli which function differently (e.g., a mand is a response reinforced by the acquisition of a tangible reinforcer; a tact reinforced by attention in the form of social praise). The problem is, use of these terms doesn't add anything functionally new to the analysis given Skinner's core definition of verbal behavior. In the bar-pressing examples used in the book, for example, the rat's bar-press on a reinforcement schedule controlled by the experimenter would be considered a mand; the rat's bar-press on a reinforcement schedule controlled by the 'hole in the feed bag' would simply be a response made in the presence of a discriminative stimulus (or SD) which functions to acquire a tangible reinforcer. But either way, the SD (in this case, say the bar or lever) functions exactly the same way (to elicit a bar-pressing response) and exactly the same schedule of reinforcement results. In other words, describing the rat's behavior as verbal or non-verbal adds nothing functionally useful to the analysis--the rat will continue to respond as generally expected for a rat receiving food pellets on a VI5 schedule, and no new terms based on the learning history of the listener or experimenter need be forwarded. In fact, by implying that the learning history of the listener/experimenter needs to be taken into account in order to determine 'what kind of behavior' the rat is engaging in, Skinner (perhaps inadvertantly) departed from a core focus in behavior analysis: It is the learning history of the individual under analysis, and how this history ascribes differential functions to current contexts, that is solely of interest. Plus, the way Skinner defined VB turned out not to address the differences in responding so far empirically observed between humans and non-humans (the fact that we can talk about a rat emitting verbal behavior using Skinner's definition points to part of the problem).
Stimulus equivalence theory and RFT manage to draw functionally useful distinctions between verbal and non-verbal behavior, distinctions that have repeatedly held up under empirical scrutiny. RFT in particular draws the dividing line between VB and non-VB solely at a process level (i.e., derived relational responding in the case of verbal behavior; operant behavior based on direct contingencies and generalization in the case of non-verbal behavior) that can be witnessed by focusing solely on the learning history of the individual under analysis.
And virtually all of this particular thread of the discussion is probably unimportant to those of you simply trying to understand RFT better. I think it only really becomes important when you are trying to sort through different behavioral accounts of verbal behavior and determine which one has a better smell to it.
Fun stuff, anyway.
Best,
JT
The role of the listener. (Submitted by Jacqueline A-Tjak on June 14, 2006 - 1:54am.)
Hi Aidan and all,
John and Francis are right: we do not need to understand Skinners view on VB or the corrections RFT made to understand the RFT stuff. Still there is some fun in it and I sure am glad with the questions asked, all the comments, examples and definitions that were given by others (on another childpage).
The role of the listener, Aidan, seems very important to me too. And he would not have his role as listener if he did not have a history of learning to respond/reinforce the words of the speaker.
But as I get it, focussing on the history of the listener brings about so many problems that verbal behavior cannot be studied in a way that helps us to understand human behavior better. John explained some of these problems. So RFT changed the definition of verbal behavior. This does not mean that studying the role of the listener suddenly does not seem important at all any more. It is just not a part of the definition any more.
Still, I do think you are very right that it is the interaction that 'needs' to be studied: behavior in context. The listener is (part of the) context for the speaker. The listeners behavior (which has a history) can be reinforcing for the speaker. The listeners behavior can now be seen as verbal behavior and the listener can now be seen as a speaker and the speaker as a listener, who reinforces the respons of the speaker who was a listener at first etc. Which is a complicated way to say that therapist and client mutually influence each others behavior.
Jacqueline
The role of the listener. (Submitted by Marco Kleen on June 14, 2006 - 4:16am.)
Hi everybody,
I think you hit an important point here, Jacqueline. The clinical implications of mutual influence of speakers and listeners are huge. This subject is very related to things like therapeutic relation, motivation, 'nonspecific variables' and so on. Just focussing on the intrapsychological processes would mean ignoring the role of the listener (and observer in experiments) as important contextual factor for the speaker.
A question: does that mean that the only thing a therapist can theoretically do is influencing the context because he's nothing more than a (relevant) contexual factor, or are there more theoretical possibilities?
Marco
The role of the listener. (Submitted by JT Blackledge on June 14, 2006 - 9:18pm.)
Hi Marco--
The issue you mention (the mutual influence of therapists and clients) is critically important--I wholeheartedly agree that we can and should monitor both therapist and client behavior, and that we should be interested in monitoring how therapist and client interact and in changing the behaviors of both parties for the better. And the function issue as it relates to verbal behavior is actually a different issue than that. The behavioral assumption is that stimuli take on different functions for an individual solely because of the learning history of the individual. When I'm interacting with a client in therapy, whatever I do functions in specific ways for the client solely because of the learning history of the client. Once we've started interacting, the client's interactions with me become part of his learning history--but it's still solely his learning history (intersecting with current context) that determines functions of stimuli in his environment, and thus determines his behavior. And certainly, many of the stimuli 'presented' to the client by me will be dependent on my learning history as the therapist. But the functions those stimuli take on for the client still depend entirely on the interaction between the client's learning history and the current context (not on ontological claim--just a pragmatic one). In other words, it's the client or speaker's learning history--not the therapist or listener's learning history--that determines what functions stimuli take on for the speaker from moment to moment.
The biggest take-home message from chapter 1, I think, is that it sets up the notion that RFT adds a clear description of how verbal behavior allows stimuli to take on different functions for an individual in a way (through derived relational responding) that's a bit different from non-verbal processes like direct contingency operant conditioning. That's one critically important thing RFT does that Skinner's analysis doesn't (Skinner assumed that verbal behavior and nonverbal behavior lead to stimuli taking on functions in the same ways). The second thing is that RFT does this without stating that we have to focus on the learning histories of both the client (e.g., the speaker) and the therapist (e.g., the listener) simultaneously in order to determine what function a given stimulus has for the client/speaker. It's the speaker's learning history that determines how a stimulus (even a stimulus provided by a "listener") functions for the speaker at any given moment--not the listener's learning history.
Anyway, fun to talk about.
Best,
JT
Mands and Tacts. (Submitted by JKesselring on June 7, 2006 - 4:20am.)
I'll have a go at the mand vs tact distinction. Consider this example: Bill and Joe are walking together down a street when they see a mutual acquantance ahead of them. Joe says to Bill, "What's that guys name?" and Bill replies "Jack". In this case the specific form of Bill's response (saying "Jack")was controlled by the specific properties of the stimulus (the guy calls himself Jack). This is a tact. [Joes question is a mand that sets the occasion for Bills response, but lets not worry about that now.]
Since Bill and Joe walk faster than Jack they gradually catch up to him. When they get a few feet behind him Bill says "Jack" which leads Jack to stop, turn toward them, and start to interact. In this situation a response with the same (or similar) formal characteristics as in the tact example (saying "Jack") has different functional characteristics. This is a mand since Bill said it "to get Jacks attention." Or to put it more behaviorally, he responded this way because in the past he has been reinforced by social interaction in similar contexts when he has said a person's name.
Another example: Joe says to his friend, Moe, who just baked a cake, "That cake looks tasty." This response would probably be a tact in the case where Joe has eaten a big meal and is throughly satiated. He is describing stimulus characteristics of the cake because in the past describing positive characteristics of the food that Moe prepares has been reinforced in various ways.
On the other hand, Joe's verbalization would be a mand in the case where he is food deprived and statements of this type in Moe's presence have been reinforced by food in the past. In this case Joe is says it because in similar contexts he has a history of being given a piece of the food after making positive remarks about the food.
Nontechnically speaking, the same words might be a compliment or a request for food (or both). (If his words did function as a request for food some would call them a "disguised mand" since they formally sound like a tact -- i.e., like a statement). The definition of a tact emphasizes the form of the response being controlled by of the properties of a contextual stimulus (in this case the cake or features of the cake), while the definition of the mand emphasizes the characteristics of the reinforcing stimulus relative to a deprivation condition (or other establishing operation).
I hope I didn't further confuse things.
John Kesselring
Mands. (Submitted by samtully on June 6, 2006 - 10:00pm.)
Correct me if I am wrong. I understand mands to be behavior, as outlined by Phillippe, though not limited to speech. i.e. if I wave at my friend to get him to come over this would be a mand. When a baby cries for food, this would be a mand. If a child spits to get attention, this is a mand. And of course, textual mands as well as sign language.
Cheers!
Shelly
Chapter 2
Chapter 2- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
C func equation, page 33
C func equation, page 33I have read and reread (and reread again!) chapter 2 over the past month, and find it much denser even than chapter 1. The concept I get hung up on over and over is the notion of arbitrary applicability (AA). While I know that AA is defined as a relationship that depends on social whim or consensus instead of formal characteristics of the stimulus, I think I’m missing the implications.
If we look at the equation for Cfunc as expressed on page 33, there’s a sentence that follows that says: “[w]e can say it this way: given arbitrarily applicable stimulus relations between A, B, and C, and given a context that actualizes the transformation of a given function of A, the functions of B and C will be modified in terms of the underlying relations between A, B, and C.”
I’d like to substitute examples for “A, B, and C”—could someone tell me if I’m on the right track with this?
An example of an actualizing context would be people talking to each other, having a conversation.
In that context, A might be a banana (the fruit itself, not the word).
One person could say, “Have you ever noticed how her nose [B, in my example?] looks like a banana [the oral word for the fruit, C in my example?]?”
Now, this comparison relies on both people’s previous experience with bananas. If the person responded “What’s a banana?” the first person would have to whip out a banana, or at least a picture of a banana, for purposes of comparison.
If this is right so far, one question would be, does one of the 3 items in the relation have to be something with material existence, not “just” a word? I think the answer to this is “no” because what if my characters were talking about something abstract?
So . . .
One person might say, “Love [A] is blind [B].”
Would C in this example be the quality of not being sighted, of blindness?
I’m getting tangled up here. Help!
Response Submitted
Funcky Cstuff. (Submitted by Jacqueline A-Tjak on August 1, 2006 - 2:55am.)
Hi Leslie,
I hope I do this right and this message will appear as an reply to your post.
The example you give of nose and banana seems right to me. The function: 'bended' tranfers/transforms from the actual banana to the nose (word).
Now the second example. Here is a 'simple' way to look at this: I do not know whether you need the third part (C). Transfer of function can happen too when it is about two relata, A en B, Love and blindness. There would be a transfer of the function: not seeing properly from the word blind to the word love.
Now lets make it more complicated:
The word blind refers to actually being blind or seeing someone that is blind (modeling). You could understand the sentence 'love is blind' without ever having seen that, just by hearing people tell about it.
With 'love' its even more complicated, because that is an even more complex experience.
Your question was: does one of the 3 items in the relation have to be something with material existence, not “just” a word.
The answer, as far as I understand it, is no, but....Somewhere in the learning history has to be direct experience. If you take the example of numbers: They are abstract, but we learn them by counting actual things. So your example would not be about three relata, but maybe thirty relata that add up to 'love is blind'. And one or more of these relata would be derived from experience.
And I think it would be far to complicated to try and figure out what relata you need to get at 'love is blind'.
So for the sake of understanding the matter maybe it is easier and enough to stay with the two relata.
Well, I hope this makes sense and it is a good test to see if I get what RFTstuff is about.
Jacqueline
Pg 30 mutual entailment and transformation / transfer of stimulus function
Pg 30 mutual entailment and transformation / transfer of stimulus functionOn page 30, first full paragraph, there is a description of a natural language event--someone names a ball to a child. It's being used to illustrate mutual entailment. But it seems that the last sentence "the r response in other words, will involve responding to the sound "ball" in terms of the previously experienced functions of actual balls." So that seems to be a description of the transfer of stimulus functions.
Is transfer of stimulus function a more precise term than transformation of stimulus function. Is transfer of stimulus function a subset of transformation of stimulus function that applies with frames of coordination or is it a different thing altogether?
Joanne Steinwachs
Leslie Telfer
Response to initial post-
Just go on reading... (Submitted by Philippe Vuille on August 5, 2006 - 9:28am.)
The response to your question is to be found on pages 31-32 :
«Equivalence research has repeatedly revealed that stimulus functions commonly transfer through the members of equivalence classes.»
Consider the classical example given by Catania (Learning, 4th ed. p. 154) :
«A child has learned to obey a parent's words, go and stop, when crossing with the parent at a traffic intersection. In a separate setting, the child is taught that go and green traffic lights are equivalent and that stop and red traffic lights are equivalent (in other words, go and green become members of one equivalence class and stop and red become members of another). If the discriminative functions of the words go and stop transfer to the respective traffic lights, the child will obey the traffic lights without any additional instruction.»
RFT is not only about equivalence or "coordination frames". In the case of frames such as opposition, the stimulus functions will not be merely transferred but transformed, as is shown in the example on page 32 :
«(...) Suppose a person is trained to selext stimulus B as the "opposite" of stimulus A. Now suppose that A is given a conditioned punishing function, such as by pairing it with a loss of points. It might be predicted that B would then have reinforcing functions (without having that function directly trained), by virtue of its "opposite" relation to the punishing A stimulus (...) It hardly seems right to say that the reinforcing effects "transferred" in such a case, because they were acquired indirectly through the relation of opposition between B and a punisher. It seems more proper to use the term transformation than transfer, and it is for this reason that RFT has adopted transformation of stimulus functions as the general term for this effect. We will still use the term transfer of stimulus functions, but will generally reserve it for situations in which the underlying relation leads to derived functions that are similar to those that were trained or that pre-existed.»
Philippe
Some questions
Some questionsHi all,
Here are some questions I have after reading chapter 2.
1. In paragraph 2.1.1 (page 22/24) is explained what overarching purely functional operants are. Could one say that 'avoidance' is an overarching purely functional operant?
2. Does anyone know what 'self-discrimination functions' are? They are mentioned on page 32 in a paragraph about tranformation of stimulusfunctions (2.2.3)as an example of stimulusfunctions that have been shown to transfer.
As a whole, I still find the concept of stimulusfunctions very difficult to grasp. What I find especially difficult is to find good examples and to specify stimulusfunctions that are involved when looking at a real life example. Anyone who can help out here with examples?
3. In paragraph 2.4 families of relational frames are summed up (page 35-39). If I get it right the phrase: 'snakes are dangerous' means NOT that the snakes are in a relation of coordination, which should be understood as equivalence, but in a relation of hierarchie, like the phrase: John is an man. Snakes are a part of dangerous stuff. Is this right?
4. Am I right that stimulusfunctions can be relata?
Jacqueline
A discussion of this chapter is included below:
re: Some questions. (Submitted by JT Blackledge on September 4, 2006 - 11:02pm.)
Hi Jacqueline--
Good questions--I've inserted some answers below.
1. In paragraph 2.1.1 (page 22/24) is explained what overarching purely functional operants are. Could one say that 'avoidance' is an overarching purely functional operant?
I think it would be slightly more technically correct to term avoidance behaviors as members of the same functional class--as avoidance behaviors have over the relatively long history of behavior analysis. Reserving the word 'overarching' for language (for example) allows the term to illustrate how operants can be grouped together even if these operants involve different functions.
(this answer might make more sense after reading the answer to 2, below).
2. Does anyone know what 'self-discrimination functions' are? They are mentioned on page 32 in a paragraph about tranformation of stimulusfunctions (2.2.3)as an example of stimulusfunctions that have been shown to transfer.
As a whole, I still find the concept of stimulusfunctions very difficult to grasp. What I find especially difficult is to find good examples and to specify stimulusfunctions that are involved when looking at a real life example. Anyone who can help out here with examples?
A stimulus function essentially refers to three things: the stimulus itself, the response made with respect to it, and the [punishing or reinforcing] consequence received for making that response. For example, you could say that a stimulus (e.g., a snake) serves an avoidance function if the presentation of a snake leads a subject to run away, and this 'running away' response is negatively reinforced by the 'removal' of the snake. Or, you could say that a child screaming serves an attention function if the screaming--made in response to an adult previously ignoring him--results in the adult positively reinforcing the child by attending to him. Finally, a 'self-discrimination function' might be evident if the verbal stimulus "Where are you, Jacqueline?" resulted in you responding "I'm right here", which in turn resulted in me positively reinforcing you. Essentially then, a "stimulus function" refers to a stimulus, a response made to that stimulus, and a consequence for that response. The 'whole behavioral unit', so to speak.
I've noticed the term "stimulus function" used more loosely & informally. For example, one might say that film of a combat scene serves an "emotive function", which would imply that the stimulus (the film) makes the viewer feel a certain way. Or, the term 'experiential avoidance' might be used to describe an attempt to avoid an unpleasant feeling that doesn't 'succeed' (i.e., doesn't yield negative reinforcment by immediate termination of the unpleasant feeling). Not entirely technically correct usage, as instances like this don't specify the consequence to the response-- though it does describe, in varying detail, the topographical nature of the response.
3. In paragraph 2.4 families of relational frames are summed up (page 35-39). If I get it right the phrase: 'snakes are dangerous' means NOT that the snakes are in a relation of coordination, which should be understood as equivalence, but in a relation of hierarchie, like the phrase: John is an man. Snakes are a part of dangerous stuff. Is this right?
Correct. The critical thing to think about when deciding if two stimuli are in a hierarchical relation vs. a relation of coordination is this: Does 'reversing' the relation make sense? If it's a coordinative relation, it will make logical sense without changing the relational term (e.g., changing "noir is black" to "black is noir" makes sense, as does changing "pictures are snapshots" to "snapshots are pictures"). If it's a hierarchical relation, it won't make sense: changing either "snakes are dangerous" to "dangerous are snakes" or "dogs are mammals" to "mammals are dogs" doesn't work, since in each case, one of the relata are members of a larger class and do not exclusively or exhaustively define the class.
4. Am I right that stimulusfunctions can be relata?
I think they would be more technically referred to as stimuli, but this relates to your question #2. Within behavior analysis, a "stimulus function" refers to a stimulus, the response made with respect to that stimulus, and the consequence that follows. If you think of relata as stimuli, and grant that (within behavior analysis) stimuli are typically only talked about if they have a function (why include a stimulus in a functional analysis unless it affects subsequent behavior?), then it follows that, for practical purposes, every stimulus has a function--and that any relata included in a meaningful functional analysis are thus not only stimuli, but also partipate in stimulus functions.
Best,
JT
JT Blackledge
Lecturer
University of Wollongong
New South Wales, Australia
(Inevitably) some more questions. (Submitted by Jacqueline A-Tjak on September 5, 2006 - 7:09am.)
Hi JT
Thank you do much. Your answers made things more clear to me. And led to more questions.
In chapter one it is metioned that 'stimulusfunctions could be substitutive, no longer requiring the presence of a stimulusobject' (page 8. This is why I thought stimulusfunctions can be relata or stimuli on their own right. After reading your postand thinking it over I now come to the conclusion that there must be some kind of stimulus, non-verbal or verbal that 'contains' the stimulusfuntion and stimulusfunctions do not exist in a void. Do I understand this properly this way?
And do you mean to say that self-discrimination functions mean that a person discriminates himself in a way?
Now, you put stimulusfunctions in a frame of operant conditioning, if I may put it this way. But on page 31 the RFT book says that elicited conditioned emotional responses have been proven to be stimulusfunctions that transfer. Do you think/know, does this mean that these responses must be understood in a operant context, for instance that they are functioning as a discriminative stimulus? Or do stimulusfunctions also operate in a classical conditioning way?
You write:
I've noticed the term "stimulus function" used more loosely & informally. For example, one might say that film of a combat scene serves an "emotive function", which would imply that the stimulus (the film) makes the viewer feel a certain way. Or, the term 'experiential avoidance' might be used to describe an attempt to avoid an unpleasant feeling that doesn't 'succeed' (i.e., doesn't yield negative reinforcment by immediate termination of the unpleasant feeling). Not entirely technically correct usage, as instances like this don't specify the consequence to the response-- though it does describe, in varying detail, the topographical nature of the response.
Now what you write makes me think we should not view stimulusfunctions as something that happens in a classical conditioning situation, since there are no consequences in purely classical conditioning. I am not sure if you can, in ordinary life (as opposed to the laboratory) divide operant and classical conditioning, but I would like to make sure that I understand it correctly, if that is possible.
Lastly, you answered me that avoidance should be seen as a functional class, not an overarching operant. I am afraid that I do not understand why it is the first AND not the latter.
Thanks for having taken the trouble to clear things up for me and I hope you or somebody else can help me out with these new questions.
Best wishes
Jacqueline
RE: additional questions. (Submitted by JT Blackledge on September 5, 2006 - 9:14pm.)
Hi Jacqueline--
I've inserted answers below in ALL CAPS.
In chapter one it is metioned that 'stimulusfunctions could be substitutive, no longer requiring the presence of a stimulusobject' (page 8. This is why I thought stimulusfunctions can be relata or stimuli on their own right. After reading your postand thinking it over I now come to the conclusion that there must be some kind of stimulus, non-verbal or verbal that 'contains' the stimulusfuntion and stimulusfunctions do not exist in a void. Do I understand this properly this way?
YES--I CAN DEFINITELY SEE HOW THAT SENTENCE IS MISLEADING. THE 'UNWRITTEN SUBTEXT' THERE IS THAT THE STIMULUS IS NOW NOT AN ACTUAL LIGHT, BUT A VERBAL STIMULUS LIKE "IMAGINE A LAMP SITTING IN FRONT OF YOU". THE SENTENCE MIGHT MORE ACCURATELY READ "STIMULUS FUNCTIONS COULD BE SUBSTITUTIVE, NO LONGER REQUIRING THE PRESENCE OF THE ORIGINAL STIMULUS OBJECT".
And do you mean to say that self-discrimination functions mean that a person discriminates himself in a way?
YES
Now, you put stimulusfunctions in a frame of operant conditioning, if I may put it this way. But on page 31 the RFT book says that elicited conditioned emotional responses have been proven to be stimulusfunctions that transfer. Do you think/know, does this mean that these responses must be understood in a operant context, for instance that they are functioning as a discriminative stimulus? Or do stimulusfunctions also operate in a classical conditioning way?
You write:
I've noticed the term "stimulus function" used more loosely & informally. For example, one might say that film of a combat scene serves an "emotive function", which would imply that the stimulus (the film) makes the viewer feel a certain way. Or, the term 'experiential avoidance' might be used to describe an attempt to avoid an unpleasant feeling that doesn't 'succeed' (i.e., doesn't yield negative reinforcment by immediate termination of the unpleasant feeling). Not entirely technically correct usage, as instances like this don't specify the consequence to the response-- though it does describe, in varying detail, the topographical nature of the response.
Now what you write makes me think we should not view stimulusfunctions as something that happens in a classical conditioning situation, since there are no consequences in purely classical conditioning. I am not sure if you can, in ordinary life (as opposed to the laboratory) divide operant and classical conditioning, but I would like to make sure that I understand it correctly, if that is possible.
VERY NICE CATCH OF A VERY FINE-GRAINED POINT. THINK OF IT THIS WAY: A GIVEN STIMULUS CAN TAKE ON DIFFERENT FUNCTIONS DUE TO VARIOUS PROCESSES--CLASSICAL CONDITIONING, OPERANT CONDITIONING, STIMULUS GENERALIZATION, DERIVED RELATIONAL RESPONDING. ONCE A STIMULUS HAS A FUNCTION, REGARDLESS OF THE PROCESS(ES) INVOLVED IN TAKING ON THAT FUNCTION, THAT FUNCTION STILL TECHNICALLY REFERS TO THAT STIMULUS, THE RESPONSE THAT IS MADE TO THAT STIMULUS, AND THE CONSEQUENCE THAT FOLLOWS.
YOU'RE DEFINITELY RIGHT ABOUT THE ARBITRARY DISTINCTION BETWEEN CLASSICAL AND OPERANT CONDITIONING. INDEED, IT'S BEEN ARGUED THAT AN OPERANT CAN BE DESCRIBED IN PURELY RESPONDENT TERMS (I.E., THE DISCRIMINATIVE STIMULUS IS CLASSICALLY CONDITIONED TO THE RESPONSE, WHICH IN TURN IS CLASSICALLY CONDITIONED TO THE CONSEQUENCE). IT'S JUST THE PRACTICAL UTILITY IN DISTINGUISHING BETWEEN TWO PROCESSES THAT KEEPS THEM SEPARATE, METHINKS.
Lastly, you answered me that avoidance should be seen as a functional class, not an overarching operant. I am afraid that I do not understand why it is the first AND not the latter.
IN APPLIED BEHAVIOR ANALYSIS, IT'S COMMMON TO TALK ABOUT BEHAVIOR HAVING ONE OF FOUR FUNCTIONS: AVOIDANCE (OF AVERSIVE STIMULATION), ACQUISTION (OF TANGIBLE REINFORCERS), ATTENTION (I.E., BEHAVIOR THAT FUNCTIONS TO RECEIVE POSITIVE REINFORCEMENT IN THE FORM OF ATTENTION), AND SELF-STIMULATION. ANY BEHAVIOR, REGARDLESS OF HOW DIFFERENT THOSE BEHAVIORS LOOK, THAT SERVES ONE OF THOSE FUNCTIONS (E.,G., AN AVOIDANCE FUNCTION) FALLS INTO THAT RESPECTIVE FUNCTIONAL CATEGORY. IN OTHER WORDS, BEHAVIORS ARE GROUPED INTO FUNCTIONAL CLASSES SOLELY ACCORDING TO FUNCTION--A FUNCTIONAL CLASS, BY DEFINITION, INCLUDES A VARIETY OF STIMULUS/RESPONSES THAT ALL SERVE PRECISELY THE SAME FUNCTION.
OVERARCHING OPERANTS--LIKE MUTUAL/COMBINATIORIAL ENTAILMENT--INVOLVE PROCESSES THAT OPERATE REGARDLESS OF WHAT SUBSEQUENT FUNCTIONS RESULT. IN ANY GIVEN CASE OF COMBINATORIAL ENTAILMENT, FOR EXAMPLE, THE RESULTING FUNCTION MIGHT BE AVOIDANCE, ACQUISITION, ATTENTION, OR SELF-STIMULATION. THINK OF AN OVERARCHING OPERANT AS A PROCESS THAT ALLOWS VARIOUS FUNCTIONS TO 'ATTACH' THEMSELVES (SO TO SPEAK) TO STIMULI IN A CLEARLY SPECIFIED WAY--AND FUNCTIONAL CLASSES AS GROUPINGS OF STIMULUS/RESPONSES THAT SHARE THE SAME FUNCTION (REGARDLESS OF THE PROCESSES THROUGH WHICH THESE FUNCTIONS AROSE).
Thanks for having taken the trouble to clear things up for me and I hope you or somebody else can help me out with these new questions.
NO PROBLEM--IT STRETCHES MY BRAIN :)
Best wishes
Jacqueline
JT Blackledge
Lecturer
University of Wollongong
New South Wales, Australia
One addition. (Submitted by JT Blackledge on September 6, 2006 - 1:11am.)
Actually, you know what, the more I think about it, the more I recall that it would be correct to talk about a respondent function as including only the classically conditioned stimulus and the response made with respect to it (theoretically speaking, no consequence). That is, indeed, the 'whole behavioral unit', when speaking about a respondent, so why not?
JT Blackledge
Lecturer
University of Wollongong
New South Wales, Australia
More brainstretching exercises. (Submitted by Jacqueline A-Tjak on September 6, 2006 - 3:22am.)
Hi JT,
Thanks for clearing things for me and in the proces of doing so make me feel that I am asking questions that are worth answering. Asking these kind of questions always make me feel awkward, since my mind produces a lot of chatter in the proces.
Now if I understand everything you have written, it follows that the phrase: "one might say that film of a combat scene serves an "emotive function", which would imply that the stimulus (the film) makes the viewer feel a certain way (I quoted you here) is actually in accordance with the way stimulusfunctions work. What the speakers means/could mean is that the movie by classical conditioning or derivation has acquired a conditional emotional responsfunction. Is this correct?
Now here comes a difficult question for me to ask:
You wrote a very fine article about RFT: Blacklegde J.T. (2003) An Introduction to Relational Frame Theory: Basics and Applications. (The Behavior Analyst Today, 3, 4, 421-433). I recommend it to everyone who wants to know more about RFT. Soon I will be giving a course in ACT and tell something about RFT and your article is among the literature the coursemembers have to read.
AND..... You say in this article that Snakes and Danger are in a relation of coordinance. So, would this mean you made a mistake there?
Kind regards,
Jacqueline
re: stretching. (Submitted by JT Blackledge on September 6, 2006 - 6:22pm.)
Yes indeed--danger would stand in a hierarchical relation to snakes (not a coordinative one), wouldn't it?
JT Blackledge
Lecturer
University of Wollongong
New South Wales, Australia
Stimulus Functions. (Submitted by Jacqueline A-Tjak on September 17, 2006 - 9:21am.)
Hi all,
Still strugling with the concept of stimulusfunctions (the RFT book does not give a proper definition, does it?) I would like to know if one could say the following to be technically correct:
"Stimulusfunctions specify the nature of influence (not the intensity of it) of a certain stimulus to a certain respons". For instance, a stimulus could have a discriminative function, which would mean that it signals to a person that certain behavior has a acceptable probability to be reinforced. Since we are talking about probabilities you cannot say the stimulusfunction specifies the influence, only the nature of the influence (we are never sure beforehand this influence actually will show itself).
Jacqueline
Chapter 3
Chapter 3- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 4
Chapter 4- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 5
Chapter 5- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 6
Chapter 6- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 7
Chapter 7- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 8
Chapter 8- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 9
Chapter 9- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 10
Chapter 10- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 11
Chapter 11- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 12
Chapter 12- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Chapter 13
Chapter 13- To add a new summary, question, or discussion item, click on the add a child page link at the bottom of this page. This will create a new web page for your summary or question. It will also create a link to your new page at the bottom of this page.
- To respond to a summary, question, or discussion item someone has already posted, go to the page that contains their question or summary and click on the add new comment link at the bottom of that page. This will append your comment to the bottom of that page (it does not create a new web page). You can also reply to existing comments by clicking on the "reply" link in the comment.
Other Helpful Readings
Other Helpful ReadingsHi all,
I suggest that we use this page to post other readings so people don't have to dig through posts to find them. If it's not too much trouble, when you come across something, please post it here as well as in your original post. I'm thinking that all that we post here will be read by newcomers to ACT/RFT and I'd like to make it as easy as possible for them. It would also be useful if you'd give a few sentences on why you found it useful and what you found it useful for.
So far we've got:
Kohlenberg and Tsai (1991)
Blackledge, J. T. (2003). An introduction to Relational Frame Theory: Basics and applications. The Behavior Analyst Today, 3(4), 421-433.
Hayes, Get Out of Your Mind and Into Your Life
Hayes et al, Practical Guide to ACT
The RFT tutorial
Ciarrochi, J., Robb, H., & Godsell, C. (2005). Letting a little nonverbal air into the room: Insights from Acceptance and Commitment Therapy: Part 1: Philosophical and theoretical underpinnings. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 23, 79-106.
Any others?
Thanks,
Joanne
Learning BA to understand RFT
Learning BA to understand RFTHi all,
For those of us who aren't behaviourally trained, I've been working through this Resources in Behavior Analysis page from the Cambridge Center.
It's wonderful:
It's on the website, but I thought I'd put it here. The Skinner program on BA is helping me a lot with basic terminology.
Joanne Steinwachs
Resources for Learning RFT
Resources for Learning RFTWe recommend several ways to enhance your understanding of RFT. Great books to start with are Learning RFT: An introduction to relational frame theory and its clinical applications, or Understanding and Applying Relational Frame Theory but there are many options for you, including a great tutorial from FoxyLearning, linked below.
The RFT SIG is in the process of organizing, updating, and adding to these resources—if you have more to add, please go to the relevant area below and add them there. Please keep checking back!
Essential articles as recommended by the RFT SIG
Whether or not you intend to gain an in-depth understanding of RFT, we believe that having a basic understanding of RFT and contextual behavioral science can be invaluable for conducting clinical work. We do not believe that not having this knowledge is at all a detriment to clinical work, but we do know that when folks take the time to do so they report finding it illuminating and they simply do not think in the same way after learning about RFT.
We have compiled several resources for anyone with an interest in RFT, novice and expert alike:
- those who are interested in understanding the principles as they inform clinical practice;
- those who are interested in gaining a more in-depth understanding of the theoretical model and its research base;
- and those who are seeking formal academic training in a laboratory conducting research on RFT and its principles.
If you have an interest in discussing RFT with others who share your interests, please consider joining the RFT email listserv no matter what your background and training in RFT. The community is interested in learning and growing together and your questions may just push the community to consider new ways of approaching the work. Like the main ACT for Professionals listserv, you must be a current paid member of ACBS prior to joining.
In the child pages below you will find reading suggestions, multimedia presentations on RFT principles and how they relate to clinical phenomena, suggestions for linking up with others to learn about RFT, and information on the newly improved and highly successful RFT tutorial and how to take it.
RFT Mentor Match
RFT Mentor MatchWant to learn RFT through mentorship?
Submit an email to Patrick Smith with the subject line "RFT Mentor Match Request." Please provide some details about yourself, your familiarity with RFT, your broad interests related to RFT, your preferences regarding compensating a mentor for their time, and any other information you feel would be important for us to know for helping connect you with a mentoring opportunity that will work for you.
Want to offer mentoring?
Use the "Become a Mentor" form* linked here to submit your details and express interest in providing mentoring through our mentor match service.
*Note: Disregard the Part 1 & 3 links. This form is also used in the BiAnnual SIG survey. Those links will only work during the survey periods.
Frequently Asked Questions:
What is RFT Mentor Match?
Learning and applying Relational Frame Theory can be challenging. Much of the nuanced knowledge is not well documented. Learning through mentorship can be a very efficient way to accelerate you toward your RFT goals. The RFT Special Interest Group within ACBS represents the highest concentration of those experts. To facilitate dissemination and advancement of Relational Frame Theory, the SIG Steering Committee provides a matching service between mentors interested in working with learners and those learners. On and ongoing basis, we survey the community for members willing to mentor. When you submit a match request, we compare your request to available mentors and make introductions when we feel there is a likely valued fit.
Who Should Apply to Mentor Match?
Any learner interested in advancing their RFT goals. You may be a student, academic, professional, or even someone from outside the community who needs to get up to speed quickly.
Who are the available mentors?
Available mentors range across applied practitioner, academic faculty, and knowledgeable community members. Mentor availability changes and we want to ensure good fit between potential mentor and mentee so we don't disclose specifics. Most potential mentors have demonstrated significant contribution to the RFT community.
Will I have to pay for mentoring?
Many of our mentors provide mentoring and coaching as a professional service. Some may provide all or some of the mentor match time at no cost or a values based fee. The Mentor Match initiative does not require free work from the mentors. When mentors volunteer to be listed in the Mentor Match, their preference regarding providing paid, free, or some hybrid compensation of mentoring is part of the application. Mentee applicants will be notified of these preferences if a suitable match is identified. It is up to the mentor and mentee to agree to how the mentoring relationship will be compensated.
What are the steps of the matching process?
- Potential mentors submit their information using the "Find a Mentor" form* linked here or during the BiAnnual Survey.
- Applicant mentees submit their match request emails as described above.
- Once a match request email comes in, SIG Steering Committee members review the request and the available mentors.
- If an available mentor is a good match for the mentee, a Steering Committee member will reach out to that potential mentor to verify their availability and current interest in taking on a mentee. In the initial reach out to potential mentors, the applicant mentee ID will not be revealed to the potential mentor but some details relevant to checking match fit may be disclosed. This is why it is important for applicants to be clear and forthcoming about providing relevant information.
- If there is initial interest and availability by the potential mentor, the applicant will be provided relevant contact information for their matched mentor. At that point, applicant mentees are expected to reach out to their matched mentor. At the request of the applicant mentee, the steering committee may facilitate an introduction.
Because the goal of this program is high quality connections, we may not match applicants or potential mentors. Sincere efforts will be made to create valued matches, but matching is not guaranteed.
If you do not get matched, you are always welcome to apply again after the next round of the BiAnnual Survey.
What Mentor Match is NOT:
Mentor Match is not an employment service. Mentoring can be a very effective step toward career opportunities, but we are not placing applicants in jobs here. If you have a job opening, please share it to the RFT SIG listserve or email it to a Steering Committee Member to reshare at their discretion.
Mentor Match is not a graduate school application. Many graduate programs are built around mentoring. Some of our available mentors are also graduate faculty. Do not apply to mentor match as a substitute for an official grad school application. If you are pursuing admission into a graduate program that includes RFT, good luck. Make sure you apply through that program's official process.
Still Have Questions?
Further Questions about Mentor Match should be directed to Patrick Smith, or the current Community Engagement Steering Committee Member.
Articles Linking RFT and ACT
Articles Linking RFT and ACTThere is an extensive list of excellent articles that describe RFT in simple terms, and links the principles directly to ACT processes. We highly recommend reading some of these to further your understanding RFT and it's relation to ACT.
Please visit the page by clicking here.
Dutch language blog series
Dutch language blog seriesRichard Vanromunde has written an extensive blogseries on RFT, it's freely accessible here:
https://edotora.nl/rft-woordenboek/
From Richard:
It is in Dutch, but with Chat GPT you'll get an ok translation.
If anybody is interested in helping translate it into English, please contact Richard ([email protected]).
It's still a work in progress, but currently, you can find information about the following subjects:
Philosophy:
- Introduction in to Pepper
- Pepper's two inadequate world hypotheses
- Pepper's four adequate world hypotheses
- Eclecticism
- Functional Contextualism
What you can expect:
Philosophy:
- Dualism
- Monism
- Understanding the goal of Functional Contextualism
- Behavioral Pragmatism
- Interbehavioral field
Theory:
- Relational Responding
- Conditioning (classical and operant) as classes of Relational Responding
- (D)AARRing
- RFT
- RFT as a field
- ROE/updated RFT
RFT Tutorial
RFT Tutorial
An Introduction to Relational Frame Theory is a fully online, self-paced, interactive, multimedia tutorial designed to introduce the basic concepts and approach of Relational Frame Theory (RFT). It was developed by Dr. Eric J. Fox and first released in 2004, and has been regularly updated and maintained by FoxyLearning since 2010. An open-access version can be completed for free, a CEU version can be completed at CEUniverse to earn 7 continuing education units to maintain certification as a Board Certified Behavior Analyst (BCBA), and instructors or trainers can assign a low-cost version of the free version as a supplement to their course or training. The tutorial was written and designed for a very broad audience, and helps users to gain mastery over complex concepts in RFT by breaking them down and allowing the user to practice them along the away. It is hoped that everyone from undergraduate psychology students to doctoral-level psychologists to any educated person on the street (or on the web!) will find the material accessible, engaging, and relevant.
In 2005 the tutorial received the Nova Southeastern Award for Outstanding Practice by a Graduate Student in Instructional Design from the Design & Development division of the Association for Educational Communications & Technology. With an award name that long, you know it's got to be good.
Visit FoxyLearning to learn more!
Suggested Readings & Helpful Presentations
Suggested Readings & Helpful PresentationsThere are numerous resources for further reading. These are simply a few suggestions and you may find many others helpful. We highly recommend using this list as a starting point from which to begin your journey. We also recommend you click on this link to see a longer list of RFT/Behavior Analysis books and also to use the Publications list as an instrument for guiding your own path of learning.
Top 10 RFT Research Articles
In Spring 2023, the RFT SIG took on the task of developing an unofficial list of top RFT research articles to help people know where to start diving into the literature. The categories were “Just Getting Started” and “Contemporary and Advanced”.
Just Getting Started
- Hayes, S. C., Law, S., Assemi, K., Falletta-Cowden, N., Shamblin, M., Burleigh, K., ... & Smith, P. (2021). Relating is an operant: A fly over of 35 years of RFT research. Perspectivas em Análise do Comportamento, 12(1), 5-32.
- Cassidy, S., Roche, B., & O’Hora, D. (2010). Relational frame theory and human intelligence. European Journal of Behavior Analysis, 11(1), 37-51.
- Barnes-Holmes, D., Barnes-Holmes, Y., & Cullinan, V. (2000). Relational frame theory and Skinner’s Verbal Behavior: A possible synthesis. The Behavior Analyst, 23(1), 69-84.
- Ming, S., Moran, L., & Stewart, I. (2014). Derived relational responding and generative language: Applications and future directions for teaching individuals with autism spectrum disorders. European Journal of Behavior Analysis, 15(2), 199-224.
- Blackledge, J. T. (2003). An introduction to relational frame theory: Basics and applications. The Behavior Analyst Today, 3(4), 421.
- Stewart, I., McElwee, J., & Ming, S. (2013). Language generativity, response generalization, and derived relational responding. The Analysis of Verbal Behavior, 29(1), 137-155.
- Pelaez, M., & Monlux, K. (2018). Development of communication in infants: Implications for stimulus relations research. Perspectives on Behavior Science, 41(1), 175-188.
- McEnteggart, C. (2018). A brief tutorial on acceptance and commitment therapy as seen through the lens of derived stimulus relations. Perspectives on Behavior Science, 41(1), 215-227.
- Healy, O., Barnes‐Holmes, D., & Smeets, P. M. (2000). Derived relational responding as generalized operant behavior. Journal of the Experimental Analysis of Behavior, 74(2), 207-227.
- Stapleton, A., & McHugh, L. (2021). Healthy selfing: Theoretically optimal environments for the development of tacting and deictic relational responding. Perspectivas em Análise do Comportamento, 12(1), 125-137.
Contemporary and Advanced
- Kirsten, E. B., & Stewart, I. (2021). Assessing the development of relational framing in young children. The Psychological Record, 72(1), 221-246.
- Belisle, J., & Dixon, M. R. (2020). Relational density theory: Nonlinearity of equivalence relating examined through higher-order volumetric-mass-density. Perspectives on Behavior Science, 43(1), 259-283.
- Cummins, J., Nevejans, M., Colbert, D., & De Houwer, J. (2023). On the structure of relational responding. Journal of Contextual Behavioral Science, 27(1), 16-25.
- Barnes-Holmes, D., Barnes-Holmes, Y., & McEnteggart, C. (2020). Updating RFT (more field than frame) and its implications for process-based therapy. The Psychological Record, 70(1), 605-624.
- Hayes, L. J., & Fryling, M. J. (2019). Functional and descriptive contextualism. Journal of Contextual Behavioral Science, 14(1), 119-126.
- Foody, M., Barnes-Holmes, Y., Barnes-Holmes, D., Törneke, N., Luciano, C., Stewart, I., & McEnteggart, C. (2014). RFT for clinical use: The example of metaphor. Journal of Contextual Behavioral Science, 3(4), 305-313.
- Delabie, M., Cummins, J., Finn, M., & De Houwer, J. (2022). Differential Crel and Cfunc acquisition through stimulus pairing. Journal of Contextual Behavioral Science, 24(1), 112-119.
- Mulhern, T., Stewart, I., & McElwee, J. (2018). Facilitating relational framing of classification in young children. Journal of Contextual Behavioral Science, 8(1), 55-68.
- Kirsten, E. B., Stewart, I., & McElwee, J. (2022). Testing and training analogical relational responding in children with and without autism. The Psychological Record, 72(1), 561-583.
- Stewart, I., Barnes‐Holmes, D., Roche, B., & Smeets, P. M. (2002). A functional‐analytic model of analogy: A relational frame analysis. Journal of the Experimental Analysis of Behavior, 78(3), 375-396.
General Theory Books on RFT and Contextual Behavior Science
- Villatte, M., Villatte, J. L., & Hayes, S. C. (2019). Mastering the clinical conversation: Language as intervention. New York: The Guilford Press.
- Dahl, J., Stewart, I., Martell, C., Kaplan, J. (2014) ACT and RFT in Relationships: Helping Clients Deepen Intimacy and Maintain Healthy Commitments Using Acceptance and Commitment Therapy and Relational Frame Theory.
- Dymond, S., & Roche, B. (Eds.) (2013). Advances in relational frame theory: Research and application. New Harbinger Publications.
Törneke, N. (2010). Learning RFT: An introduction to relational frame theory and its clinical applications. Oakland, CA: New Harbinger Publications, Inc.
This book is designed to make RFT accessible to clinicians. This book is extremely readable and helps the reader understand behavioral principles, technical terms within RFT, and how to apply RFT across many different areas.
Ramnero, J., & Törneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: New Harbinger & Reno, NV: Context Press.
The ABCs of Human Behavior offers the practicing clinician a solid and practical introduction to the basics of modern behavioral psychology. The book focuses both on the classical principles of learning as well as more recent developments that explain language and cognition in behavioral and contextual terms. These principles are not just discussed in the abstract—rather the book shows how the principles of learning apply in a clinical context. Practical and easy to read, the book walks you through both common sense and clinical examples that will help you use behavioral principles to observe, explain, and influence behavior in a therapeutic setting.
Hayes, S. C., Barnes-Holmes, D., & Roche, B. (Eds.). (2001). Relational Frame Theory: A Post-Skinnerian account of human language and cognition. New York: Plenum Press.
This book may be one of the most difficult to read, but it is also the most thorough account of RFT principles and we highly recommend reading it (at some point) to gain a thorough and working understanding of RFT. Suggestion: do the RFT tutorial first. Read chapters 1 to 8, not stopping when you do not understand. Then pause and re-read Chapter 8. Then re-read the whole book and now you can stop and try to figure out what you do not understand. Don't worry. You will survive it.
Hayes, S. C. (Ed.). (1989/2004). Rule governed behavior: Cognition, contingencies, and instructional control. New York: Plenum / reprinted in 2004 by Context Press.
One of the first full-length presentations of the ACT / RFT model is in three chapters in this book on the topic. This book is now available in paperback from Context Press.
Special Issues
Conceptual Developments in Relational Frame Theory: Research and Practice. Journal of Contextual Behavioral Science.
Videos
Academic Training
Academic TrainingA number of academic training programs provide some measure of training in RFT. Go to Research Labs and click on a program or school's name to learn more about it.
ACBS Members: If you are a faculty member in an academic program that provides training in RFT, you can list your program clicking on the "research labs" link above and then "add child page" at the bottom of that page.
RFT Books
RFT BooksThere are many books to help you learn more about RFT.
RFT Listserv
RFT ListservThe RFT email listserv is a forum for scientists, scholars, practitioners, and students to discuss Relational Frame Theory (RFT), an explicitly psychological account of human language and cognition. RFT is an approach designed to be a pragmatically useful analysis of complex human behavior, providing empirical and conceptual tools to conduct an experimental analysis of substantive topics in this arena. It is based on the principles of behavior analysis and contextual behavioral science. RFT is looked to as the conceptual basis for Acceptance and Commitment Therapy, as well as an increasingly large array of other applied interventions such as language training program, or programs designed to develop a sense of self in developmentally delayed children.
The RFT listserv is open to professionals or graduate students in relevant fields. Paid ACBS membership (student or professional) is required to join the RFT Listserv.
Login to your ACBS account and click here to join the RFT listserv