Books
BooksThere are many books, audiobooks, and other materials to help you learn more about ACT, RFT, Contextual Behavioral Science, and related topics such as mindfulness and other third wave interventions.
There may seem like a lot of choices in some areas. And there are, which is a testament to how quickly the ACT/RFT/CBS work has grown.
ACT Books: General Purpose
ACT Books: General Purpose(The following list of books is from the LEARNING ACT RESOURCE GUIDE: The complete guide to resources for learning Acceptance & Commitment Therapy by Jason Luoma, Ph.D. Updated July 2020 learningact.com)
BOOKS FOR LEARNING ACT
- LEARNING ACT
- Acceptance and Commitment Therapy (Theories of Psychotherapy)
- Acceptance and Commitment Therapy, Second Edition: The Process and Practice of Mindful Change
- Acceptance and Commitment Therapy: 100 Key Points and Techniques
- Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change
- Acceptance and Commitment Therapy: Contemporary Theory Research and Practice
- Acceptance and commitment Therapy: The CBT distinctive features series
- Acceptance and Commitment Therapy For Dummies
- The ACT Approach: A Comprehensive Guide for Acceptance and Commitment Therapy
- The Act in Context: The Canonical Papers of Steven C. Hayes
- ACT in Practice: Case Conceptualization in Acceptance and Commitment Therapy
- ACT in Steps: A Transdiagnostic Manual for Learning Acceptance and Commitment Therapy
- ACT Made Simple: An Easy-To-Read Primer on Acceptance and Commitment Therapy (The New Harbinger Made Simple Series)
- The ACT Matrix: A New Approach to Building Psychological Flexibility Across Settings and Populations
- The ACT Practitioner’s Guide to the Science of Compassion: Tools for Fostering Psychological Flexibility
- ACT Questions and Answers: A Practitioner’s Guide to 150 Common Sticking Points in Acceptance and Commitment Therapy
- The Art and Science of Valuing in Psychotherapy: Helping Clients Discover, Explore, and Commit to Valued Action Using Acceptance and Commitment Therapy
- The Big Book of ACT Metaphors: A Practitioner’s Guide to Experiential Exercises and Metaphors in Acceptance and Commitment Therapy
- Interventions for Radical Change: Principles and Practice of Focused Acceptance and Commitment Therapy
- A CBT Practitioner’s Guide to ACT: How to Bridge the Gap Between Cognitive Behavioral Therapy and Acceptance and Commitment Therapy
- Committed Action in Practice: A Clinician’s Guide to Assessing, Planning, and Supporting Change in Your Client (The Context Press Mastering ACT Series)
- A Contextual Behavioral Guide to the Self: Theory and Practice
- Contextual Schema Therapy: An Integrative Approach to Personality Disorders, Emotional Dysregulation, and Interpersonal Functioning
- The Essential Guide to the ACT Matrix: A Step-by-Step Approach to Using the ACT Matrix Model in Clinical Practice Essentials of Acceptance and Commitment Therapy
- Evolution and Contextual Behavioral Science: An Integrated Framework for Understanding, Predicting, and Influencing Human Behavior
- Experiencing ACT from the Inside Out: A Self-Practice/Self-Reflection Workbook for Therapists (Self-Practice/Self-Reflection Guides for Psychotherapists)
- The Heart of ACT: Developing a Flexible, Process-Based, and Client-Centered Practice Using Acceptance and Commitment Therapy
- Innovations in Acceptance and Commitment Therapy: Clinical Advancements and Applications in ACT
- Inside This Moment: A Clinician’s Guide to Promoting Radical Change Using Acceptance and Commitment Therapy
- Introduction to ACT: Learning and Applying the Core Principles and Techniques of Acceptance and Commitment Therapy
- Learning Acceptance and Commitment Therapy: The Essential Guide to the Process and Practice of Mindful Psychiatry
- Learning ACT for Group Treatment: An Acceptance and Com-mitment Therapy Skills Training Manual for Therapists
- A Liberated Mind: How to Pivot Toward What Matters
- The Little ACT Workbook
- Metaphor in Practice: A Professional’s Guide to Using the Science of Language in Psychotherapy
- Mindfulness, Acceptance, and the Psychodynamic Evolution: Bringing Values into Treatment Planning and Enhancing Psychodynamic Work with Buddhist Psychology (The Context Press Mindfulness and Acceptance Practica Series)
- Mindfulness, Acceptance, and Positive Psychology: The Seven Foundations of Well-Being (The Context Press Mindfulness and Acceptance Practica Series)
- Mindfulness- and Acceptance-Based Behavioral Therapies in Practice (Guides to Individualized Evidence-Based Treatment)
- Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition
- Mindfulness and Acceptance in Social Work: Evidence-Based Interventions and Emerging Applications (The Context Press Mindfulness and Acceptance Practica Series)
- The Mindfulness-Informed Educator: Building Acceptance and Psychological Flexibility in Higher Education
- A Practical Guide to Acceptance and Commitment Therapy
- Talking ACT: Notes and Conversations on Acceptance and Commitment Therapy
- Values in Therapy: A Clinician’s Guide to Helping Clients Explore Values, Increase Psychological Flexibility, and Live a More Meaningful Life
- The Wiley Handbook of Contextual Behavioral Science
- ADVANCED PRACTICE IN ACT
- ACT Questions and Answers: A Practitioner’s Guide to 150 Common Sticking Points in Acceptance and Commitment Therapy
- ACT Verbatim for Depression and Anxiety: Annotated Transcripts for Learning Acceptance and Commitment Therapy
- Advanced Acceptance and Commitment Therapy: The Experienced Practitioner’s Guide to Optimizing Delivery
- Advanced Training in ACT: Mastering Key In-Session Skills for Applying Acceptance and Commitment Therapy
- Cognitive Defusion in Practice: A Clinician’s Guide to Assessing, Observing, and Supporting Change in Your Client (The Context Press Mastering ACT Series)
- Getting Unstuck in ACT: A Clinician’s Guide to Overcoming Common Obstacles in Acceptance and Commitment Therapy
- Inside This Moment: A Clinician’s Guide to Promoting Radical Change Using Acceptance and Commitment Therapy
- Learning ACT: An Acceptance and Commitment Therapy Skills Training Manual for Therapists
- Learning ACT for Group Treatment: An Acceptance and Com-mitment Therapy Skills Training Manual for Therapists
- Metaphor in Practice: A Professional’s Guide to Using the Science of Language in Psychotherapy
- Mindfulness for Two: An Acceptance and Commitment Therapy Approach to Mindfulness in Psychotherapy
ACT in Practice
ACT in Practice
Welcome to the companion website for the book!
Case conceptualization is an important part of any psychotherapeutic approach, and the ACT in Practice book helps therapists learn how to take clinically useful ideas from Acceptance and Commitment Therapy, and actually put them into practice and formulate treatments for a wide variety of clinical concerns.
The first section of the book offers an introduction to Acceptance and Commitment Therapy, an overview of the impact of ACT, and a brief introduction to the ACT's "hexaflex" model. The book also describes how to accomplish case conceptualizations in general and offers review of the literature on the importance and value of case conceptualization.
The first section closes with synopsis of the first, second, and third wave of behavior therapy with explanations of how the different waves would have treated hypothetical clients in specific situations.
The second section of the book covers ways that different ACT approaches can be applied to actual practice.
Quizzes at the end of each chapter help the reader evaluate the information they have just learned.
Please click on the links below for additional information and resources!
ACT Training and Supervision by the Authors
ACT Training and Supervision by the AuthorsPatty and D.J. have been training therapists in ACT and providing supervision in clinical behavior analysis since 2001.
If you are interested in having clinical tapes and videos reviewed for “distance supervision,” or would like to organize an ACT training workshop, we would be happy to assist you.
Please contact us for further details: [email protected]
About the Authors
About the AuthorsPatricia A. Bach, Ph.D.
Patty received her doctorate from the University of Nevada in 2000. She is an assistant professor of psychology at the Illinois Institute of Technology in Chicago, where she does ACT and RFT research and trains students of clinical psychology.
Daniel J. Moran, Ph.D., BCBA
D.J. received his doctorate in clinical and school psychology from Hofstra University in 1998. He began his training in acceptance and commitment therapy in 1994 and practices clinical behavior analysis with victims of abuse and individuals with obsessive-compulsive disorder. He is the founder of the MidAmerican Psychological Institute, and director of the Family Counseling Center, a division of Trinity Services, in Joliet, IL.
D.J. is also the host of Functionally Speaking – A 21st Century Behavior Therapy podcast. Listen here!
Case Conceptualization Worksheet
Case Conceptualization WorksheetThis “Inflexahex” model for case conceptualization can assist the clinician in charting and rating clinically relevant concerns in their clients’ lives. Dr. Patty Bach and Dr. D.J. Moran have made the ACT Case Conceptualization form available for download in pdf form, free to paid ACBS members. The form is also below for your convenience. You may select the image below and save it to your computer by right clicking on it and choosing "Save Image As".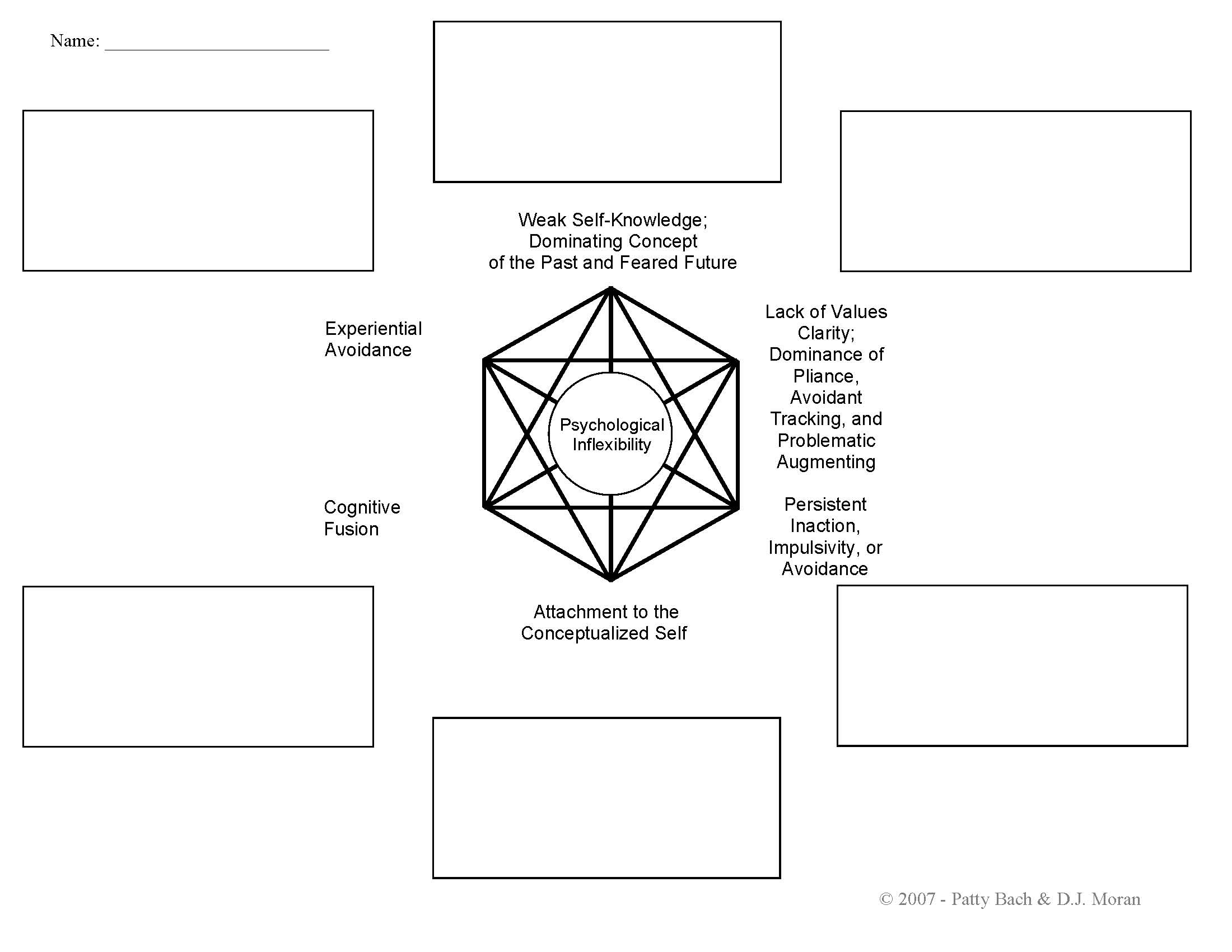
If you would like a free, full-sized pdf copy of the form and are not a paid ACBS member, please email the authors for a copy at [email protected].
ACT Books: Specific Populations
ACT Books: Specific PopulationsACT Books: Specific Populations |
(The following list of books is from the LEARNING ACT RESOURCE GUIDE: The complete guide to resources for learning Acceptance & Commitment Therapy by Jason Luoma, Ph.D. Updated July 2020 learningact.com)
- ANGER
Therapist guides
- Contextual Anger Regulation Therapy: A Mindfulness and Acceptance- Based Approach (Practical Clinical Guidebooks)
Client books
- Act on Life Not on Anger: The New Acceptance & Commitment Therapy Guide to Problem Anger
- The Moral Injury Workbook: Acceptance and Commitment Therapy Skills for Moving Beyond Shame, Anger, and Trauma to Reclaim Your Values
- ANXIETY
Therapist guides
- Acceptance and Commitment Therapy: The Ultimate Guide to Using ACT to Treat Stress, Anxiety, Depression, OCD, and More, Including Mindfulness Exercises and a Comparison with CBT and DBT
- Acceptance and Commitment Therapy for Anxiety Disorders
- Acceptance-Based Behavioral Therapy: Treating Anxiety and Related Challenges
- ACT-Informed Exposure for Anxiety: Creating Effective, Innovative, and Values-Based Exposures Using Acceptance and Commitment Therapy
- The Clinician’s Guide to Exposure Therapies for Anxiety Spectrum Disorders: Integrating Techniques and Applications from CBT, DBT, and ACT
- Trichotillomania: An ACT-Enhanced Behavior Therapy Approach Therapist Guide (Treatments That Work)
Client books
- The ACT on Anxiety Workbook
- The ACT Workbook for OCD: Mindfulness, Acceptance, and Exposure Skills to Live Well with Obsessive-Compulsive Disorder
- Anxiety Happens: 52 Ways to Find Peace of Mind
- Be Mighty: A Woman’s Guide to Liberation from Anxiety, Worry, and Stress Using Mindfulness and Acceptance
- Cognitive Behavioral Therapy: How to Use CBT to Overcome Anxiety, Depression and Intrusive Thoughts + A Guide to Acceptance and Commitment Therapy and ACT Techniques
- The Confidence Gap: A Guide to Overcoming Fear and Self-Doubt
- In This Moment: Five Steps to Transcending Stress Using Mindfulness and Neuroscience
- Living Beyond OCD Using Acceptance and Commitment Therapy: A Workbook for Adults
- The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy (2nd Edition)
- The Mindfulness and Acceptance Workbook for Social Anxiety and Shyness: Using Acceptance and Commitment Therapy to Free Yourself from Fear and Reclaim Your Life
- Outsmart Your Anxious Brain: Ten Simple Ways to Beat the Worry Trick
- Social Courage: Coping and thriving with the reality of social anxiety
- Things Might Go Terribly, Horribly Wrong: A Guide to Life Liberated from Anxiety
- Trichotillomania: An ACT-Enhanced Behavior Therapy Approach Workbook (Treatments That Work)
- The Worry Trap: How to Free Yourself from Worry & Anxiety Using Acceptance and Commitment Therapy
- CANCER
Client books
- Flying over Thunderstorms: Living Your Life with Cancer through Acceptance and Commitment Therapy
- CHILDREN/ADOLESCENTS/PARENTING
Therapist guides
- Acceptance and Commitment Therapy: The Clinician’s Guide for Supporting Parents
- Acceptance & Mindfulness Treatments for Children & Adolescents: A Practitioner’s Guide
- ACT for Adolescents: Treating Teens and Adolescents in Individual and Group Therapy
- ACT for Treating Children: The Essential Guide to Acceptance and Commitment Therapy for Kids
- Challenging Perfectionism: An Integrative Approach for Supporting Young People Using ACT, CBT and DBT
- Mindfulness and Acceptance for Counseling College Students: Theory and Practical Applications for Intervention, Prevention, and Outreach (The Context Press Mindfulness and Acceptance Practical Series)
- Teen Anxiety: A CBT and ACT Activity Resource Book for Helping Anxious Adolescents
- The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection
Client books
- Acceptance and Mindfulness Toolbox for Children and Adolescents: 75+ Worksheets & Activities for Trauma, Anxiety, Depression, Anger & More
- The ACT Workbook for Kids: Fun Activities to Help You Deal with Worry, Sadness and Anger Using Acceptance and Commitment Therapy
- The ACT Workbook for Teens with OCD
- Becoming Mum
- Dark Agents, Book One: Violet and the Trial of Trauma
- Get Out of Your Mind and Into Your Life for Teens: A Guide to Living an Extraordinary Life
- The Gifted Kids Workbook: Mindfulness Skills to Help Children Reduce Stress, Balance Emotions, and Build Confidence
- The Joy of Parenting: An Acceptance and Commitment Therapy Guide to Effective Parenting in the Early Years
- The Mental Health and Wellbeing Workout for Teens: Skills and Exercises from ACT and CBT for Healthy Thinking
- The Mindfulness and Acceptance Workbook for Teen Anxiety: Activities to Help You Overcome Fears and Worries Using Acceptance and Commitment Therapy (Instant Help Book for Teens)
- Nuna and the Fog
- Parenting a Troubled Teen: Manage Conflict and Deal with Intense Emotions Using Acceptance and Commitment Therapy
- Parenting Your Anxious Child with Mindfulness and Acceptance: A Powerful New Approach to Overcoming Fear, Panic, and Worry Using Acceptance and Commitment Therapy
- Stuff That Sucks: Accepting What You Can’t Change and Committing to What You Can
- DEPRESSION
Therapist guides
- ACT for Depression: A Clinician’s Guide to Using Acceptance & Commitment Therapy in Treating Depression
Client books
- The ACT Workbook for Depression and Shame: Overcome Thoughts of Defectiveness and Increase Well-Being Using Acceptance and Commitment Therapy
- The Mindfulness and Acceptance Workbook for Depression: Using Acceptance and Commitment Therapy to Move Through Depression and Create a Life Worth Living (2nd Edition)
- DEVELOPMENTAL DISABILITIES
- Derived Relational Responding Applications for Learners with Autism and Other Developmental Disabilities: A Progressive Guide to Change
- DIVERSE POPULATIONS
Therapist guides
- ACT for Gender Identity
- Mindfulness and Acceptance for Gender and Sexual Minorities: A Clinician’s Guide to Fostering Compassion, Connection, and Equality Using Contextual Strategies
- Mindfulness and Acceptance in Multicultural Competency: A Contextual Approach to Sociocultural Diversity in Theory and Practice (The Context Press Mindfulness and Acceptance Practica Series)
- EATING DISORDERS/BODY IMAGE
Therapist guides
- Acceptance and Commitment Therapy for Body Image Dissatisfaction: A Practitioner’s Guide to Using Mindfulness, Acceptance, and Values-Based Behavior Change Strategies
- Acceptance and Commitment Therapy for Eating Disorders: A Process-Focused Guide to Treating Anorexia and Bulimia
- A Clinician’s Guide to Acceptance-Based Approaches for Weight Concerns: The Accept Yourself! Framework
- ACT for Anorexia Nervosa: A Guide for Clinicians
- Mindfulness and Acceptance for Treating Eating Disorders and Weight Concerns: Evidence-Based Interventions
Client books
- The Anorexia Workbook: How to Accept Yourself, Heal Your Suffering, and Reclaim Your Life
- Living with Your Body and Other Things You Hate: How to Let Go of Your Struggle with Body Image Using Acceptance and Commitment Therapy
- The Diet Trap: Feed Your Psychological Needs and End the Weight Loss Struggle Using Acceptance and Commitment
- HEALTH/CHRONIC PAIN/INTEGRATED CARE
Therapist guides
- Acceptance and Commitment Therapy for Chronic Pain
- Behavioral Consultation and Primary Care: A Guide to Integrating Services
- Contextual Cognitive-Behavioral Therapy for Chronic Pain
- Mindfulness and Acceptance in Behavioral Medicine: Current Theory and Practice
- Psychological Treatment for Patients With Chronic Pain (Clinical Health Psychology)
- Real Behavior Change in Primary Care: Improving Patient Outcomes and Increasing Job Satisfaction
- Somatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy Perspectives
Client books
- Better Living With IBS: A step-by-step program to managing your symptoms so you can enjoy life to the full!
- The Diabetes Lifestyle Book
- End the Insomnia Struggle: A Step-by-Step Guide to Help You Get to Sleep and Stay Asleep
- Living Beyond Lyme: Reclaim Your Life From Lyme Disease and Chronic Illness
- Living Beyond Your Pain: Using Acceptance & Commitment Therapy to Ease Chronic Pain
- INTERPERSONAL/RELATIONSHIP ISSUES
Therapist guides
- Acceptance and Commitment Therapy for Couples: Using Mindfulness, Values, and Schema Awareness to Rebuild Relationships
- Acceptance and Commitment Therapy for Interpersonal Problems: Using Mindfulness, Acceptance, and Schema Awareness to Change Interpersonal Behaviors
- ACT and RFT in Relationships: Helping Clients Deepen Intimacy and Maintain Healthy Commitments Using Acceptance and Commitment Therapy and Relational Frame Theory
- The Interpersonal Problems Workbook: ACT to End Painful Relationship Patterns
Client books
- ACT with Love: Stop Struggling, Reconcile Differences, and Strengthen Your Relationship with Acceptance and Commitment Therapy
- The Mindful Couple: How Acceptance and Mindfulness Can Lead You to the Love You Want
- LOSS/GRIEF
Client books
- The Reality Slap: Finding Peace and Fulfillment When Life Hurts
- OCCUPATIONAL/COACHING
- Acceptance and Mindfulness at Work: Applying Acceptance and Commitment Therapy And Relational Frame Theory to Organizational Behavior Management
- Maximize Your Coaching Effectiveness with Acceptance and Commitment Therapy
- The Mindful and Effective Employee: An Acceptance and Commitment Therapy Training Manual for Improving Well-Being and Performance
- PSYCHOSIS
Therapist guides
- Acceptance and Commitment Therapy and Mindfulness for Psychosis
- ACT for Psychosis Recovery: A Practical Manual for Group- Based Interventions Using Acceptance and Commitment Therapy
- Incorporating Acceptance and Mindfulness into the Treatment of Psychosis: Current Trends and Future Directions
- Treating Psychosis: A Clinician’s Guide to Integrating Acceptance and Commitment Therapy, Compassion-Focused Therapy, and Mindfulness Approaches within the Cognitive Behavioral Therapy Tradition
- RELIGION/SPIRITUALITY
Therapist guides
- Acceptance and Commitment Therapy for Christian Clients: A Faith-Based Workbook
- ACT for Clergy and Pastoral Counselors: Using Acceptance and Commitment Therapy to Bridge Psychological and Spiritual Care
- Faith-based ACT for Christian clients: An integrative treatment approach
- SOCIAL WORK
- Mindfulness and Acceptance in Social Work
- SPORTS/HUMAN PERFORMANCE
- The Psychology of Enhancing Human Performance: The Mindfulness-Acceptance-Commitment Approach
- The Winner’s Mind: Strengthening Mental Skills in Athletes
- SUBSTANCE ABUSE/ADDICTION
Therapist guides
- Acceptance and Commitment Therapy for Pathological Gamblers
- Acceptance and Commitment Therapy for Substance Abuse: A Clinician’s Guide to Using Practical Mindfulness and Acceptance- Based Interventions for Alcoholism and Drug Addiction
- Investigating Acceptance and Commitment Therapy within Addictions
- Mindfulness and Acceptance for Addictive Behaviors: Applying Contextual CBT to Substance Abuse and Behavioral Addictions
- Mindfulness-Based Sobriety: A Clinician’s Treatment Guide for Addiction Recovery Using Relapse Prevention Therapy, Acceptance and Commitment Therapy, and Motivational Interviewing
Client books
- Power Over Addiction: A Harm Reduction Workbook for Changing Your Relationship with Drugs
- The Wisdom to Know the Difference: An Acceptance and Commitment Therapy Workbook for Overcoming Substance Abuse
- TRAUMA/PTSD
Therapist guides
- Acceptance and Commitment Therapy for the Treatment of Post-Traumatic Stress Disorder and Trauma-Related Problems: A Practitioner’s Guide to Using Mindfulness and Acceptance Strategies
Client books
- Dark Agents, Book One: Violet and the Trial of Trauma
- Finding Life Beyond Trauma: Using Acceptance and Commitment Therapy to Heal from Post-Traumatic Stress and Trauma-Related Problems
- The PTSD Survival Guide for Teens: Strategies to Overcome Trauma, Build Resilience, and Take Back Your Life (The Instant Help Solutions Series)
- WORK/COACHING/BUSINESS
- Acceptance and Commitment Coaching (Coaching Distinctive Features)
- Acceptance and Mindfulness at Work: Applying Acceptance and Commitment Therapy And Relational Frame Theory to Organizational Behavior Management
- Maximize Your Coaching Effectiveness with Acceptance and Commitment Therapy
- Prosocial: Using Evolutionary Science to Build Productive, Equitable, and Collaborative Groups
- The Mindful and Effective Employee: An Acceptance and Commitment Therapy Training Manual for Improving Well-Being and Performance
- The psychology of enhancing human performance: The Mindfulness-Acceptance-Commitment (MAC) approach
- YOGA
- Mindful Yoga-Based Acceptance and Commitment Therapy: Simple Postures and Practices to Help Clients Achieve Emotional Balance
ACT Books: Self Help
ACT Books: Self HelpSelf-Help and Life Enhancement Resources |
Please note that not all ACT self help books have been specifically empirically validated. A list of such studies is here and you can search for additional RCT studies here.
The World Health Organization also distributes an extensively validated free ACT self-help book Doing What Matters in Times of Stress: An Illustrated Guide and audio recordings to go with it: https://www.who.int/publications-detail/9789240003927
(The following list of books is from the LEARNING ACT RESOURCE GUIDE: The complete guide to resources for learning Acceptance & Commitment Therapy by Jason Luoma, Ph.D. Updated July 2020 learningact.com)
Self-Help, Self-Improvement, and Skills Workbooks
- ACT SELF HELP BOOKS
- Acceptance and Commitment Therapy: Principles of Becoming More Flexible, Effective, and Fulfilled
- The ACT Deck: 55 Acceptance & Commitment Therapy Practices to Build Connection, Find Focus and Reduce Stress
- ACTivate Your Life: Using acceptance and mindfulness to build a life that is rich, fulfilling and fun
- Break Free: Acceptance and Commitment Therapy in 3 Steps: A Workbook for Overcoming Self-Doubt and Embracing Life
- Cognitive Behavioral Therapy: A Guide to Self-Empowerment with CBT, DBT, and ACT: How to Build Brain Strength and Reshape Your Life with Behavioral Therapy
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous Life
- The Diet Trap: Feed Your Psychological Needs and End the Weight Loss Struggle Using Acceptance and Commitment Therapy
- Escaping the Emotional Roller Coaster: ACT for the emotionally sensitive
- Get Out of Your Mind and Into Your Life: The New Acceptance and Commitment Therapy
- Get the Life You Want: Finding Meaning and Fulfillment through Acceptance and Commitment Therapy
- The Happiness Trap: How to Stop Struggling and Start Living
- How to Be Nice to Yourself: The Everyday Guide to Self Compassion: Effective Strategies to Increase Self-Love and Acceptance
- The Illustrated Happiness Trap: How to Stop Struggling and Start Living
- Learning to Thrive: An Acceptance and Commitment Therapy Workbook
- The Mindfulness and Acceptance Workbook for Self Esteem
- The Mindfulness and Acceptance Workbook for Stress Reduction: Using Acceptance and Commitment Therapy to Manage Stress, Build Resilience, and Create the Life You Want (A New Harbinger Self-Help Workbook)
- The Power of Small: Making Tiny Changes When Everything Feels Too Much
- Reclaim Your Life: Acceptance and Commitment Therapy in 7 Weeks
- Sex ACT: Unleash the Power of Your Sexual Mind with Acceptance & Commitment Therapy
- Stress Less, Live More: How Acceptance and Commitment Therapy Can Help You Live a Busy yet Balanced Life
- Therapy Quest: An Interactive Journey Through Acceptance And Commitment Therapy
- Your Life on Purpose: How to Find What Matters and Create the Life You Want
Self Help Books for Specific Populations
- ANGER
- Act on Life Not on Anger: The New Acceptance & Commitment Therapy Guide to Problem Anger
- The Moral Injury Workbook: Acceptance and Commitment Therapy Skills for Moving Beyond Shame, Anger, and Trauma to Reclaim Your Values
- ANXIETY
- The ACT on Anxiety Workbook
- The ACT Workbook for OCD: Mindfulness, Acceptance, and Exposure Skills to Live Well with Obsessive-Compulsive Disorder
- Anxiety Happens: 52 Ways to Find Peace of Mind
- Be Mighty: A Woman’s Guide to Liberation from Anxiety, Worry, and Stress Using Mindfulness and Acceptance
- Cognitive Behavioral Therapy: How to Use CBT to Overcome Anxiety, Depression and Intrusive Thoughts + A Guide to Acceptance and Commitment Therapy and ACT Techniques
- The Confidence Gap: A Guide to Overcoming Fear and Self-Doubt
- In This Moment: Five Steps to Transcending Stress Using Mindfulness and Neuroscience
- Let Go of Anxiety: Climb Life’s Mountains with Peace, Purpose, and Resilience
- Living Beyond OCD Using Acceptance and Commitment Therapy: A Workbook for Adults
- The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy (2nd Edition)
- The Mindfulness and Acceptance Workbook for Social Anxiety and Shyness: Using Acceptance and Commitment Therapy to Free Yourself from Fear and Reclaim Your Life
- Outsmart Your Anxious Brain: Ten Simple Ways to Beat the Worry Trick
- Social Courage: Coping and thriving with the reality of social anxiety
- Ten Little Ways to Beat the Worry Trick: Outsmart Anxiety, Fear, and Panic
- Things Might Go Terribly, Horribly Wrong: A Guide to Life Liberated from Anxiety
- Trichotillomania: An ACT-Enhanced Behavior Therapy Approach Workbook (Treatments That Work)
- The Worry Trap: How to Free Yourself from Worry & Anxiety Using Acceptance and Commitment Therapy
- CANCER
- Flying over Thunderstorms: Living Your Life with Cancer through Acceptance and Commitment Therapy
- CHILDREN/ADOLESCENTS/PARENTING
- Acceptance and Mindfulness Toolbox for Children and Adolescents: 75+ Worksheets & Activities for Trauma, Anxiety, Depression, Anger & More
- The ACT Workbook for Teens with OCD
- Becoming Mum
- Dark Agents, Book One: Violet and the Trial of Trauma
- Get Out of Your Mind and Into Your Life for Teens: A Guide to Living an Extraordinary Life
- The Gifted Kids Workbook: Mindfulness Skills to Help Children Reduce Stress, Balance Emotions, and Build Confidence
- The Joy of Parenting: An Acceptance and Commitment Therapy Guide to Effective Parenting in the Early Years
- The Mental Health and Wellbeing Workout for Teens: Skills and Exercises from ACT and CBT for Healthy Thinking
- The Mindfulness and Acceptance Workbook for Teen Anxiety: Activities to Help You Overcome Fears and Worries Using Acceptance and Commitment Therapy (Instant Help Book for Teens)
- Nuna and the Fog
- Parenting a Troubled Teen: Manage Conflict and Deal with Intense Emotions Using Acceptance and Commitment Therapy
- Parenting Your Anxious Child with Mindfulness and Acceptance: A Powerful New Approach to Overcoming Fear, Panic, and Worry Using Acceptance and Commitment Therapy
- Stuff That Sucks: Accepting What You Can’t Change and Committing to What You Can
- DEPRESSION
- The Mindfulness and Acceptance Workbook for Depression: Using Acceptance and Commitment Therapy to Move Through
- Depression and Create a Life Worth Living (2nd Edition)
- EATING DISORDERS/BODY IMAGE
- The Anorexia Workbook: How to Accept Yourself, Heal Your Suffering, and Reclaim Your Life
- Living with Your Body and Other Things You Hate: How to Let Go of Your Struggle with Body Image Using Acceptance and Commitment Therapy
- HEALTH/CHRONIC PAIN/INTEGRATED CARE
- Better Living With IBS: A step-by-step program to managing your symptoms so you can enjoy life to the full!
- The Diabetes Lifestyle Book
- End the Insomnia Struggle: A Step-by-Step Guide to Help You Get to Sleep and Stay Asleep
- Living Beyond Lyme: Reclaim Your Life From Lyme Disease and Chronic Illness
- Living Beyond Your Pain: Using Acceptance & Commitment Therapy to Ease Chronic Pain
- INTERPERSONAL/RELATIONSHIP ISSUES
- ACT with Love: Stop Struggling, Reconcile Differences, and Strengthen Your Relationship with Acceptance and Commitment Therapy
- The Mindful Couple: How Acceptance and Mindfulness Can Lead You to the Love You Want
- Saying The Wrong Thing: How to Speak Up in Difficult, Controversial, or Emotionally Charged Conversations
- LOSS/GRIEF
- The Reality Slap: Finding Peace and Fulfillment When Life Hurts
- SPORTS/HUMAN PERFORMANCE
- The Psychology of Enhancing Human Performance: The Mindfulness-Acceptance-Commitment Approach
- The Winner’s Mind: Strengthening Mental Skills in Athletes
- SUBSTANCE ABUSE/ADDICTION
- Power Over Addiction: A Harm Reduction Workbook for Changing Your Relationship with Drugs
- The Wisdom to Know the Difference: An Acceptance and Commitment Therapy Workbook for Overcoming Substance Abuse
- TRAUMA/PTSD
- Dark Agents, Book One: Violet and the Trial of Trauma
- Finding Life Beyond Trauma: Using Acceptance and Commitment Therapy to Heal from Post-Traumatic Stress and Trauma-Related Problems
- The PTSD Survival Guide for Teens: Strategies to Overcome Trauma, Build Resilience, and Take Back Your Life (The Instant Help Solutions Series
RFT/Behavior Analysis Books
RFT/Behavior Analysis Books- Dixon, M.R., Hayes, S.C., & Belisle, J. (2023). Acceptance and Commitment Therapy for Behavior Analysts. New York: Routledge.
- Ming, S., Gould, E., & Fiebig, J. (2023). Understanding and Applying Relational Frame Theory: Mastering the Foundations of Complex Language in Our Work and Lives as Behavior Analysts. Context Press.
- Fryling, M., Rehfeldt, R. A., Tarbox, J., & Hayes, L. J. (Eds.). (2020). Applied Behavior Analysis of Language and Cognition: Core Concepts and Principles for Practitioners. New Harbinger Publications.
- Villatte, M., Villatte, J. L., & Hayes, S. C. (2019). Mastering the clinical conversation: Language as intervention. New York: The Guilford Press.
- Törneke, N., Luciano, C., Barnes‐Holmes, Y., & Bond, F. W. (2015). RFT for clinical practice: Three core strategies in understanding and treating human suffering. Chapter in The Wiley handbook of contextual behavioral science, 254-272.
- Dahl, J., Stewart, I., Martell, C., Kaplan, J. (2014) ACT and RFT in Relationships: Helping Clients Deepen Intimacy and Maintain Healthy Commitments Using Acceptance and Commitment Therapy and Relational Frame Theory.
- Dymond, S., & Roche, B. (Eds.) (2013). Advances in relational frame theory: Research and application. New Harbinger Publications.
- McHugh, L., & Stewart, I. (2012). The self and perspective taking: Contributions and applications from modern behavioral science. Oakland: New Harbinger Publications.
- Törneke, N. (2010). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Reno, NV: Context Press.
- German Translation: Törneke, N. (2012). Bezugsrahmentheorie : Eine Einführung. Paderborn: Junfermann Verlag. (translated by Guido Plata)
- Korean translation: Törneke, N. (2019). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Hakjisa (translated by Lee, S.).
- Spanish Transation: Törneke, N. (2016). Aprendiendo TMR : una introducción a la Teoría del Marco Relacional y sus aplicaciones clínicas. Úbeda, Jaén: Didacbook. - Rehfeldt, R. A., Barnes-Holmes, Y. (2009). Derived relational responding: Applications for learners with autism and other developmental disabilities. Oakland, CA: New Harbinger Publications, Inc.
- Derived Relational Responding offers a series of revolutionary intervention programs for applied work in human language and cognition targeted at students with autism and other developmental disabilities. It presents a program drawn from derived stimulus relations that you can use to help students of all ages acquire foundational and advanced verbal, social, and cognitive skills. The first part of Derived Relational Responding provides step-by-step instructions for helping students learn relationally, acquire rudimentary verbal operants, and develop other basic language skills. In the second section of this book, you'll find ways to enhance students' receptive and expressive repertoires by developing their ability to read, spell, construct sentences, and use grammar. Finally, you'll find out how to teach students to apply the skills they've learned to higher order cognitive and social functions, including perspective-taking, empathy, mathematical reasoning, intelligence, and creativity. This applied behavior analytic training approach will help students make many substantial and lasting gains in language and cognition not possible with traditional interventions. - Dahl, J. C., Plumb, J. C., Stewart, I., & Lundgren, T. (2009). The Art and Science of Valuing in Psychotherapy: Helping Clients Discover, Explore, and Commit to Valued Action Using Acceptance and Commitment Therapy. Oakland, CA; New Harbinger Publications, Inc.
- The Art and Science of Valuing in Psychotherapy is an applied volume in purpose, but includes an RFT account of each of the ACT processes, and in particular an in depth RFT perspective on personal values and the clinical interventions employed to enhance them and promote committed action. - Ramnero, J., & Törneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- The ABCs of Human Behavior offers the practicing clinician a solid and practical introduction to the basics of modern behavioral psychology. The book focuses both on the classical principles of learning as well as more recent developments that explain language and cognition in behavioral and contextual terms. These principles are not just discussed in the abstract—rather the book shows how the principles of learning apply in a clinical context. Practical and easy to read, the book walks you through both common sense and clinical examples that will help you use behavioral principles to observe, explain, and influence behavior in a therapeutic setting. - Miltenberger, R.G., (2008). Behavior modification: Principles and procedures (4th Ed.). Pacific Grove, CA: Thomson/Wadsworth.
- Woods, D. W., & Kanter, J. W. (Eds.). (2007). Understanding behavior disorders: A contemporary behavioral perspective. Reno, NV: Context Press.
- Understanding behavior disorders presents a contemporary behavioral model of behavior disorders that incorporates the findings of current RFT and ACT research. Rich in possibilities for clinical work, this view of disordered behavior is an important milestone in clinical psychotherapy - an opportunity for behavioral clinicians to reintegrate their clinical practice with an experimental analysis of behavior. - Cooper, J.O., Heron, T.E. & Heward, W.L. (2007). Applied Behavior Analysis (2nd Edition). Prentice Hall.
- Applied Behavior Analysis (2nd Edition) is great resource to get you ready for the BCBA exam and to understand basic principals. - Baum, W. M. (2004). Understanding Behaviorism: Behavior, Culture, and Evolution (2nd edition). Wiley-Blackwell.
- Pierce, W.D. & Cheney, C.D. (2003). Behavior Analysis and Learning, 3rd edition.Lawrence Erlbaum.
- The "focus on research" and "on the applied side" sections in various chapters add an excellent generalization of concepts into interesting areas. There is a section on Bandura and the Bobo doll, review of Sidman's comments on coercion, review of the intrinsic/extrinsic reinforcement debates, a creativity section, respondent conditioning and heroin overdose, medical conditioning, and much more. - Barnes-Holmes, Y., Hayes, S. C., Barnes-Holmes, D., & Roche, B. (2001). Relational frame theory: A post-Skinnerian account of human language and cognition. In H. W. Reese & R. Kail (Eds.), Advances in Child Development and Behavior, Volume 28 (pp. 101-138). New York: Academic.
- Baldwin, J.D. & Baldwin, J.I. (2000). Behavior Principles in Everyday Life (4th Edition). Prentice Hall.
- Behavior Principles in Everyday Life (4th Edition) is a really accessible account of behavioral principles. Great accompaniment to ABCs of Human Behavior. - Dougher, M. J. (Ed.). (2000). Clinical Behavior Analysis. Reno, NV: Context Press.
- Chiesa, M. (1994). Radical Behaviorism: The philosophy and science. Cambridge Center.
- Leigland, S. (1992). Radical behaviorism: Willard Day on psychology and philosophy. Reno, NV: Context Press.
Puts Skinner's work in context; links history/philosophy and the battles of minds as a background to RFT/ACT. - Catania, C. (1992). Learning. Prentice Hall.
- Hayes, S. C. (Ed.). (1989/2004). Rule Governed behavior: Cognition, contingencies, and instructional control. New York: Plenum / reprinted in 2004 by Context Press.
- One of the first full-length presentations of the ACT / RFT model is in three chapters in this book on the topic. - Skinner, B.F. (1965). Science and Human Behavior. Free Press.
ACT Books in 20+ Languages
ACT Books in 20+ Languages CommunityGeneral Purpose Books on Contextual Behavioral Science
General Purpose Books on Contextual Behavioral ScienceGeneral Purpose Books on Contextual Behavioral Science |
- McHugh, L., Stewart, I., & Almada, P. (2019). A Contextual Behavioral Guide to the Self: Theory and Practice. Oakland, CA: New Harbinger.
- Wilson, D.S., Hayes, S.C. (2018) Evolution and Contextual Behavioral Science: An Integrated Framework for Understanding, Predicting, and Influencing Human Behavior. Context Press.
- Zettle, R. D., Hayes, S.C., Barnes-Holmes, D., Biglan, A. (2016) The Wiley Handbook of Contextual Behavioral Science (Wiley Clinical Psychology Handbooks) Wiley-Blackwell.
Ramnero, J., & Torneke, N. (March 2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: Context Press / New Harbinger.
It's a basic behavior analysis book for clinicians/ M.D.s/ psychiatrists/ etc. who haven't had training in BA. Goes all the way up to RFT. Nice.
Woods, D. W., & Kanter, J. W. (Eds.). (2007). Understanding behavior disorders: A contemporary behavioral perspective. Oakland, CA: Context Press/New Harbinger.
This volume presents a contemporary behavioral model of behavior disorders that incorporates the findings of current RFT and ACT research. Rich in possibilities for clinical work, this view of disordered behavior is an important milestone in clinical psychotherapy - an opportunity for behavioral clinicians to reintegrate their clinical practice with an experimental analysis of behavior.
Biglan, A. (1995). Changing cultural practices: A contextualistic framework for intervention research. Oakland, CA: Context Press/New Harbinger.
This is begins to show how you might scale these issues to the level of cultural practices. If the ACT model is correct, we either alter the prevalence of psychological inflexibility or we fail to help the human condition. You can do that one at a time, or in formal prevention efforts, but either way it is the same bottom line. No change in prevalence = failure. So we need to think about how to measure this and approach this wisely throughout the work we are doing.
Hayes, S. C., Hayes, L. J., Reese, H. W., & Sarbin, T. R. (Eds.). (1993). Varieties of scientific contextualism. Oakland, CA: Context Press/New Harbinger.
If you get interested in the philosophical foundations of ACT, this will help you understand them.
Leigland, S. (1992). Radical behaviorism: Willard Day on psychology and philosophy. Oakland, CA: Context Press/New Harbinger.
Puts Skinner's work in context; links history/philosophy and the battles of minds as a background to RFT/ACT.
Hayes, S. C. (Ed.). (1989/2004). Rule Governed behavior: Cognition, contingencies, and instructional control. New York: Plenum / reprinted in 2004 by Context Press and currently sold by Oakland, CA: Context Press/New Harbinger..
One of the first full-length presentations of the ACT / RFT model is in three chapters in this book on the topic. This book is now available in paperback from Context Press.
FAP and CFT Books
FAP and CFT Books- FAP Books
- Gareth Holman PhD, Jonathan Kanter PhD, Mavis Tsai PhD, Robert Kohlenberg PhD, Steven C. Hayes (2017) Functional Analytic Psychotherapy Made Simple.
- Mavis Tsai, Robert J. Kohlenberg, Jonathan W. Kanter, Gareth I. Holman, Mary Plummer Loudon (2012) Functional Analytic Psychotherapy (CBT Distinctive Features)
- Mavis Tsai, Robert J. Kohlenberg, Jonathan W. Kanter, Barbara Kohlenberg, William C. Follette, Glenn M. Callaghan. (2008) The Practice of Functional Analytic Psychotherapy.
- Mavis Tsai, Robert J. Kohlenberg, Jonathan W. Kanter, Barbara Kohlenberg, William C. Follette, Glenn M. Callaghan (2008) A Guide to Functional Analytic Psychotherapy: Awareness, Courage, Love, and Behaviorism.
- Mavis Tsai, Robert J. Kohlenberg. (2007) Functional Analytic Psychotherapy: Creating Intense and Curative Therapeutic Relationships. (Published in 1991 and republished in 2007)
- Translations of FAP Books
- Italian: Tsai, M. Kohlenberg, R., Kanter, J. W., Holman, G., Plummer Loudon, M. (2013). La psicoterapia analitico-funzionale (FAP). Caratteristiche distintive. (Ed. C. Orsini) Franco Angeli Edizioni.
- Portuguese: Holman, G., Kanter, J. W., Tsai, M., & Kohlenberg, R. (2022). Psicoterapia Analítica Funcional Descomplicada: Guia Prático Para Relações Terapêuticas (Rolim de Moura, P., Bastos Oshiro, C. K., & Villas-Bôas, A., Trans). Sinopsys Editora.
- Spanish: Kanter, J. W., Tsai, M., & Kohlenberg, R. J. (2021). La práctica de la psicoterapia analítico-funcional. (Ed J. Virues-Ortega) ABA Espanay.
- Spanish: Kohlenberg, R. J. & Tsai, M. (2021). FAP. Psicoterapia Analítico Funcional: Creación de relaciones terapéuticas intensas y curativas. Editociones Psara
- Compassion Focused Therapy Books for Therapists
- Gilbert, P. & Simos, G. (Editors) (2022). Compassion Focused Therapy: Clinical Practice and Applications. Routledge.
- Kolts, R.L., Bell, T., Bennett-Levy, J., Irons, C. (2018) Experiencing Compassion Focused Therapy from the Inside Out.
- Kolts, R.L. (2016) CFT Made Simple - An excellent and very readable introduction to compassion-focused therapy, with a fantastic chapter showing how to use chair-work with highly self-critical clients.
- Tirch, D., Schoendorff, B., Silberstein, L.R. (2014) The ACT Practitioner's Guide to the Science of Compassion - This is the first book on the market to provide an in-depth discussion of compassion in the context of ACT and other behavioral sciences. It offers case conceptualization, assessments, and direct clinical applications that integrate ACT, functional analytic psychotherapy, and compassion focused therapy to enhance your clinical practice.
- Gilbert, P. (2010) Compassion-Focused Therapy: Distinctive Features - A key reference source for learning compassion-focused therapy. It's concise, filled with clinical wisdom, and a handy reference for thinking through how to work with shame and self-criticism.
- Gilbert, P. (2009). The Compassionate Mind. London: Constable.
- Books based on Compassion-Focused Therapy for Clients
- How to Be Nice to Yourself: The Everyday Guide to Self Compassion by Laura Silberstein-Tirch (2019)
- The Mindful Self-Compassion Workbook: A Proven Way to Accept Yourself, Build Inner Strength, and Thrive by Kristin Neff and Christopher Germer (2018)
- Self-Compassion: The Proven Power of Being Kind to Yourself by Kristin Neff
- Compassion Focused Therapy for Dummies - From the publisher: Compassion Focused Therapy For Dummies is a wonderful resource if you are seeing—or thinking about seeing—a therapist who utilizes compassion techniques, or if you would like to leverage the principles of compassion focused therapy to manage your own wellbeing.
- Mindful Compassion: How the Science of Compassion Can Help You Understand Your Emotions, Live in the Present, and Connect Deeply with Others. This book by Paul Gilbert (creator of compassion-focused therapy) and Choden (a Buddhist monk) presents the principles of compassion-focused therapy in an accessible manner. A great book for people wanting to develop a kinder, more compassionate way of related to themselves and others.
- The Power of Self-Compassion: Using Compassion-Focused Therapy to End Self-Criticism and Build Self-Confidence by Welford and Gilbert. This book uses tools from Compassion-Focused Therapy to guide increased self-compassion and self-confidence.
- An Open-Hearted Life: Transformative Methods for Compassionate Living from a Clinical Psychologist and a Buddhist Nun is written in short chapters that make it easy to consume. Each chapter can be read in one sitting, each has a brief exercise to put to use the concepts therein, and each covers one topic that is important to living a more compassionate life.
- The Compassionate Mind Guide to Overcoming Anxiety - This book is written primarily from the perspective of compassion-focused therapy, but also integrates techniques from acceptance and commitment therapy. This might be a particularly relevant book for people who are both anxious and highly self-critical.
- The Mindful Path to Self-Compassion: Freeing Yourself from Destructive Thoughts and Emotions. By C.K. Germer
- The Compassionate-Mind Guide to Managing Your Anger – A book based on compassion-focused therapy on how to bring compassion to the pain of anger and feeling threatened.
- The Compassionate-Mind Guide to Recovering from Trauma and PTSD - A book based on compassion-focused therapy on how to bring compassion to people who have survived trauma and abuse.
- The Compassionate-Mind Guide to Ending Overeating - A book based on compassion-focused therapy for people who binge or suffer from disordered eating.
- The Compassionate-Mind Guide to Building Social Confidence - A book based on compassion-focused therapy for people who are shy or suffer from social anxiety.
- Mindfulness and other Third Generation Books
- Jonathan Feiner (2020). Mindfulness: A Jewish Approach. Mosaica Press.
- Christopher Germer, Ronald D. Siegel, and Paul R. Fulton, Editors (2016) Mindfulness and Psychotherapy, Second Edition.
- Ann F. Haynos, Evan Forman, Meghan Butryn, and Jason Lillis, Editors (2016) Mindfulness and Acceptance for Treating Eating Disorders and Weight Concerns: Evidence-Based Interventions
- Matthew D. Skinta and Aisling Curtin (2016) Mindfulness and Acceptance for Gender and Sexual Minorities: A Clinician's Guide to Fostering Compassion, Connection, and Equality Using Contextual Strategies
- Dennis Tirch, Laura R. Silberstein-Tirch, Russell L. Kolts (2015) Buddhist Psychology and Cognitive-Behavioral Therapy: A Clinician's Guide
- Paul Gilbert and Choden. (2014). Mindful Compassion: How the Science of Compassion Can Help You Understand Your Emotions, Live in the Present, and Connect Deeply with Others.
- Matthew S. Boone, Editor (2014) Mindfulness and Acceptance in Social Work: Evidence-Based Interventions and Emerging Applications
- Jason M. Stewart, Editor (2014) Mindfulness, Acceptance, and the Psychodynamic Evolution: Bringing Values into Treatment Planning and Enhancing Psychodynamic Work
- Jacqueline Pistorello, Editor (2013) Mindfulness and Acceptance for Counseling College Students: Theory and Practical Applications for Intervention, Prevention, and Outreach
- Todd B. Kashdan and Joseph Ciarrochi, Editors (2013) Mindfulness, Acceptance, and Positive Psychology: The Seven Foundations of Well-Being
- Steven C. Hayes and Michael Levin, Editors (2012) Mindfulness and Acceptance for Addictive Behaviors: Applying Contextual CBT to Substance Abuse and Behavioral Addictions
- Lance McCracken (2011) Mindfulness and Acceptance in Behavioral Medicine: Current Theory and Practice
- Steven C. Hayes, Victoria M. Follette, and Marsha M. Linehan, Editors (2011) Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition
- Richard W. Sears, Dennis D. Tirch, Robert B. Denton (2011) Mindfulness in Clinical Practice
- Lizabeth Roemer and Susan M. Orsillo (2010) Mindfulness- and Acceptance-Based Behavioral Therapies in Practice (Guides to Individualized Evidence-Based Treatment)
- Ruth Baer, Editor (2010) Assessing Mindfulness and Acceptance Processes in Clients: Illuminating the Theory and Practice of Change
- Kelly G. Wilson PhD and Troy DuFrene (2009) Mindfulness for Two: An Acceptance and Commitment Therapy Approach to Mindfulness in Psychotherapy
- Kashdan, T. (2009). Curious? Discover the missing ingredient to a fulfilling life. New York, NY: Harper Collins.
- Flowers, S.H. (2009). The Mindful Path Through Shyness: How Mindfulness and Compassion Can Free You From Social Anxiety, Fear, and Avoidance. Oakland, CA: New Harbinger.
- Vieten, C. (2009). Mindful Motherhood: Practical Tools for Staying Sane During Pregnancy and Your Child’s First Year. Oakland, CA: New Harbinger.
- Greco, L., & Hayes, S. C. (Eds.). (2008). Acceptance and mindfulness treatments for children and adolescents: A practitioner's guide. Oakland, CA: New Harbinger. Shows how the work in acceptance and mindfulness is impacting the treatment of children and adolescents. Several ACT chapters; also includes DBT, MBCT, MBSR etc
- Baer, R. A. (Ed.). (2005). Mindfulness-based treatment approaches: Clinician's guide to evidence base and applications. New York: Academic Press. This book discusses the conceptual foundation, implementation, and evidence base for the four best-researched mindfulness treatments: mindfulness-based stress reduction (MBSR), mindfulness-based cognitive therapy (MBCT), dialectical behavior therapy (DBT) and acceptance and commitment therapy (ACT). All chapters were written by researchers with extensive clinical experience. Each chapter includes the conceptual rationale for using a mindfulness-based treatment and a review of the relevant evidence base.
- Orsillo, S. M., & Roemer, L. (Eds). (2005). Acceptance and mindfulness-based approaches to anxiety: New directions in conceptualization and treatment. New York: Kluwer Academic/Plenum. Includes conceptual and practical applications of ACT and other third-wave therapies to the anxiety disorders, with chapters covering ACT, DBT skills, and MBSR, as well as specific anxiety disorders, anxiety in children and basic research in anxiety and acceptance.
- Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2004). Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition. New York: Guilford Press. Meet most of the major approaches in the third wave. Shows that ACT is not alone. Lots of good ideas for expanding your clinical work inside a third wave model. More theoretical though than immediately practical.
- Dougher, M. J. (Ed.). (2000). Clinical Behavior Analysis. Oakland, CA: Context Press/NewHarbinger. Situates ACT, Behavioral Activation, and other approaches in clinical behavior analysis. That is the tradition where this work comes from.
- Hayes, S. C., Jacobson, N. S., Follette, V. M., & Dougher, M. J. (Eds.). (1994). Acceptance and change: Content and context in psychotherapy. Oakland, CA: Context Press/New Harbinger. The first comprehensive third wave book. It carved out the domain we are now busy filling. Still relevant, despite its age.
Books (Archives)
Books (Archives) CommunityACT Study Group for Beginners
ACT Study Group for BeginnersHow This Came About
In February 2004 several beginners, interested but little experienced with ACT, found themselves on the ACT listserve. The idea arose for launching an on-line study group for beginners. Very soon 30 or more folks signed in, and the “ACT study group for beginners” was born.
We began reading the book chapter by chapter, and discussing it on the listserve. The first, theoretical part was tough. Kate Partridge raised the idea of starting each discussion with a summary of a section of the book. The summarizing began on 04/13/04, when we reached the clinical part of the book.
What you find below is a uncensured, uncorrected collection of the summaries. They’re meant for discussion, not for teaching purposes per se, but we are allowing them to become part of this website simply because we hope they might be useful to other beginners. People from 7 countries did parts of it: Australia, Belgium, Canada, Netherlands, Spain, United Kingdom, and the USA. (More countries participated in the discussion: Germany, Israel, Sweden, …) It was fun to participate, and very inspiring, … but sometimes hard too: we chose a fixed schedule of weekly reading, discussing, and sometimes summarizing … but we were willing and committed.
Part of the value in doing this probably cannot be achieved just by reading these products. This way we structured it beginners, hesitatant to take part in discussions between more experienced ACT-ors, had unique learning opportunities by taking part in the beginners’ discussion. The “masters” could watch us and interfered when helpful, which also was stimulating. I can recommend the formula to other beginners and hesitating “lurkers”. It might be worth while to start a second round. But that’s up to others. Meanwhile, here are our written products.
Thanks to all beginners who participated, and to the listserve for the opportunity!
ACT Book Summary: Pages 81-86
ACT Book Summary: Pages 81-86Contributed by: Francis De Groot Part II: The clinical methods of ACT Chapters 3 to 9 present the ACT concepts and strategies. ACT = Acceptance and Commitment Therapy = Accept, Choose and Take action Goal: to move in the direction of chosen values, and accept the automatic effects of life's difficulties. Barriers: experiential avoidance & cognitive fusion Source of these barriers: verbal Act stages focus on shift from content of experience to context of experience Why?: to enable clients to pursue valued goals in life. During treatment metaphors, paradoxes, and experiential exercises are frequently used to undermine the traps of literal language and pliance. Metaphors:
- are not specific & proscriptive (less pliance)
- are more like pictures (more experiential)
- are easily remembered
Therapeutic paradox:
- not the classic therapeutic paradox to eliminate certain sympoms: e.g. "don't obey me". They rely on pliance
- = inherent paradox: functional contradictions between literal and functional properties of a verbal event: e.g. "try to be spontaneous"
Experiential exercises: To help contact potentially troublesome thoughts, feelings, memories, ...
- experience in a different context
- allows experience to be observed & studied experientially
- superior to discussing
Summary: More:
- pursuing of valued goals
- direct experience
- acceptance of negative experiences (thoughts, feelings, memories, bodily sensations, ...)
Less:
- literal language
- pliance
Use of: less "literalizing" verbal modalities: metaphors, paradoxes, experiential exercises Focus on: WHAT DOES YOUR EXPERIENCE TELL YOU? This also goes for therapists? Let's go for some tracking, not for pliance!
ACT Book Summary: Pages 87 - 91
ACT Book Summary: Pages 87 - 91Contributed by Kate Partridge Creative Hopelessness: Challenging the Normal Change Agenda [Comments in square brackets are from me. I know this summary is almost as long as the section itself, but doing it has really helped me understand it. Kate] Theoretical Focus Resistance to Change: Clients enter therapy because they have already struggled for a long time with "the problem", in many different ways (contemplation, planning, discussion, praying, reading, tapes, etc.) In spite of so much effort having been exerted, no solution to the problem has arisen. In this sense, the client is resistant to change. There are [at least] two reasons for this: 1) The client has not found the right way to fix the problem. 2) There is a fundamental flaw in the model for change, which is based on culturally sanctioned, language-based rules for solving problems. Culturally Sanctioned [Unconscious] Problem-Solving Rules:
- Psychological problems = the presence of unpleasant inner experiences (feelings, thoughts, sensations, etc.). The presence of these unpleasant experiences signal that "something is wrong and must be changed".
- "Healthy living" = the absence of these negative experiences.
- These experiences need to be eliminated by the correction of inner deficits (e.g., lack of confidence), through the understanding or modification of their causes (e.g., overcritical parents).
The underlying metaconcept is: "The problem is one of bad content; change the content and the problem will go away." ACT Assumption [Message of Hope and Liberation]: The Change Agenda Is Not Workable: The culturally sanctioned problem solving rules are like water to fish - they are taken so much for granted that to challenge them seems nonsensical. The ACT therapist works to undermine the sense of normality surrounding these rules, by showing that efforts based on these rules can actually be the source of problems, not their solution. The therapist asks: • "Which will you believe, your 'mind' or your actual experience of the unworkability of these rules?" [Not expressed in these words, naturally.] The therapist takes apart for the client the underlying logical assumption: 1) Identify the problem: "bad" thoughts and feelings. 2) Eliminate the problem: " " " " 3) Life will then improve. By drawing out multiple examples from the client's own history, the client can become experientially connected to what is often a long series of unsuccessful attempts to use this strategy. This can be quite painful. The therapist aims to organize most of the client's solutions into a general class of events that can be described as: "Control of private experience = Successful living." The client is (gently) encouraged to confront the reality of their multiple experiences of the unworkability of this assumption. This leaves the client often not knowing what to do next, in a state of "creative hopelessness". The state is "creative" because entirely new strategies can be developed with being overwhelmed by the old and previously unconscious rule system. Clinical Focus In this phase of ACT, the therapist focuses on the following issues:
- Client has tried everything, but the problem remains.
- The problem is not one of motivation, nor of specific tactics. The client is not to blame for being stuck.
- There is a paradox here: Working hard to solve the problem makes the problem seem worse. The solution is part of the problem. [I need some concrete examples here of how the solution makes things worse - KAP]
- The logic of the problem-solving system is flawed. A more valid and reliable source of problem-solving is the client's own direct experience and their feedback from life.
TABLE 4.1: ACT Goals, Strategies, and Interventions Regarding Creative Hopelessness. [There is no point in summarizing this useful table. It is on Page 91]. Informed Consent ACT interventions can be intense, and the client must be prepared for this by being provided with:
- general descriptions of operating principles [How general?]
- frank discussion of areas of ambiguity [What does this mean?]
- alternative forms of therapy that could be followed instead of ACT
Treatment involves the client in having to face previously avoided experiences. When this occurs, the client can start to question his/her commitment to treatment. Therefore, the client should be committed to meeting for a certain number of sessions, to expect ups and downs, and to hang in until a progress review occurs at a specified session. In this way, the client is guided away from impulsively dropping out of treatment.
ACT Book Summary: Pages 92 - 98
ACT Book Summary: Pages 92 - 98ACT Book Summary: Pages 98 - 105
ACT Book Summary: Pages 98 - 105- Begins by noting that engendering creative hopelessness is the first ACT intervention (following thorough assessment of the client's 'presenting problem', change agenda, and strategies that have been tried to resolve it.
- Also notes (or warns) that doing this inevitably involves the use of human language, which is part of the trap the client is in anyway - the conundrum of attempting to side- step the trap of language, but needing to use language to deliver interventions. The therapist is thus just as susceptible as the client to the trap of literal language, and must be careful about too strongly believing or becoming fixed on the logic of words.
- This highlights the equality of therapist and client, with the therapist's only advantage that of having an outside perspective (the client would also have this advantage were the therapist's problems the topic of discussion).
- The therapist confronts the system by working outside it, using language only to meet certain ends, not to change beliefs or model more "rational" beliefs and thoughts. If those ends are not met, then the words are not true, no matter how logical. So this takes us from the typical reliance on logic to relying on workability - this become our metric. The question for both clients and therapists is "does that work for you?".
- In the beginning of this section, the authors provide a caveat that it is written with severely affected clients in mind (although the tools are still useful in less severe circumstances).
- The work starts with confrontation, although of a different sort than typically thought. The confrontation is between the client's change agenda and the client's experience of the workability of that system. The message of the therapist and client being in the same boat as far as confronting this system (i.e. the therapist is not some expert who has all the answers) can be powerfully conveyed by the therapist sitting next to the client, with the system imagined as out in front, being confronted by both people together.
- The therapist is armed at this point with information related to strategies the client has tried in the past that haven't worked.
- Unworkability is gently suggested - the therapist highlights how hard the client has been thinking and working at the change agenda, and that consulting a therapist is another attempt to find a solution. Another powerful intervention here is to highlight that usually when we work this hard, things get accomplished, but that this situation seems different. All this effort has not resolved the issue.(this is a subtle way to highlight the role of the client's experience)
- This moves into a discussion of the notion that perhaps looking for solutions is part of the problem. That the client is stuck, and it's not because they are not clever enough to figure it out or are not trying. Perhaps it is because it can't work. The authors suggest that a way to make this more tangible to the client is to suggest that the client doesn't actually believe there is a solution - that anything offered by the therapist would likely just be refuted by the client based on the client' s experience that it would not work. So here, the idea that experience and mind tell the client different things, and that experience is more accurate is brought to the discussion.
- The authors break from the therapeutic dialogue here to discuss the importance of framing creative hopelessness as a positive thing. Being careful not to suggest that the client is hopeless or to engender hopeless feelings. But rather to introduce this idea as a starting point for giving up unworkable strategies and opening up for new possibilities to emerge.
- Several metaphors are provided, including the Man in the Hole metaphor, p. 101, to side-step the trap of language. This metaphor is flexible and can be used to address many issues a client might raise, such as:
- giving up
- belief in the need to delve into the past
- responsibility
- blame
- continuing to look for solutions - this one actually seems really important and I think best highlights the goals of this part of therapy. The therapist really seems to stay away from promising solutions, but takes on a role of saying "I don't know". The goal at this point is batter down the tendency toward sense-making and to stay with the importance of the client giving up unworkable strategies, even without any promise of what will come next. This is a leap of faith and should be noted as such, since clients (like the rest of us) are definitely not used to not trying to make sense of things when there are problems in our lives.
- illustrating the opportunity suffering presents for us to learn to disentangle ourselves from our own minds.
ACT Book Summary: Pages 105 - 110
ACT Book Summary: Pages 105 - 110ACT Book Summary: Pages 110 - 114
ACT Book Summary: Pages 110 - 114ACT Book Summary: Pages 115 - 118
ACT Book Summary: Pages 115 - 118- "Deliberate control works well for me in the external world."
- "I was taught it should work with personal experiences (e.g., 'Don't be afraid...')."
- "It seems to work for other people around me (e.g., 'Daddy never seemed scared...')."
- "It even appears to work with certain experiences I've struggled with (e.g., relaxation works for a while to reduce my anxiety symptoms)." It is emphasized that the examination of control strategies is based entirely on the clients experience, with workability as the unit of analysis, and that the therapist needs to be extremely careful not to dictate or demand that the client evaluate their control strategies as unworkable. Therapist techniques that are mentioned include using metaphors and experiential exercises to help the client develop increasing sensitivity to directly experienced contingencies. Also, the authors mention that asking questions rather than stating conclusions can be helpful in reducing pliance on the part of the client.
ACT Book Summary: Pages 119 - 125
ACT Book Summary: Pages 119 - 125- If I'm not willing to have it (e.g., anxiety), I have it
- If I don't get so uptight about being anxious, I will be less anxious
- If I am willing to have it in order to get rid of it, I am not willing to have it and I will have it again
- contrast between controllable behaviors (i.e., paint the wall or I will shoot you) versus behavior that is not regulated successfully by verbal rules (relax or I'll shoot you)
- People carry their own polygraph with them all the time (their nervous system) and their own gun (self-esteem, self-worth). They are constantly monitoring for symptoms (e.g., anxiety) and firing the gun at themselves
- How seemingly successful attempts to make situation work, don't work in the long term. For example, taking valium may help you relax initially but what about when it wears off?
- either it is particularly difficult not to think about it (me included in this group)
- or attempts to not think about it (e.g., "I thought about something else") actually require you to think about chocolate cake (you have to know what you are not thinking about)
ACT Book Summary: Pages 125 - 132
ACT Book Summary: Pages 125 - 132ACT Book Summary: Pages 132 - 135
ACT Book Summary: Pages 132 - 135- designed to look at concept of control and its relationship to distress
- Should be linked to clients' experience of their own futile effort to control distress, can link it to more mundane or less meaningful examples for the client (for example, trying to sleep during a bout of insomnia. The harder you try to fall asleep the less sleep you get. In supervision, we often use the Chinese finger trap example-the harder you try to get out of it, the less out of it you are- you get stuck.)
- Want to undermine the client's confidence in the control strategy and depathologize the struggle over control
- Not crazy, just using the wrong strategy
ACT Book Summary: Pages 136 - 141
ACT Book Summary: Pages 136 - 141- willingness is appearing spontaneously in situations that used to elicit control
- clients report spontaneous examples of feeling feelings differently
ACT Book Summary: Pages 141 - 147
ACT Book Summary: Pages 141 - 147- personal work for the clinician
- a clinical vignette
- appendices containing daily experiences diary, identifying programming exercise, feeling good exercise, rules of the game exercise and clean versus dirty discomfort diary. I'll deal with each of these in turn:
ACT Book Summary: Pages 148 - 154
ACT Book Summary: Pages 148 - 154Building Acceptance by Defusing Language
Here are some nuts and bolts followed by questions and critiques:
1. The distinction between process and content: language is a learned set of derived stimulus relations, while languaging is the action of deriving those relations.
2. Humans (therapists, clients, etc.) often don't make this distinction and often relate on (and become connected to) the content level. Taking these contents at "face value" (i.e., literally, tangibly) in turn, leads to powerful and predictable behavior patterns (that are often destructive) on the part of the client.
3. One of the main paradoxes in ACT is that language cannot be weakened by more language; however the essence of deliteralization is to take advantage of loopholes in the way language functions (by teaching the client to see that thoughts and feelings are just that-thoughts and feelings).
4. Page 152 contains a table (6.1) of ACT goals, strategies, and interventions to use regarding deliteralization.
5. One of the ways to begin addressing the paradox and function of language is to demonstrate to the client the limits of language in deciphering human experience (and to elicit their own examples). For example, there are two metaphors (found on page 153) that communicate how describing something is different from experiencing it. One metaphor is "finding a place to sit," which essentially describes how talking about a chair (its features, uses) does not help when one wants to actually sit down. In other words, one cannot "sit" in a description of a chair. One can only sit IN an actual chair. A corollary of this metaphor is that one can describe the experience of swimming (how the water feels moving through it, its temperature, etc.). However, one cannot learn to swim in or by a description.
6. There is an assumption in ACT that "your mind is not your friend." Extrapolating from pre-human experience, one can see that the (human) mind was not developed to make humans or "prehumans" feel good. It was developed to keep humans from danger and was mostly comprised of negative content. Explain to clients the paradox "your mind is not your friend AND you cannot live without it."
7. Another assumption is that language is arbitrary and that once it is learned, it becomes relatively independent of immediate environmental support. This reminds me of my nanny's (successful) efforts to train my 20 month-old son to say "bling-bling" when he sees jewelry-now without her having to label it.
8. There is a provocative quote related to the usefulness of nonverbal (experiential?) knowledge at the end of this section on page 154: "If we suddenly had all nonverbal knowledge removed from our repertoires-we would fall to the floor quite helpless."
Comments/questions:
9. It has been my experience that, while clients appear "fused" to a lot of different ideas/contents, a great share of them come to my office without having specific terms/language to describe their experience. In fact they come ONLY with experience, which they have a difficult time describing in words. For example, an extremely anxious patient I had (with Posttraumatic Stress Disorder) wouldn't ever label himself as "anxious," rather he just knows he feels bad.
10. I don't know if behavior patterns follow from the premise that one does not make a distinction between the process of thinking and actual thought, and becomes fused with actual thought content, thereby leading directly to ingrained behavior patterns. I suppose one could explain this as troublesome behavior patterns becoming automatic due to conditioning (i.e., not being aware of the interaction pattern itself); however, I'm not sure if this is because one is fused to a verbal event.
11. Have any of these hypotheses been evaluated using individuals with various types of brain injuries (resulting in apraxia, aphasia, acquired deficits in language versus acquired deficits in motor ability, etc.)?
ACT Book Summary: Pages 154 - 158
ACT Book Summary: Pages 154 - 158- Thoughts are used to structure our perception of the world. We don't even notice that we look at the world from our thoughts, because we believe them in literal way. To look at the process of language involves focusing attention on language as language, cryptic as this may sound. A bit of defusion from literal 'understanding' can be achieved by watching the direct stimulus functions of language like sound, the feeling of your muscles, the sight, etc.
- An elegant way to watch your attention switch from the symbolic function of a word to some of its direct stimulus functions is by repeating a word over and over again for one or two minutes. This is the classic milk, milk, milk exercise (Titchener, 1916). Present it as an experiment or experiential exercise and help the client notice how the literal meaning of the word disappears and one can see the word as an instant of the language process.
- I like the notion of skill learning here. Deliteralization is a skill you can practice, it's not another rule to follow. One can play with direct stimulus properties and thereby loosen the 'grand illusion of language' by realizing that the symbolized thing is not there at all. The only thing that's there is sound, movement, breathing and so on. And this is not a fact, but a skill, something you do.
- You, the driver of the bus. You want to go places and do your job.
- The passengers are your thoughts and all kinds of inner states. Some are nice, some ugly, scary, nasty.
- The scary ones threat you and want to come up front where you'll see them.
- You take this very serious and stop the bus (you don't go anywhere anymore) and try to make a deal with them: they'll keep quiet in the back of the bus, only when you do exactly what they tell you.
- This means your route plan is greatly impaired and you're always on the watch inside the bus.
- What happens is that you let these passengers control the whereabouts of the bus. You, the driver, are not in control at all.
- Even though these passengers look scary, nasty, threatening etc. they can't take control (unless you let them). They can't make you do something against your will.
ACT Book Summary: Pages 158 - 168
ACT Book Summary: Pages 158 - 168ACT Book Summary: Pages 168 - 174
ACT Book Summary: Pages 168 - 174ACT Book Summary: Pages 174 - 179
ACT Book Summary: Pages 174 - 179ACT Book Summary: Pages 180 - 187
ACT Book Summary: Pages 180 - 187- Int: So, we've talked a lot about what your critics think of you and your work, what your wife and ex-wives and children think. I have to ask, what do you think about Clint Eastwood?
- CE: I tend not to think about him very much.
- When I am x and I and my community do much better when I am x, I am pretty invested in remaining x, because if I act as Y there are consequences
- Our history has taught us to see and maintain patterns.
- We have equivalency statements that may not be equivalent "I am 5'10" (maybe 9") becomes the same as "I am alcoholic."
- If I try to act outside of "who I think I am," it seems almost life (or self?) threatening. Note: I wonder about this with the "guys" I work with. Many are domestic violence offenders, and even though their physicality is usually not threatened, many lash out when their sense of "self" is threatened, the "manly man syndrome." OR "Eliminate conceptualization = eliminate me."
ACT Book Summary: Pages 187 - 192
ACT Book Summary: Pages 187 - 192We're looking at the first part of the 'Clinical Focus' section of chapter 7 'Discovering Self, Defusing self'.
As will have been outlined earlier, this is an important part of ACT. The section begins with a brief outline of the core perspectives that are introduced here. Table 7.1 (p.188) provides the ACT goals, strategies and interventions regarding self.
Initially, it is helpful to 'Undermine Attachment to a Conceptualized Self'. Clients may vary in readiness to work on this area. The timeless struggle between content and context is presenting itself here. ACT promotes the idea that the problem may lie in attachment to beliefs, rather than in the beliefs themselves. This may be seen as a reversal of some views in which self-conceptualization and performance are linked. The 'Mental Polarity Exercise' can be used here to demonstrate the effects of attachment to evaluative thoughts. The description of the exercise also describes the etymology of the word 'perfect'. This is also a powerful and important point, that, in my view is worthy of detailed attention.
Next we have a section on 'Building Awareness of the Observing Self', that aims to help the client notice the process of consciousness and sense of perspective. A 'central ACT intervention', the Chessboard Metaphor, is then described in detail, and a helpful brief therapist/client transcript provided. The Chessboard metaphor can be physically acted out in therapy. Issues such as willingness can be demonstrated through observing how little effort it takes for the board to hold the pieces. An important phrase - " The point is that thoughts, feelings, sensations, memories etc are pieces on the board, they are not you" (p.192).
A couple of notes from a beginner: As p.189 notes, 'therapists and clients are in this language stew together'. It is therefore as important for therapists to work on attachment to their own conceptualized self(-ves), as for the client (a theme of the book). I especially like the brief paragraph on perfect (p.190). In this sense, who is not 'thoroughly made'? This perspective may also carry over to the judgments and evaluations we make of others.
The Chessboard Metaphor is very useful - although I have had one or two clients wanting to sweep all of the pieces from the board (wipe the slate clean). John Billing gave us alternative metaphor on 16.06.04 (or 06.16.04, depending on which side of the pond you're on)
ACT Book Summary: Pages 192 - 198
ACT Book Summary: Pages 192 - 198ACT Book Summary: Pages 198 - 203
ACT Book Summary: Pages 198 - 203ACT Book Summary: Pages 205 - 212
ACT Book Summary: Pages 205 - 212ACT Book Summary: Pages 212 - 219
ACT Book Summary: Pages 212 - 219ACT Book Summary: Pages 219 - 229
ACT Book Summary: Pages 219 - 229These pages concern how to differentiate goals from values, methods to clarify values, ways to elicit actions related to values and how to evaluate barriers to valued action.
Outcome is the Process through which Process Becomes the Outcome
This section relates how needing to attain goals creates motivation and direction for action, but does not provide vitality in life. Attaining goals does not equal happiness or life satisfaction, as one is forced to live in a constant state of deprivation (interestingly, it is pointed out that the etymology of the word "want" is "missing").
The Gardening Metaphor describes how to stick it out with an initial choice (i.e., value) to see what happens (without believing that the "grass is greener on the other side," no pun intended). Another "goal" in this phase of therapy is to help clients see that the process of living equals the outcome of interest. The Skiing Metaphor describes this well. Your stated "goal" may be to get down to the lodge and you are planning to ski there. If someone whisks you off in a helicopter to bring you to the lodge, that would make you mad. It is the process of getting to the lodge (i.e., skiing) that is what is to be enjoyed.
Finally, process cannot be measured from moment to moment like goals. If one continually monitors progress toward specific goals, they may miss the " big picture" (i.e., what they have accomplished to date). Here the Path up the Mountain Metaphor comes into play. It highlights what is wrong with monitoring only "snapshots" of life. If you are hiking up a mountain, you may notice twists and turns, circling around (perhaps even going down the path in parts) ultimately to get up the mountain. You may think at any given time: "I'm doing well" (for instance on an up-path) or conversely: "I'm doing poorly" (on a down-path). Yet, an observer with binoculars across the way (looking down at the hikers) may notice steady, continuous progress toward the overall goal.
Values Clarification: Setting the Compass Heading
In this section, values work is further elaborated. The authors point out that doing values work can be an intimate experience between therapist and client, as oftentimes values are not something the client has ever articulate before to someone else. One of the "values" of "values work" is in the fact that values may help point out to clients what IS working in their lives (i.e., they may be leading valued lives in certain areas they hadn't even recognized). There are some values worksheets on page 224. There are three forms, including a values narrative form, values assessment rating form, and goals, actions, barriers form you can use with clients. The goal is to review the worksheets together and build on them. Values work may be a helpful assessment tool as well. In doing the values work, therapists can uncover possible "ulterior motives" for certain values. The authors give three examples:
- when values statements are controlled by the presence of the therapist, the consequence can be therapist approval or lack of disapproval.
- when values statements are controlled the presence of the culture more generally, the consequence can be the absence of cultural sanctions, broad social approval, or prestige.
- when values statements are controlled by stated or assumed values of the client's parents, the consequence can be parental approval
This is not to say that these factors don't affect EVERYONE'S values, but the extent to which the client takes ownership of their values is important to assess. When a client is wedded to the consequences mentioned above, the therapist can ask the client what would happen if the stated consequences were not there (i.e., "What if your parents did not know you received a Ph.D.?"). Another point the authors make is that it is not uncommon for values to change in valence over the course of therapy. Sometimes (oftentimes) clients may leave certain (or many) domains completely empty. In this situation it can be helpful for the therapist to ask the client what values he/she held earlier in life.
Assessing Goals and Actions
After values work is underway, the focus is on developing goals and specifying the actions that can be taken to achieve those goals. A goal is define as a specific achievement, accomplished in the service of a particular value. Clients do homework in acting according to values either as a one-time deal or from a commitment to repeated and regular acts in the service of a given value. The therapist and client monitor for a close connection between action, goal, and value and try to "accumulate small positives." The authors assert that little steps consistently taken are more useful than heroic steps taken inconsistently. What to do about barriers? The authors mention that engaging in valued action almost always provokes a psychological reaction (often in the form of barriers). At these times, clients may get stuck because they avoid taking values actions as a means of avoiding painful emotional barriers. The therapist then helps the client examine:
- the type of barrier
- ask if the barrier is something they can make room for and still act
- find out what aspect of the barrier may actually help reducing your willingness to have it without defense
- assess whether barriers are a form of emotional control or avoidance
Question
Although I am a big proponent of values work (or I wouldn't be doing this therapy), I am still struck by the similarity of values homework to "monitoring progress toward a goal," not noticing the process itself. In other words, the question "How well did you move toward this goal this week by these actions" seems like the very "snapshot" that is proposed as problematic in the initial part of this section. Any reactions?
ACT Book Summary: Pages 229 - 234
ACT Book Summary: Pages 229 - 234Willingness to have barriers and barriers to willingness: willingness is a value-based action, a choice: see the "Bubble in the road" metaphor p. 230. Therapeutic do's and don'ts:
- coercive use of choice: conflicts are possible between the therapist's and the client's values. Take care not to use "choice" as a way to blame the client.
- confusing values and goals: "I want to be happy" is not a value. It's no direction. It's something you can have or not have, like an object. Values cannot be achieved and maintained. Helping question: "What would you be able to do if that was accomplished?" Values are no means to an end.
ACT Book Summary: Pages 235 - 238
ACT Book Summary: Pages 235 - 238ACT Book Summary: Pages 238 - 244
ACT Book Summary: Pages 238 - 244ACT Book Summary: Pages 244 - 249
ACT Book Summary: Pages 244 - 249ACT Book Summary: Pages 249 - 254
ACT Book Summary: Pages 249 - 254Primary barriers to committed action:
When a client resists committed action, often the client is struggling with how the action will alter his (or her) personal history; how the client has created in his own mind his place in his world. The client may also be grappling with the impact this history has had on his conceptualized self. The client has constructed a self perception of who he is. If he has been subjected to an abusive or otherwise harmful environment, his self perception embraces how he has been victimized by others.
Not surprisingly, the client is threatened with the possibility of positive change. This threat challenges both the client's self perception and the hope that an abuser may someday validate the client's self perception and make amends. For example, a client was physically abused as a child. He now perceives himself as a victim of physical abuse; the perception is intertwined with his identity. If he makes positive change, he may no longer appear as a victim to himself or his abuser. He loses his self perceived identity (as a victim).
Clients with history of painful events (especially in childhood) may have learned that life can be unpredictable and punitive. By limiting their exposure to painful thoughts, they mistakenly believe they can curb their sense of trauma. The opposite is often true. Psychological pain hurts but does not damage; whereas psychological trauma is pain without the willingness to experience the pain. This unwilling causes damage; the effect of the pain persist.
An exercise to teach the difference between psychological pain and trauma:
- Ask the client to describe past painful and traumatic events in detail.
- distinguish between the original pain and,
- the client's reaction to the events.
2. Inventory the area of responses (i.e. physical reactions, emotional reactions, memories, thoughts, etc.)
3. Note the sense of trauma
4. As the client becomes aware of the reaction, ask the client to let go of the struggle with the reaction.
The client's willingness will shift the context of the events; this change will often reduce the client's tension related to the event. As a consequence, the client will be begin to distinguish between trauma and pain. The pain will remain; the trauma will disappear; positive change may occur. A client's reluctance and resistance can be expected. If so, the clinician should:
- point out to the client the burdened caused by resisting the avoided content
- have the client notice physical, emotional and cognitive responses that attach to the unwillingness
- prompt the client to let go of the struggle with unwillingness and be willing to be unwilling
- if the client is able to do this, ask the client to notice the difference between struggle and letting go
- encourage the client to continue the process of letting go and bringing up avoided material.
Things to remember:
- The therapist must identify the functional connection between failing to be "right" about being a victim and remaining a victim who demands redress.
- If the client believes he must remain "broken" in order to prove someone else wrong, the client is stuck, not broken.
- Intervention is delicate.
- The events in question are not being disputed.
- What is being disputed is the necessity of living in a self defeating life in the service of waiting for the recognition and redress that seldom, if ever, comes.
ACT Book Summary: Pages 254 - 259
ACT Book Summary: Pages 254 - 259ACT Book Summary: Pages 259 - 264
ACT Book Summary: Pages 259 - 264ACT Book Summary: Pages 267 - 271
ACT Book Summary: Pages 267 - 271ACT Book Summary: Pages 271 -275
ACT Book Summary: Pages 271 -275ACT Book Summary: Pages 275 - 288
ACT Book Summary: Pages 275 - 288- some useful rules are given (esp. for beginners): no more than 20% explanation, back to exercise, ...
- excessive focus on emotional processing: I was exactly doing this the very moment I read this piece. Back to values and behavior!
- remaining questions: what about clients not seeking help, but needing it (involuntary treatment); how to integrate RFT with other problems (not having to do with avoidance): impulsivity, aggression, ...
Book Translations (Archives)
Book Translations (Archives) CommunityTranslated ACT and RFT Books
Translated ACT and RFT BooksThis list is no longer being updated. Please click here for a list of ACT Books in 20+ Languages.
Translated ACT Books Organized by Language Community
(see below for list by English title)
- Chinese
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Chinese translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2016). 接纳承诺疗法(ACT)--正念改变之道 (Translators: Zhu Zhuzhuohong, Zhang Qi). Bejing: 知识产权出版社 (Intellectual Property Press).
- Hayes, S. C., & Lillis, J. (2012). Acceptance and Commitment Therapy. Washington, DC: American Psychological Association.
- Chinese translation: Hayes, S. C., & Lillis, J. (2016). 接纳承诺疗法(ACT). Translators: Zhu zhuohong, Cao Jing, & Wang Shujuan. Chongqing: 重庆大学出版社 (Chongqing University Press)
- Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004) (Eds.). Mindfulness and acceptance: Expanding the cognitive behavioral tradition. New York: Guilford Press.
- Chinese translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2005.) Mindfulness and acceptance: Expanding the cognitive behavioral tradition. Shanghi: Ewen Publishers. [2011]
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Chinese translation: 羅斯.哈里斯(2009)。快樂是一種陷阱。台北:張老師文化。
- Bach, P., & Moran, D. (2008). ACT in practice: Case conceptualization in Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Chinese translation: 帕特里夏·A.巴赫(Patricia A.Bach)、(美國)丹尼爾·J.莫蘭(2011)。接受與實現療法:理論與實務。重慶:重慶大學出版社。
- John P. Forsyth, & Georg H. Eifert. (2008). The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Chinese translation: 約翰.福賽思(John.P.Forsyth)、格奧爾格.艾弗特(Georg H.Eifert)(2010)。晚安,我的不安:緩解焦慮自助手冊。四川:四川人民出版社。
- Patricia J. Robinson, & Kirk D. Strosahl. (2008). The Mindfulness and Acceptance Workbook for Depression. Oakland, CA: New Harbinger.
- Chinese translation: 科尔克.斯特尔萨拉,派翠西娅.罗宾逊(2010)。抑郁的自我疗法:用接受与实现疗法走出抑郁。华东:华东师范大学出版社。
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Chinese translation: Hayes, S. C., & Smith, S. (2010). Zǒuchū nǐ de tàidù, zài nǐ de shēnghuó: Xīn Acceptance and Commitment Therapy. Chongqing, China: Chongqing University Press.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Danish
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Danish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2013). Acceptance en Commitment Therapy: Psykologisk fleksibilitet og mindfulnessprocessor (2nd edition). Translator: Bjorn Nake. Copenhagen, Denmark: Hans Reitzel Publishers).
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Danish translation: Hayes, S. C., & Smith, S. (2008). Slip tanketyrraniet – tag fat på livet. (Trans. T. Bøgeskov). Copenhagen: Dansk Psykologisk Forlag.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Dutch
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Dutch translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance en Commitment Therapie: Veranderingen door mindfulness, het process en de praktijk. (2nd edition). Amsterdam: Pearson Education Publishers.
- Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- Dutch translation: Luoma, J., Hayes, S. C., & Walser, R. (2009). Leer ACT. Vaardigheden voor therapeuten (Trans. L. Berkhuizen, P. van der Kaaij, & J. A-Tjak). Houten, The Netherlands: Bohn Stafleu van Loghum.
- Hayes, S. C., Strosahl, K. & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
- Dutch translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2006). ACT. Een experiëntiële weg naar gedragsverandering. Nederlandse bewerking (trans. By Ando Rokx). ISBN 90 265 1758 0 Verschijnt zomer 2006 Prijs: C.a. € 50, -
- Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004) (Eds.). Mindfulness and acceptance: Expanding the cognitive behavioral tradition. New York: Guilford Press.
- Dutch translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2006). Mindfullnes en acceptatie. De derde generatie gedragstherapie . (Trans. By Ando Rokx). Nederlandse bewerking. ISBN 90 265 1759 9 Verschijnt zomer 2006 Prijs: C.a. € 50, -
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Dutch translation: Hayes, S. C., Smith, S. (2006). Uit je hoofd, in het leven. Een werkboek voor een waardevol leven met mindfulness en Acceptatie en Commitment Therapie. (Trans. A. Rokx). Amsterdam: Uitgeverij Nieuwezijds.
- Eifert, G. H., McKay, M., & Forsyth, J. P. (2006). Act on life not on anger: The new Acceptance and Commitment Therapy guide to problem anger. Oakland, CA: New Harbinger.
- Dutch translation: Eifert, G. H., Forsyth, J., & McKay, M. (2006). Boosheid de bass: ACT: een nieuwe methode om ergernis en frustratie in de hand te houden. The Netherlands: Thema.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Dutch translation: (2010): De valstrik van het geluk. Bohn Stafleu van Loghum.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Finnish
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Finnish translation: Hayes, S. C., & Smith, S. (2008). Vapaudu mielesi vallasta ja ala elää. (Trans. Päivi and Raimo Lappalainen). Tampere, Finland: Suomen Käyttäytymistieteellinen.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- French
- Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2016). The essential guide to the ACT matrix: A step-by-step approach to Using the ACT matrix model in clinical practice. Oakland, CA: New Harbinger Publications.
- French translation: Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2017) Guide de la matrice ACT. De Boeck Sup.
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- French translation: Villatte, M., Villatte, J., & Hayes, S. C. (2019). Maîtriser la conversation clinique: Le langage en therapie. Malakoff: Dunod Editeur.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- French translation (2009): Le piège du bonheur. Montréal : Éditions de l’Homme.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- French translations: Hayes, S. C., & Smith, S. (2013). Penser moins pour etre heureux: Ici et maintenant, accepter so passé, ses peurs et sa tristesse. Paris, France: Groupe Eyrolles.
- Hayes, S. C., & Smith, S. (2019). Penser moins pour etre heureux: Vicure pleinement, ici et mainenant. Paris, France: Editions Eyrolles.
- Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2016). The essential guide to the ACT matrix: A step-by-step approach to Using the ACT matrix model in clinical practice. Oakland, CA: New Harbinger Publications.
- German
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- German translation: Hayes, S. C. (2020). Kurswechsel im Kopf: Von der Kunst anzunehmen, was ist, und innerlich frei zu werden. Beltz Verlag
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- German translation: Villatte, M., Villatte, J., & Hayes, S. C. (2020). Beherrschung der klinischen Konversation: Sprache als Intervention. Stuttgart: W. Kohlhammer GmbH.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- German translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Akzeptanz & Commitment Therapie: Achtsamkeitsbasierte Veranderungen in Theorie und Praxis (2nd edition). Paderborn, Germany: Junfermann Verlag
- Greco, L., & Hayes, S. C. (Eds.). (2008). Acceptance and mindfulness treatments for children and adolescents: A practitioner’s guide. Oakland, CA: New Harbinger.
- German translation: Greco, L., & Hayes, S. C. (Eds.). (2011). Akzeptanz und achtsamkeit in der kinder - und jugendlichenpsychotherapie. Wienheim, Germany: Beltz Verlag.
- Hayes, S. C., Strosahl, K. & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
- German translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2004). Akzeptanz- und Commitment-Therapie: Ein erlebnisorientierter Ansatz zur Verhaltensänderung. München: CIP-Medien. (transl. by Rainer F. Sonntag & Danielle Tittelbach)
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- German translation: Hayes, S. C., & Smith, S. (2007). In abstand zur inneren wortmaschine: Ein selbsthilfe- und therapiebegleitbuch aud der grundlage der Akzeptanz- und Commitment-Therapie. (Trans. G. Kluger). Tübingen, Germany: dgvt-Verlag.
- Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- German translation (2009): ACT-Training. Reihe Fachbuch, ACT für die klinische Praxis; Acceptance & Commitment Therapie: ein Handbuch. Ein Lernprogramm in zehn Schritten. Translators:Theo Kierdorf, Hildegard Höhr. (ISBN: 978-3-873877-00-9).
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Hebrew
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Hebrew translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). תרפיית קבלה ומחויבות: תהליך ועבודה מעשית ליצירת שינוי קשוב (2nd edition). Haifa, Israel: Ach Publishers.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Italian
- Luoma, J., Hayes, S. C., & Walser, R. (2017). Learning ACT: An Acceptance & Commitment Therapy skills-training manual for therapists (2nd ed). Oakland, CA: Context Press / New Harbinger Publications.
- Italian translation: Luoma, J., Hayes, S. C., & Walser, R. (2019). Il manuale del terapeuta ACT: Apprendere e allenare le abilita dell’ Acceptance & Commitment Therapy (2nd ed). Rome, Italy: Giovanni Fioriti Editore.
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Italian translation: Villatte, M., Villatte, J., & Hayes, S. C. (2020). Il dialogo clinic: Funzione, valore e centralita del linguaggio in psicoterapia. Milan: Franco Angeli.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Italian translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2013). Teoria e pratica del l'Acceptance and Commitment Therapy. (2nd edition). Translation edited by Cesare Maffei. Translators: Nidia Morra and Nicolò Gaj. Milan, Italy: Rafaello Cortina Editore.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Italian translation (2010): Hayes, S. C., & Smith, S. (2010). Smetti di Soffrire, Inizia a Vivere. (ed. IT P. Moderato trans. ACT-Italia) Milano: Franco-Angeli. Visit the ACT-Italia site for information on how to purchase this book. Translators: Ilaria Balasini, Sara Borelli, Katia Covati Katia Manduchi, Giovambattista Presti, Anna Bianca Prevedini, Elisa Rabitti, Massimo Ronchei, Francesca Scaglia, Giovanni Zucchi, Silverio Zucchi, Giovanni Miselli.
- Luoma, J., Hayes, S. C., & Walser, R. (2017). Learning ACT: An Acceptance & Commitment Therapy skills-training manual for therapists (2nd ed). Oakland, CA: Context Press / New Harbinger Publications.
- Japanese
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Japanese translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Juyō to komittomentoserapī. Suginami City, Japan: Seiwa Shoten.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Japanese translation:幸福になりたいなら幸福になろうとしてはいけない: マインドフルネスから生まれた心理療法ACT入門 (単行本) (Japanese) Tankobon Hardcover – December 17, 2015
- Greco, L., & Hayes, S. C. (Eds.). (2008). Acceptance and mindfulness treatments for children and adolescents: A practitioner’s guide. Oakland, CA: New Harbinger.
- Japanese translation: Greco, L., & Hayes, S. C. (Eds.). (2013). Shōni oyobi seinen no tame no ukeire to maindofurunesu ryōhō: jitsumu sha no tame no gaido (Translation Supervisor: T. Muto). Tokyo, Japan: Akashi Shoten.
- Bach, P., & Moran, D. (2008). ACT in practice: Case conceptualization in Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Japanese translation (2009): ACT wo jissenn-suru. (Trans. T. Muto, M. Yoshioka, K. Ishikawa, & A. Kumano) Tokyo: Seiwa-shoten. www.seiwa-pb.co.jp/
- Ramnero, J., & Torneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: Context Press / New Harbinger.
- Japanese translation (2009): Rinshou-koudou-bunnseki no ABC. (Trans. T. Muto, N. Yoneyama, & J. Tanaka-Matsumi) Tokyo: Nihon-Hyoron-sha. www.nippyo.co.jp
- Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- Japanese translation (2009): ACT wo manabu. (Trans. H. Kumano, F. Takahashi, & T. Muto) Tokyo: Seiwa-shoten. www.seiwa-pb.co.jp
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Japanese translation (2008): Anata no Jinsei wo Hajimeru tameno Workbook: Kokoro tono Atarashii Tsukiai kata, Acceptance and Commitment (Trans. T. Muto, H. Harai, M. Yoshioka, & M. Okajima). Tokyo: Brain Shuppan.
- Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004) (Eds.). Mindfulness and acceptance: Expanding the cognitive behavioral tradition. New York: Guilford Press.
- Japanese translation (2005): Maindofurunesu ando akuseputansu; Ninchikodo-ryoho no shinjigen. (Trans. by Y. Haruki, T. Muto, Y. Ito, & Y. Sugiura). Tokyo: Brain-shuppan.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Korean
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Korean translation: Villatte, M., Villatte, J., & Hayes, S. C. (in press). Imsang daehwa maseuteohagi : Gaeib-euloseoui eon-eo. Seoul: Life and Knowledge Publishing
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Korean translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2018). Acceptance and Commitment Therapy: The process and practice of mindful change. Soule, Korea: Sigma Press.
- Greco, L., & Hayes, S. C. (Eds.). (2008). Acceptance and mindfulness treatments for children and adolescents: A practitioner’s guide. Oakland, CA: New Harbinger.
- Korean translation: Greco, L., & Hayes, S. C. (Eds.). (2012). Eo-ri-ni-wa cheong-so-nyeo-neu-rwi-han su-yong mit mindfulness teu-ri-teu. Soule, Korea: Sigma Press.
- Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- Korean translation: Luoma, J., Hayes, S. C., & Walser, R. (2012). Bae-u-gi ACT. Soule, Korea: Hakjisa Publishers.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Korean translation: Hayes, S. C., & Smith, S. (2010). 마음에서 빠져나와 삶 속으로 들어가라 새 수용전념치료. Seoul: Hakjisa Publishers.
- Hayes, S. C., Strosahl, K. & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
- Korean translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2009). 수용과 참여의 심리치료. Sigmapress (translated by Moon, S-W & Kim, E.). Click here to buy this book.
- Hayes, S. C., & Strosahl, K. D. (2004) (Eds.). A practical guide to Acceptance and Commitment Therapy. New York: Springer-Verlag.
- There is a Korean translation in press from Hakjisa Publisher
- McCurry, C. (2011). Parenting your anxious child with mindfulness. Oakland, CA: New Harbinger.
- Korean translation: McCurry, C. (2011). 불안한 아이 수용과 마음챙김으로 키우기. Sigmapress (translated by Lee, S.).
- Forsyth, J. P. & Eifert, G. H. (2008). The Mindfulness and Acceptance Workbook for Anxiety Workbook: A guide to breaking free from anxiety, phobias, & worry using Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Korean translation: Forsyth, J. P. & Eifert, G. H. (2008). 마음챙김과 수용중심 불안장애 치료의 실제. Sigmapress (translated by Lee, S., Han, H., Jung, E.).
- Törneke, N. (2010). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Reno, NV: Context Press.
- Korean translation: Törneke, N. (2019). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Hakjisa (translated by Lee, S.).
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Norwegian
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Norwegian Translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2018) Aksept og verdibasert adferdsterapi (ACT) Mindfull endring - prosess og praksis. Oslo: Arneberg Forlag.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Norwegian translation: Hayes, S. C., & Smith, S. (2015). Slutt å gruble begynn å leve. Oslo: Arneberg Forlag.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Persian
- Vowles, K. E., & Sorrell, J. T. (2008). Life with chronic pain: an acceptance-based approach (therapist guide and patient workbook).
- Persian translation: Vowles, K. E., & Sorrell, J. T. (2008). زندگی با درد مزمن: رویکرد مبتنی بر پذیرش. zendegi ba darde mozmen: roykarde mobtani bar paziresh (rahnamaye darmangar va ketabe kare bimar). translated by F. Mesgarian. Tehran: Arjmand.
- Vowles, K. E., & Sorrell, J. T. (2008). Life with chronic pain: an acceptance-based approach (therapist guide and patient workbook).
- Polish
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Polish translation: Hayes S. C. (2020). Umysł Wyzwolony. Zakończ wewnętrzną walkę i żyj w zgodzie ze sobą. Sopot: Gdańskie Wydawnictwo Psychologiczne.
- Hayes, L. L., & Ciarrochi, J. (2015). The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection. Oakland, CA: New Harbinger.
- Polish translation: Hayes, L., Ciarrochi, J. (2019). TRUDNY CZAS DOJRZEWANIA. Jak pomóc nastolatkom radzić sobie z emocjami, osiągać cele i budować więzi, stosując terapię akceptacji i zaangażowania oraz psychologię pozytywną. Gdańsk: GWP.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Polish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2015). Terapia akceptacji i zaangażowania (2nd edition). Krakow, Poland: Jagiellonian University Press.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Polish translation: Hayes, S. C., & Smith, S. (2014). W pulapce mysli: Jak skutecznie poradzic sobie z depresja, stresem I lekiem. Gdansk: Gdanskie Wydawnictwo Psychologizne.
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Portuguese
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Portuguese translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2021). Terapia de aceitacao e compromisso: a processo e a practica da mundanca consciente (2a editcao). Translation edited by Sandra Maria Mallmann da Rosa. Porto Alegre, Brazil: Artmed.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Romanian
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Romanian translation: Hayes, S. C., & Smith, S. (2013). Ieși din scenariile minții și trăiește-ți viața. (Trans. K. Szabo). Lași, Romania: Editura Poliram.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Russian
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Russian translation: Hayes S. C. (2021). Освобождённый разум. Moscow: Бомбора (Bombora).
- Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- Serbian / Bosnian / Croatian / Montenegrin
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Serbian / Bosnian / Croatian / Montenegrin translation: Hayes, S. C., & Smith, S. (2017). Centar za Kongnitivno-Bohejvioralnu Terapiju. Banja Luka, Bosnia Hercegovina: My Books / Centar za kognitivno-bihejvioralnu terapiju.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Spanish
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Spanish translation: Villatte, M., Villatte, J., & Hayes, S. C. (2019). Gerente la conversación clínica: El lenguaje como intervención. Madrid: Madrid Institute of Contextual Psychology.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Spanish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Terapia de aceptacion y compromise: Proceso y practica del cambio (2nd edition). Translation edited by Ramiro Alvarez. Bilbao, Spain: Desclee de Brouwer.
- Twohig, M., & Hayes, S. C. (2008). ACT verbatim: Depression and Anxiety. Oakland, CA: New Harbinger; Reno, NV: Context Press.
- Spanish translation: Twohig, M., & Hayes, S. C. (2019). ACT en la practica clinica para le depression y la ansiedad. Bilbao, Spain: Desclee de Brouwer.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Spanish translation (2008): Las Trampas De La Felicidad. Grupo Editorial Patria.
- Harris, R. (2011). The Confidence Gap. Boston, MA: Trumpeter.
- Spanish translation (2012): Cuestión de Confianza. Santander. Sal Terrae.
- Hayes, S.C. (2005). Get Out of Your Mind and Into Your Life. Oakland, CA: New Harbinger Publications.
- Spanish translation (May 2013): Sal de tu mente, entra en tu vida. Bilbao. Desclée de Brouwer.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Spanish translation (2014) Terapia de aceptacion y compromise: Proceso y practica del cambio (2nd edition). Translation edited by Ramiro Alvarez. Bilbao, Spain: Desclee de Brouwer.
- Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- Swedish
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
- Swedish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). ACT – Acceptance and Commitment Therapy i teori och tillamping: Vagen till psykologisk flexibilitet (2nd edition). Stockholm, Sweden: Natur Och Kulture.
- Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Swedish translation: Hayes, S. C., & Smith, S. (2007). Sluta grubbla Borja leva. (Trans. A. Ghaderi). Stockholm: Natur och Kultur.
- Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Swedish translation: (2009): Lykofallan. Stockholm, Sweden.
- Hayes, S.C., Strosahl, K.D., Wilson, K.G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (second edition). New York: The Guilford Press.
Translated ACT Books by English Title
Translations of Hayes, S. C. (2019). A liberated mind: How to pivot toward what matters. New York: Penguin/Avery.
- German Translation: Hayes, S. C. (2020). Kurswechsel im Kopf: Von der Kunst anzunehmen, was ist, und innerlich frei zu werden. Beltz Verlag.
- Polish Translation: Hayes S. C. (2020). Umysł Wyzwolony. Zakończ wewnętrzną walkę i żyj w zgodzie ze sobą. Sopot: Gdańskie Wydawnictwo Psychologiczne.
- Russian Translation: Hayes S. C. (2021). Освобождённый разум. Moscow: Бомбора (Bombora).
Translations of Luoma, J., Hayes, S. C., & Walser, R. (2017). Learning ACT: An Acceptance & Commitment Therapy skills-training manual for therapists (2nd ed). Oakland, CA: Context Press / New Harbinger Publications.
- Italian translation: Luoma, J., Hayes, S. C., & Walser, R. (2019). Il manuale del terapeuta ACT: Apprendere e allenare le abilita dell’ Acceptance & Commitment Therapy (2nd ed). Rome, Italy: Giovanni Fioriti Editore.
Translations of Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2016). The essential guide to the ACT matrix: A step-by-step approach to Using the ACT matrix model in clinical practice. Oakland, CA: New Harbinger Publications.
- French translation: Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. O. (2017) Guide de la matrice ACT. De Boeck Sup.
Translations Villatte, M., Villatte, J., & Hayes, S. C. (2015). Mastering the clinical conversation: Language as intervention. New York: Guilford.
- French translation: Villatte, M., Villatte, J., & Hayes, S. C. (2019). Maîtriser la conversation clinique: Le langage en therapie. Malakoff: Dunod Editeur.
- German translation: Villatte, M., Villatte, J., & Hayes, S. C. (2020). Beherrschung der klinischen Konversation: Sprache als Intervention. Stuttgart: W. Kohlhammer GmbH.
- Italian translation: Villatte, M., Villatte, J., & Hayes, S. C. (2020). Il dialogo clinic: Funzione, valore e centralita del linguaggio in psicoterapia. Milan: Franco Angeli.
- Korean translation: Villatte, M., Villatte, J., & Hayes, S. C. (in press). Imsang daehwa maseuteohagi : Gaeib-euloseoui eon-eo. Seoul: Life and Knowledge Publishing.
- Spanish translation: Villatte, M., Villatte, J., & Hayes, S. C. (2019). Gerente la conversación clínica: El lenguaje como intervención. Madrid: Madrid Institute of Contextual Psychology.
Translations of Hayes, L. L., & Ciarrochi, J. (2015). The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection. Oakland, CA: New Harbinger.
- Polish translation: Hayes, L., Ciarrochi, J. (2019). TRUDNY CZAS DOJRZEWANIA. Jak pomóc nastolatkom radzić sobie z emocjami, osiągać cele i budować więzi, stosując terapię akceptacji i zaangażowania oraz psychologię pozytywną. Gdańsk: GWP.
Translations of Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance and Commitment Therapy: The process and practice of mindful change (2nd edition). New York: Guilford Press.
- Dutch translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance en Commitment Therapie: Veranderingen door mindfulness, het process en de praktijk. (2nd edition). Amsterdam: Pearson Education Publishers.
- Danish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2013). Acceptance en Commitment Therapy: Psykologisk fleksibilitet og mindfulnessprocessor (2nd edition). Translator: Bjorn Nake. Copenhagen, Denmark: Hans Reitzel Publishers).
- Italian translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2013). Teoria e pratica del l'Acceptance and Commitment Therapy. (2nd edition). Translation edited by Cesare Maffei. Translators: Nidia Morra and Nicolò Gaj. Milan, Italy: Rafaello Cortina Editore.
- Spanish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Terapia de aceptacion y compromise: Proceso y practica del cambio (2nd edition). Translation edited by Ramiro Alvarez. Bilbao, Spain: Desclee de Brouwer.
- Swedish translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). ACT – Acceptance and Commitment Therapy i teori och tillamping: Vagen till psykologisk flexibilitet (2nd edition). Stockholm, Sweden: Natur Och Kulture.
- German translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2014). Akzeptanz & Commitment Therapie: Achtsamkeitsbasierte Veranderungen in Theorie und Praxis (2nd edition). Paderborn, Germany: Junfermann Verlag;
- Norwegian translation: Hayes, S. C., Strosahl, K., & Wilson, K. G. (2018) Aksept og verdibasert adferdsterapi (ACT) Mindfull endring - prosess og praksis. Oslo: Arneberg Forlag.
- Japanese translation: (Suginami City, Japan: Seiwa Shoten
- Chinese translation
- Polish translation: (Krakow, Poland: Jagiellonian University Press)
- Hebrew translation: (Haifa, Israel: Ach Publishers)
- Korean translation: (Soule, Korea: Sigma Press)
- Portuguese translation: (Porto Alegre, Brazil: Artmed)
Translations of Hayes, S. C., Strosahl, K. & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
- German translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2004). Akzeptanz- und Commitment-Therapie: Ein erlebnisorientierter Ansatz zur Verhaltensänderung. München: CIP-Medien. (transl. by Rainer F. Sonntag & Danielle Tittelbach)
- Dutch translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2006). ACT. Een experiëntiële weg naar gedragsverandering. Nederlandse bewerking (trans. By Ando Rokx). ISBN 90 265 1758 0 Verschijnt zomer 2006 Prijs: C.a. € 50, -
- Korean translation: Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2009). 수용과 참여의 심리치료. Sigmapress (translated by Moon, S-W & Kim, E.). Click here to buy this book.
Translations of Hayes, S. C., & Strosahl, K. D. (2004) (Eds.). A practical guide to Acceptance and Commitment Therapy. New York: Springer-Verlag.
- There is a Korean translation in press from Hakjisa Publisher
- Japanese translation (in press). Akashi Shoten Co.
Translations of Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004) (Eds.). Mindfulness and acceptance: Expanding the cognitive behavioral tradition. New York: Guilford Press.
- Dutch translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2006). Mindfullnes en acceptatie. De derde generatie gedragstherapie . (Trans. By Ando Rokx). Nederlandse bewerking. ISBN 90 265 1759 9 Verschijnt zomer 2006 Prijs: C.a. € 50, -
- Japanese translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (2005.) Maindofurunesu ando akuseputansu; Ninchikodo-ryoho no shinjigen. (Trans. by Y. Haruki, T. Muto, Y. Ito, & Y. Sugiura). Tokyo: Brain-shuppan.
- Korean translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2005.) Mindfulness and acceptance: Expanding the cognitive behavioral tradition. Seoul: Meditation Counseling Research Institute. [2009]
- Chinese translation: Hayes, S. C., Follette, V. M., & Linehan, M. M. (Eds.). (2005.) Mindfulness and acceptance: Expanding the cognitive behavioral tradition. Shanghi: Ewen Publishers. [2011]
Translations of Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger. (Winner of the Association for Behavioral and Cognitive Therapies Self-Help Book of Merit Award, 2010)
- Danish translation: Hayes, S. C., & Smith, S. (2008). Slip tanketyrraniet – tag fat på livet. (Trans. T. Bøgeskov). Copenhagen: Dansk Psykologisk Forlag.
- Dutch translation: Hayes, S. C., Smith, S. (2006). Uit je hoofd, in het leven. Een werkboek voor een waardevol leven met mindfulness en Acceptatie en Commitment Therapie. (Trans. A. Rokx). Amsterdam: Uitgeverij Nieuwezijds.
- Finnish translation: Hayes, S. C., & Smith, S. (2008). Vapaudu mielesi vallasta ja ala elää. (Trans. Päivi and Raimo Lappalainen). Tampere, Finland: Suomen Käyttäytymistieteellinen.
- German translation: Hayes, S. C., & Smith, S. (2007). In abstand zur inneren wortmaschine: Ein selbsthilfe- und therapiebegleitbuch aud der grundlage der Akzeptanz- und Commitment-Therapie. (Trans. G. Kluger). Tübingen, Germany: dgvt-Verlag.
- Italian translation (2010): Hayes, S. C., & Smith, S. (2010). Smetti di Soffrire, Inizia a Vivere. (ed. IT P. Moderato trans. ACT-Italia) Milano: Franco-Angeli. www.act-italia.org
- French translation: Hayes, S. C., & Smith, S. (2013). Penser Moins pour etre heureux: Ici et maintenant, accepter so passé, ses peurs et sa tristesse. Paris, France: Groupe Ayrolles.
- Chinese translation: Hayes, S. C., & Smith, S. (2010). Zǒuchū nǐ de tàidù, zài nǐ de shēnghuó: Xīn Acceptance and Commitment Therapy. Chongqing, China: Chongqing University Press.
- Korean translation: Hayes, S. C., & Smith, S. (2010). 마음에서 빠져나와 삶 속으로 들어가라 새 수용전념치료. Seoul: Hakjisa Publishers.
- Japanese translation: Hayes, S. C., & Smith, S. (2008). Anata no Jinsei wo Hajimeru tameno Workbook: Kokoro tono Atarashii Tsukiai kata, Acceptance and Commitment (Trans. T. Muto, H. Harai, M. Yoshioka, & M. Okajima). Tokyo: Brain Shuppan.
- Second Japanese translation: Hayes, S. C., & Smith, S. (2010). Anata no Jinsei wo Hajimeru tameno Workbook: Kokoro tono Atarashii Tsukiai kata, Acceptance and Commitment (Trans. T. Muto, H. Harai, M. Yoshioka, & M. Okajima). Tokyo: Seiwa Shoten Publishers.
- Swedish translation: Hayes, S. C., & Smith, S. (2007). Sluta grubbla Borja leva. (Trans. A. Ghaderi). Stockholm: Natur och Kultur.
- Romanian translation: Hayes, S. C., & Smith, S. (2013). Ieși din scenariile minții și trăiește-ți viața. (Trans. K. Szabo). Lași, Romania: Editura Poliram.
- Bosnian translation: Hayes, S. C., & Smith, S. (in press). Centar za Kongnitivno-Bohejvioralnu Terapiju.
- Croatian translation: Hayes, S. C., & Smith, S. (in press). Centar za Kongnitivno-Bohejvioralnu Terapiju.
- Montenegrin translation: Hayes, S. C., & Smith, S. (in press). Centar za Kongnitivno-Bohejvioralnu Terapiju.
- Serbian translation: Hayes, S. C., & Smith, S. (in press). Centar za Kongnitivno-Bohejvioralnu Terapiju.
- Polish translation: Hayes, S. C., & Smith, S. (n press). Gdansk: Gdanskie Wydawnictwo Psychologizne.
- Spanish translation: Hayes, S. C., & Smith, S. (2013). Sal de tu mente entra en tu vida: La nueva Terapia de Aceptación y Compromiso. Bilbao, Spain: Editorial Desclée De Brouwer.
- For the visually impaired (or just those who like audio books) there is an Audio book version: New York: Tantor Audio (2012)
Translation of Eifert, G. H., McKay, M., & Forsyth, J. P. (2006). Act on life not on anger: The new Acceptance and Commitment Therapy guide to problem anger. Oakland, CA: New Harbinger.
- Dutch translation: Eifert, G. H., Forsyth, J., & McKay, M. (2006). Boosheid de bass: ACT: een nieuwe methode om ergernis en frustratie in de hand te houden. The Netherlands: Thema.
Translation of Harris, R. (2008). The Happiness Trap: How to stop struggling and start living. Boston, MA: Trumpeter.
- Spanish translation (2008): Las Trampas De La Felicidad. Grupo Editorial Patria.
- Chinese translation: 羅斯.哈里斯(2009)。快樂是一種陷阱。台北:張老師文化。
- French translation: (2009): Le piège du bonheur. Montréal : Éditions de l’Homme.
- Japanese translation: 幸福になりたいなら幸福になろうとしてはいけない: マインドフルネスから生まれた心理療法ACT入門 (単行本) (Japanese) Tankobon Hardcover – December 17, 2015
- Dutch translation: (2010): De valstrik van het geluk. Bohn Stafleu van Loghum.
- Swedish translation: (2009): Lykofallan. Stockholm, Sweden.
Translation of Harris, R. (2011). The Confidence Gap. Boston, MA: Trumpeter.
- Spanish translation (2012): Cuestión de Confianza. Santander. Sal Terrae.
Translations of Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists. Oakland, CA: New Harbinger & Reno, NV: Context Press.
- German translation (2009): ACT-Training. Reihe Fachbuch, ACT für die klinische Praxis; Acceptance & Commitment Therapie: ein Handbuch. Ein Lernprogramm in zehn Schritten. Translators:Theo Kierdorf, Hildegard Höhr. (ISBN: 978-3-873877-00-9).
- Japanese translation (2009): ACT wo manabu. (Trans. H. Kumano, F. Takahashi, & T. Muto) Tokyo: Seiwa-shoten. www.seiwa-pb.co.jp
- Dutch translation: Luoma, J., Hayes, S. C., & Walser, R. (2009). Leer ACT. Vaardigheden voor therapeuten (Trans. L. Berkhuizen, P. van der Kaaij, & J. A-Tjak). Houten, The Netherlands: Bohn Stafleu van Loghum.
- Korean translation: Luoma, J., Hayes, S. C., & Walser, R. (20012). Bae-u-gi ACT. Soule, Korea: Hakjisa Publishers.
Translations of Bach, P., & Moran, D. (2008). ACT in practice: Case conceptualization in Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Japanese translation (2009): ACT wo jissenn-suru. (Trans. T. Muto, M. Yoshioka, K. Ishikawa, & A. Kumano) Tokyo: Seiwa-shoten. www.seiwa-pb.co.jp
- Chinese translation: 帕特里夏·A.巴赫(Patricia A.Bach)、(美國)丹尼爾·J.莫蘭(2011)。接受與實現療法:理論與實務。重慶:重慶大學出版社
Translation of Ramnero, J., & Torneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: Context Press / New Harbinger.
- Japanese translation (2009): Rinshou-koudou-bunnseki no ABC. (Trans. T. Muto, N. Yoneyama, & J. Tanaka-Matsumi) Tokyo: Nihon-Hyoron-sha. www.nippyo.co.jp
Translations of Hayes, S. C., Barnes-Holmes, D., & Roche, B. (2001). Relational Frame Theory: A Post-Skinnerian account of human language and cognition. New York: Plenum Press.
- Japanese translation: Hayes, S. C., Barnes-Holmes, D., & Roche, B. (2009). Relational Frame Theory: A Post-Skinnerian account of human language and cognition. Tokyo: Seiwa Shoten.
Translation of Forsyth, J. P. & Eifert, G. H. (2008). The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy. Oakland, CA: New Harbinger.
- Chinese translation: 約翰.福賽思(John.P.Forsyth)、格奧爾格.艾弗特(Georg H.Eifert)(2010)。晚安,我的不安:緩解焦慮自助手冊。四川:四川人民出版社。
Translation of Robinson, P. J. & Strosahl, K. D. (2008). The Mindfulness and Acceptance Workbook for Depression. Oakland, CA: New Harbinger.
- Chinese translation: 科尔克.斯特尔萨拉,派翠西娅.罗宾逊(2010)。抑郁的自我疗法:用接受与实现疗法走出抑郁。华东:华东师范大学出版社。
Examples of Books on ACT and RFT
Examples of Books on ACT and RFTThis is a partial list as of 2014
General ACT Books: Professionals
Luoma, J., Hayes, S. C. & Walser, R. (2007). Learning ACT. Oakland, CA: New Harbinger. [A step by step learning companion for the main ACT book below. Very practical and helpful]
Hayes, S. C., Strosahl, K., & Wilson, K. G. (2012). Acceptance and Commitment Therapy: The process and practice of mindful change (2nd edition). New York: Guilford Press. [This is still the heart of the ACT literature. It is where it started]
Wilson, K. G. & Dufrene, T. (2009). Mindfulness for two: An Acceptance and Commitment Therapy approach to mindfulness in psychotherapy. Oakland, CA: New Harbinger. [A book on ACT that emphasizes mindfulness and the therapeutic relationship]
Hayes, S. C. & Strosahl, K. D. (2005). A Practical Guide to Acceptance and Commitment Therapy. New York: Springer-Verlag. [Shows how to do ACT with a variety of populations]
Twohig, M., & Hayes, S. C. (2008). ACT verbatim: Depression and Anxiety. Oakland, CA: New Harbinger; Reno, NV: Context Press. [Good example of ACT in actual practice]
Chantry, D. (2007). Talking ACT: Notes and conversations on Acceptance and Commitment Therapy. Reno, NV: Context Press. [This is an edited version of the ACT listserv from July 2002 through August 2005 compiled by a therapist, for therapists. Functions as a quick reference on a wide range of ACT topics (acceptance, anxiety, behavior analysis, choice, clinical resources, contextualism, etc)]
Ciarrochi, J. V. & Bailey, A. (2008). A CBT practitioner’s guide to ACT. Oakland, CA: New Harbinger. [Does what the title says it does]
Batten, S. (2011). Essentials of Acceptance and Commitment Therapy. London: Sage. [Broad introduction to ACT]
Harris, R. (2009). ACT made simple. Oakland, CA: New Harbinger. [Easy place to start with ACT]
Hayes, S. C. & Lillis, J. (2012). Introduction to Acceptance and Commitment Therapy. Washington, DC: American Psychological Association. [Books specifically for students learning about ACT]
General ACT Books: Clients
Hayes, S. C. & Smith, S. (2005). Get out of your mind and into your life. Oakland, CA: New Harbinger. [A general purpose ACT workbook. RCTs show that it works as an aid to ACT or on its own, but it will also keep new ACT therapists well oriented]
Harris, R. (2008). The happiness trap. New York: Shambala. [Very accessible ACT book for the public]
Trauma: Professional book
Walser, R., & Westrup, D. (2007). Acceptance & Commitment Therapy for the Treatment of Post-Traumatic Stress Disorder & Trauma-Related Problems: A Practitioner's Guide to Using Mindfulness & Acceptance Strategies. Oakland, CA: New Harbinger. [A very practical and accessible approach to using ACT to treat post-traumatic stress disorder (PTSD) and acute trauma-related symptoms.]
Trauma: Client book
Follette, V. M., & Pistorello, J. (2007). Finding Life Beyond Trauma: Using Acceptance and Commitment Therapy to Heal from Post-Traumatic Stress and Trauma-Related Problems. Oakland, CA: New Harbinger. [Applies the principles of ACT to help readers cope with the after effects of traumatic experience. Straightforward, practical, and useful]
Depression: Professional book
Zettle, R. (2007). ACT for Depression: A Clinician's Guide to Using Acceptance & Commitment Therapy in Treating Depression. Oakland, CA: New Harbinger. [An solid book from one of the founders of ACT on one of the most pervasive problems human beings face.]
Depression: Client book
Strosahl, K. & Robinson, P. J. (2008). The Mindfulness & Acceptance Workbook for Depression: Using Acceptance & Commitment Therapy to Move Through Depression & Create a Life Worth Living. Oakland: New Harbinger. [Great workbook on ACT for depression]
Anxiety: Professional book
Eifert, G. & Forsyth, J. (2005). Acceptance and Commitment Therapy for anxiety disorders. Oakland: New Harbinger. [Good book with a protocol that shows how to mix ACT processes into a brief therapy for anxiety disorders].
Anxiety: Client book
Forsyth, J., & Eifert, G. (2007). The Mindfulness and Acceptance Workbook for Anxiety: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy. Oakland: New Harbinger. [Solid workbook for anxiety]
Worry: Client book
Lejeune, C. (2007). The Worry Trap: How to Free Yourself from Worry & Anxiety using Acceptance and Commitment Therapy. Oakland, CA: New Harbinger. [A guide to the application of ACT to worry and generalized anxiety.]
Chronic pain: Professional books
Dahl, J., Wilson, K. G., Luciano, C., & Hayes, S. C. (2005). Acceptance and Commitment Therapy for Chronic Pain. Reno, NV: Context Press. [Describes an ACT approach to chronic pain. Very accessible and readable. One of the better clinical expositions on how to do ACT values work.]
McCracken, L. M. (2005). Contextual Cognitive-Behavioral Therapy for chronic pain. Seattle, WA: International Association for the Study of Pain. [[Describes an interdisciplinary ACT-based approach to chronic pain
Chronic pain: Client book
Dahl, J. C., & Lundgren, T. L. (2006). Living Beyond Your Pain: Using Acceptance and Commitment Therapy to Ease Chronic Pain. Oakland, CA: New Harbinger. [Uses ACT principles to help those suffering from pain transcend the experience by reconnecting with other, more valued aspects of their lives.]
Anger: Client book
Eifert, G. H., McKay, M., & Forsyth, J. P. (2006). ACT on life not on anger: The new Acceptance and Commitment Therapy guide to problem anger. Oakland, CA: New Harbinger. [The first book to adapt ACT principles to dealing with anger. It teaches readers how to change their relationship to anger by accepting rather than resisting angry feelings and learning to make values-based responses to provocation. Has been tested successfully in a small randomized trial.]
Caregivers: Client book
McCurry, S. M. (2006). When a family member has dementia: Steps to becoming a resilient caregiver. Westport, CT: Praeger Publishers. [Although not directly on ACT or mindfulness, this book for caregivers does include a significant emphasis on acceptance, as might make sense given that the author is on of the early ACT therapists from UNR.]
Eating disorders: Client book
Heffner, M., & Eifert, G. H. (2004). The anorexia workbook: How to accept yourself, heal suffering, and reclaim your life. Oakland, CA: New Harbinger. [An eating disorders patient workbook on ACT.]
Diabetes management: Client book
Gregg, J., Callaghan, G., & Hayes, S. C. (2007). The diabetes lifestyle book: Facing your fears and making changes for a long and healthy life. Oakland, CA: New Harbinger. [You cannot tell from the title but this is a book applying ACT to diabetes management.]
Organizational issues: Professional book
Hayes, S. C., Bond, F. W., Barnes-Holmes, D., & Austin, J. (2007). Acceptance and Mindfulness at Work: Applying Acceptance and Commitment Therapy and Relational Frame Theory to Organizational Behavioral Management. Binghamton, NY: Haworth Press. [This was a special issue of the Journal of Organizational Behavior Management that was bound into book form. Don't buy it expecting a smooth presentation of the applicability of ACT and RFT to organizational issues -- it is a collection of journal articles gather into a book. But it is still worthwhile if I/O is your area and you are wondering how ACT and RFT might apply.]
Human performance: Professional book
Gardner, F.L., & Moore, Z.E. (2007). The psychology of enhancing human performance: The Mindfulness-Acceptance-Commitment (MAC) approach. New York: Springer.
[This book provides theory and empirical background, and a structured step-by-step, protocol for the assessment, conceptualization, and enhancement of human performance with a variety of high-performing clientele including executives, athletes, artists, and emergency/military personnel].
Trichotillomania: Professional book
Woods, D. W., & Twohig, M. P. (2008). Trichotillomania: An ACT-enhanced Behavior Therapy Approach Therapist Guide. New York: Oxford University Press.
Trichotillomania: Client book
Woods, D. W., & Twohig, M. P. (2008). Trichotillomania: An ACT-enhanced Behavior Therapy Approach Workbook. New York: Oxford University Press.
Behavioral Medicine: Professional book
McCracken, L. (2011). Mindfulness and Acceptance in Behavioral Medicine. Oakland, CA: New Harbinger.
Assessment: Professional book
Baer, R. (2010). Assessing Mindfulness & Acceptance Processes in Clients: Illuminating the Theory & Practice of Change. Oakland, CA: New Harbinger.
Primary care settings: Professional book
Robinson, P. J., Gould, D. A., & Strosahl, K. D. (2011). Real behavior change in primary care. Oakland, CA: New Harbinger.
Irritable Bowel Syndrome: Client book
Ferreira, N. B. & Gillanders, D. T (2012) Better Living with IBS: A step-by-step program to managing your symptoms so you can enjoy life to the full! Exsile Publishing, New South Wales.
Psychosis: Professional book
Morris, E. M. J., Johns, L. C., & Oliver, J. E. (2013) (Eds). Acceptance and Commitment Therapy and mindfulness for psychosis. London: Wiley-Blackwell. ISBN: 978-1-1199-5079-0
Sleep: Client book
Meadows, G. (2014). The sleep book: How to sleep well every night. London, UK: Orion.
Persian
PersianThis list is no longer being updated. Please click here for a list of ACT Books in 20+ Languages.
Vowles, K. E., & Sorrell, J. T. (2008). Life with chronic pain: an acceptance-based approach (therapist guide and patient workbook).
Persian translation: Vowles, K. E., & Sorrell, J. T. (2008). زندگی با درد مزمن: رویکرد مبتنی بر پذیرش. translated by F. Mesgarian. Tehran: Arjmand.
Original Non-English ACT Books
Original Non-English ACT BooksThis list is no longer being updated. Please click here for a list of ACT Books in 20+ Languages.
Original Non-English ACT Books
- Danish (Dansk)
- Grønlund, C. & Møller Rasmussen, S. (2015). Rundt om ACT : muligheder og metode i acceptance and commitment therapy. Frydenlund.
- This first Danish-written anthology on ACT (Acceptance and Commitment Therapy) goes in depth with the method's many application possibilities - seen through the eyes of Danish therapists.
- Ramussen, S. & Taggaard Nielsen, O. (2010). Introduktion til ACT. Copenhagen: Dansk Psykologisk Forlag.
- Grønlund, C. & Møller Rasmussen, S. (2015). Rundt om ACT : muligheder og metode i acceptance and commitment therapy. Frydenlund.
- Dutch (Nederlandstalig)
- A-Tjak, J., & De Groot, F. (Eds.). (2008) . Acceptance and commitment therapy: Een inleiding voor hulpverleners. Houten: Bohn Stafleu van Loghum. (ISBN 978 90 313 5894 6. NUR 777)
- An original edited volume about ACT.
- Jansen, G. (2006). Denk wat I wilt doe wat I droomt: op weg naar waardevol leven. Amsterdam: Uitgeverij Nieuwezijds.
- An ACT-related book in Dutch. Some discussion between ACT and Cognitive Therapy in this book, but it is not possible to make such discrimination out of a language community. The book definitely puts a number of ACT concepts forward for consideration.
- A-Tjak, J., & De Groot, F. (Eds.). (2008) . Acceptance and commitment therapy: Een inleiding voor hulpverleners. Houten: Bohn Stafleu van Loghum. (ISBN 978 90 313 5894 6. NUR 777)
- Finnish (Suomi)
- Lappalainen, R., Lehtonen, T., Hayes, SC, Batten, S., Gifford, E., Wilson, K.G., Afari, N., & McCurry, S.M. (2004). Hyväksymis- ja omistautumisterapia käytännön terapiatyössä (Applying Acceptance and Commitment Therapy (ACT): A Clinical Manual). Tampere, Finland: Suomen Käyttäytymistieteellinen Tutkimuslaitos (The Finnish Institute for Behavioral Science).
- An ACT clinical manual in Finnish.
- Lappalainen, R., Lehtonen, T., Hayes, SC, Batten, S., Gifford, E., Wilson, K.G., Afari, N., & McCurry, S.M. (2004). Hyväksymis- ja omistautumisterapia käytännön terapiatyössä (Applying Acceptance and Commitment Therapy (ACT): A Clinical Manual). Tampere, Finland: Suomen Käyttäytymistieteellinen Tutkimuslaitos (The Finnish Institute for Behavioral Science).
- French (Français)
- Dionne, F., & Veillette, J. (2021). Apprivoiser la douleur chronique avec ACT: un guide de pratique en 10 modules. Paris, France : Dunod.
- La douleur chronique constitue un enjeu de santé publique important et pose plusieurs défis cliniques et personnels pour le praticien. La thérapie d’acceptation et d’engagement (ACT, Acceptance and Commitment Therapy) propose des stratégies thérapeutiques originales et efficaces pour améliorer la qualité de vie des gens souffrant de cette problématique.
- Son objectif n’est pas de modifier les symptômes, mais de faire évoluer le rapport du patient à leur égard, de la lutte vers l’acceptation active de la douleur, et l’engagement dans des activités en cohérence avec ses valeurs personnelles.
- Monestès, J. L. (2010). Changer grâce à Darwin. La théorie de votre évolution. Paris: Odile Jacob.
- Darwin nous a appris comment l’évolution avait façonné notre espèce. Mais sa théorie peut aussi être utile à chacun d’entre nous au quotidien !
- Cet ouvrage explique comment les mécanismes naturels qui ont fait leur preuve pour l’espèce humaine peuvent aider chacun de nous à évoluer dans sa vie : nous pouvons favoriser une sélection de nos comportements, et ne plus laisser le hasard gérer notre destin.
- Il propose de nombreux outils pratiques fondés sur la thérapie d’acceptation et d’engagement et les thérapies cognitives et comportementales : dépasser les obstacles au changement, créer de la variation, développer sa curiosité au monde, mais aussi, quand il le faut, accepter les choses comme elles viennent, ne rien changer, cesser de vouloir contrôler l’incontrôlable….
- Un « darwinisme personnel » pour faciliter votre propre évolution !
- This book presents a selectionist approach of behaviors. It proposes advice and tools to commit in direction of values and to walk through acceptance, by using concepts from Darwinism and ACT.
- Schoendorff, B. (2009). Faire Face à la Souffrance, Choisir la vie plutôt que la lutte avec la Thérapie d'Acceptation et d'Engagement.
- The first book on ACT in French. It is a bibliotherapy book based in part on the I-view model of Kevin Polk and Jerold Hambright.
- This is the first book on ACT in French. It's a self-help book based on Kevin Polk and Jerold Hambright's I-view.
- Monestès, J. L. (2009). Faire la paix avec son passé. Paris: Odile Jacob.
- Nos souvenirs, particulièrement les plus douloureux, nous incitent à la lutte pour éviter leur réapparition. Ce livre sur la mémoire développe de nombreux concepts de l’ACT et les applique aux souvenirs des événements que nous aurions préféré ne pas vivre.
- It is our natural tendency to struggle when we are confronted to hurting memories. We would prefer to erase them if we could. This book on memory uses ACT concepts to deal with memories of events we would rather not have lived.
- Dionne, F., & Veillette, J. (2021). Apprivoiser la douleur chronique avec ACT: un guide de pratique en 10 modules. Paris, France : Dunod.
- German (Deutsch)
- Wengenroth, M. (2008). Das Leben annehmen. So hile die Akzeptanz- und Commitmenttherapie (ACT). Bern, Germany: Huber.
- An original German, ACT-based self-help book. Very good buzz about this book by ACT experts.
- Wengenroth, M. (2008). Das Leben annehmen. So hile die Akzeptanz- und Commitmenttherapie (ACT). Bern, Germany: Huber.
- Polish (Polish)
- Baran, L., Hyla, M., Kleszcz, B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego.
- Portuguese (Português)
- Saban, M. T. (2015). Introdução à Terapia de Aceitação e Compromisso. Belo Horizonte: Ed. Artesã.
- Lucena-Santos, P., Pinto-Gouveia, J., & Oliveira, MS (Eds.) (2015). Terapias Comportamentais of Terceira Geração: Guia para profissionais. Novo Hamburgo: Sinopsys Editora
- An original book including but not limited to ACT. Specifically, this book is a professional guide on third-wave behavioral therapies (Mindfulness-based Cognitive Therapy, Functional Analytic Psychotherapy, Behavioral Activation Therapy, Behavioral Activation, Mindfulness-Based Stress Reduction and Compassion Focused Therapy)
- Boavista, R. (2012). Terapia of Aceitação e Compromisso (ACT): Purpose uma possibilidade para a clínica comportamental. Santo André: ESETec Editores Associados.
- In this book Rodrigo RC Boavista does a book review that contemplates philosophical assumptions, theoretical foundations, model of psychopathology and a few application scenarios of the ACT therapeutic approach.
- Japanese (日本語)
- Muto, T. (Ed.) (2017). 55歳からのアクセプタンス&コミットメント・セラピー(ACT)超高齢化社会のための認知行動療法の新展開 [Turning 55 years old in super-aging society: Living oldness with Acceptance and Commitment Therapy]. Kyoto: Ratik.
- Kumano, H. & Muto, T. (Eds.) (2009). Tokushuu-gou: Akuseputansu ando komittoment serapi. in the “Kokoro-no-Rinshou a la carte” Magazine for clinicians. Tokyo: Seiwa-shoten.
- Title translation: Special volume: Acceptance and Commitment Therapy.
- Kumano, H. (2009). 21 seiki no jibun sagashi project: kara no ori kara dete, machi ni dekakeyou. Tokyo: Sanga.
- Title translation: The “Pursuit of myself” project in 21 century: Breaking the prison of conceptualized myself.
- Muto, T. (Eds.) (2006). Akuseputansu ando komittoment serapi no bunmyaku: Rinshou-kudu-bunseki no maindofuru-na tenkai. Tokyo: Brain-shuppan.
- Title: Some contexts of Acceptance and Commitment Therapy: Mindfulness in Clinical Behavior Analysis .
- Korean (조선말, 한국어)
- Lee, Seonyoung (2017). 꼭 알고 싶은 수용-전념 치료의 모든 것: ACT와 친해지기. Soulmate. Seoul.
- Spanish (Español)
- García Higuera, JA (2007). Curso Teraperutico de Aceptación I y II. Madrid: Paradox.
- An ACT self help book with lots of exercises.
- Barraca, J. (Ed.). (2005). The mente o la vida. An aproximation to the Terapia of Acceptance and Compromise. Bilbao: Desclée de Brouwer.
- An original edited ACT book in Spanish.
- Wilson, KG, & Luciano, C. (2002). Acceptance and Commitment Therapy: A behavioral treatment focused on values. Madrid: Pirámide.
- An original ACT book in English ACT authors.
- García Higuera, JA (2003). Terapia psicológica en el tartamudeo, from Van Riper to the terapia of acceptance and compromiso.Barcelona: Editorial Ariel. Visit this site web para más información.
- An ACT book dedicated to stuttering and its psychological treatment.
- Luciano, C. (Ed.). (2001). Terapia of Acceptance and Compromise (ACT) and the Traastorno de Evitación Experiencial. A síntesis of casinos clinics. (Ed.) Valencia: Promolibro.
- An original ACT book in Spanish with a series of very creative single case studies.
- García Higuera, JA (2007). Curso Teraperutico de Aceptación I y II. Madrid: Paradox.
Samtaler som forandrer - behandlerens guide til ACT i teori og praksis
Samtaler som forandrer - behandlerens guide til ACT i teori og praksisDrømmer du om at lære de effektive, evidensbaserede og håndgribelige strategier, som skaber vilde og varige forandringer for dine klienter og for dig selv? Samtaler som forandrer er behandlerens guide til ACT i teori og praksis. Bogen er skrevet af Rikke Kjelgaard, en af Danmarks største kapaciteter inden for ACT (Acceptance and Commitment Therapy). Her får du som behandler en grundig introduktion til ACT med masser af kliniske eksempler og øvelser. Du bliver præsenteret for de grundlæggende begreber og for modellens bærende principper. Du får en gennemgang af kerneprocesserne i ACT samt eksempler på, hvordan disse processer udspiller sig i det terapeutiske møde. Du følger med i en række samtaler som netop demonstrerer kerneprocesserne. Du lærer at lave sagskonceptualisering, at skabe fleksibilitetsprofiler, og du lærer, hvordan du designer dine egne metaforer. Du får desuden en række generelle tips til, hvad du skal gøre – og hvad du skal undgå at gøre – for at skabe samtaler, som forandrer.
Self-Help Books in Non-English Languages
Self-Help Books in Non-English LanguagesThis list is no longer being updated. Please click here for a list of ACT Books in 20+ Languages.
Original Non-English Self-Help Books
German
- Waadt, M. (Author),& Acker, J. (2018). Das Selbsthilfebuch gegen Burnout: Mit Akzeptanz und Achtsamkeit den Teufelskreis durchbrechen. Berne, CHE: Hogrefe AG.
- Wengenroth, M. (2008). Das Leben annehmen. So hilft die Akzeptanz- und Commitmenttherapie (ACT). Bern, Germany: Huber.
Danish
- Ramussen, S. & Taggaard Nielsen, O. (2010) Introduktion til ACT. Copenhagen: Dansk Psykologisk Forlag. 2nd printing (2012).
Dutch
- Bohlmeijer, E., & Hulsbergen, M. (2009). Voluit leven. Amsterdam, NLD: Boom.
French
Schoendorff, B. (2009). Faire face à la souffrance, choisir la vie plutôt que la lutte avec la Thérapie d'Acceptation et d'Engagement. Paris: Retz.
Le premier livre sur l'ACT en français. C'est un ouvrage de bibliothérapie qui se base en partie sur le modèle I-view de Kevin Polk et Jerold Hambright.
Portuguese
- Bittar, E. (2011). Nao sou feliz … e agora? O que fazer quando todas as formulas fracassem? Uberlândia, Brazil: Imagine.
Spanish
García Higuera, J. A. (2007).Curso Terapéutico de Aceptación I y II. Madrid: Paradox.
An ACT self help book with 4 audio CDs with lots of exercises.
Other Self Help Books (2006-2009)
Other Self Help Books (2006-2009)OTHER SELF HELP BOOKS
- Kashdan, T. (2009). Curious? Discover the missing ingredient to a fulfilling life. New York, NY: Harper Collins.
- Flowers, S. H. (2009). The Mindful Path Through Shyness: How Mindfulness and Compassion Can Free You From Social Anxiety, Fear, and Avoidance. Oakland, CA: New Harbinger Publications.
- Vieten, C. (2009). Mindful Motherhood: Practical Tools for Staying Sane During Pregnancy and Your Child’s First Year. Oakland, CA: New Harbinger Publications.
- McKay, M., & Sutker, C. (2007). Leave Your Mind Behind. Oakland, CA: New Harbinger.
- McCurry, S. M. (2006). When a family member has dementia: Steps to becoming a resilient caregiver. Westport, CT: Praeger Publishers. - Although not directly on ACT or mindfulness, this book for caregivers does include a significant emphasis on acceptance (the author is one of the early ACT therapists from the University of Nevada, Reno and studied with Steve Hayes).
ACT /RFT Reader's Update 2008 - 2011 (Archives)
ACT /RFT Reader's Update 2008 - 2011 (Archives)The ACT/RFT Reader's Update was published from 2008 - 2011. For up-to-date lists of ACT/RFT publications, go to the ACT Randomized Controlled Trials page, the State of the ACT Evidence page, the list of ACT Books, and the Publications section.
The ACT /RFT Reader's Update is an electronic newsletter provided for your information and perusal. This online newsletter provides summaries of recent, ACT and RFT articles (or related articles) published in peer-reviewed journals. In addition, citations for the latest books, book chapters, and unpublished dissertations will be listed.
Our main aim with this update is to keep the ACT/RFT community informed. We hope to include information that is relevant, scientifically sound, and of interest in the ACT/RFT community. Our purpose is not to recreate the abstract of these articles, but to provide a broader summary of the article. However, are goal is to keep the "busy" reader in mind, and therefore, we will work to keep the summaries brief.
Reviewers include:
Robyn Walser, PhD
Christi Ulmer, PhD
Maggie Chartier, MPH, MS
Ian Stewart, PhD
Miguel Rodríguez Valverde, PhD
ACT/RFT Readers Update 2011
ACT/RFT Readers Update 2011Dear Contextual Science Community,
We are happy to be putting out our full 2011 ACT/RFT Reader’s Update. In this Update we review assessment, chronic pain, experiential avoidance, pilot studies, RCT’s, relational frame theory and several research reviews. We hope you find the information helpful. Please take a look at the attached and find what interests you.
It has been interesting times at the Update, with change in editorial/writer staff (a big welcome to Katherine Young, Jeannette Tappe, Tam Nguyen and Aimee Zhang) and other unanticipated delays with this issue, we have been pressed to finish up and post.
We are also looking forward to including and perhaps featuring articles found in the Journal of Contextual Behavioral Science. We hope everyone is enjoying the journal and finding it useful. What a great contribution to ACBS! http://contextualscience.org/JCBS
Lastly and importantly, we are looking forward to ACBS World Conference in Sydney, Australia, July 8-12. The World Conference is always exciting, engaging and fun! Many great ideas for projects, studies and papers are generated at the conference and it will be sure to provide ACT/RFT Reader’s Update staff with plenty more to review! http://contextualscience.org/wc11
Warm Regards,
Maggie Chartier, Psy.D., MPH
Barbara Mazina, B.A.
Tam Nguyen, Ph.D.
Katie Sears, Ph.D.
Ian Stewart, Ph.D.
Jeannette Tappe, M.A.
Thuy Tran, B.A.
Robyn Walser, Ph.D.
Katherine Young, M.S.
Aimee Zhang, B.S.
ACT/RFT Reader's Update 2010
ACT/RFT Reader's Update 2010Dear ACT Community,
We are excited….and relieved to put out two Reader’s Updates this round. Please log in to download the attachments from this webpage.
It is really great to see all of the work and writing that is being done in the areas of ACT, RFT and mindfulness. It is keeping us busy and energized as reviewers. Find in the Update, summaries designed to provide you with a quick overview of topics and issues, with links in the document to more detailed information.
In Update “10finalb” you will find summaries, references and abstracts on acceptance, addiction, assessment, case studies, children/adolescents, chronic pain, experiential avoidance and RFT.
In Update “10finalcd,” in addition to some of the same topics above, you will find summaries, references and abstracts on anxiety and depression, RCT’s and research reviews. In this issue we also wanted to feature RFT. It is the first summary presented in the Update. Ian Stewart has done an excellent job. He has thoughtfully put together information in a effort to keep us abreast of research this area. A big thanks to Ian!
We are diligently working on the next issue: Coming soon to a list-serve near you!
Finally, if you know of any articles, studies or other information that we should include in our next issue and may not be easily findable by regular search engines, please let us know. Also, be sure to let us know if we missed something.
Enjoy!
Reviewers and Editors
Maggie Chartier
Barbara Mazina
Katie Sears
Ian Stewart
Thuy Tran
Robyn Walser
ACT/RFT Reader's Update: Articles from early 2010 (November, 2011)
ACT/RFT Reader's Update: Articles from early 2010 (November, 2011)Dear Colleagues,
Welcome to this edition of the ACT/RFT Reader’s Update.
In this issue, as in all issues, we provide a summary of the literature published related to acceptance and commitment therapy, mindfulness and relational frame theory. We link summaries to particular topics and provide a review of the articles. Feel free to read the summaries and find the links to the references and abstracts related to the summaries right in the document. For a taste of what is in the Update, we summarize 3 articles on acceptance approaches to treatment, 3 on addiction that compare CBT to ACT, 1 on assessment by Wilson – the VLQ is alive and well -, 2 case study designs looking at the treatment of GAD and cancer, 3 articles on mindfulness based approaches with children and parents, 4 articles on experiential avoidance, 5 on mindfulness including how mindfulness works with managing emotions, intrusive thoughts, stress reduction and substance use. Finally, we have 3 on RFT reviewed by Ian – Thanks Ian!
We have sorted and distributed articles to our reviewers for the first half of 2011. We are looking forward to the next round.
Please let us know if we missed anything that we should include or inform us of dissertations, etc.
Thanks and Enjoy!
Kind Regards,
Robyn D. Walser, Ph.D.
ACT/RFT Reader's Update: Final 2009 Review (July, 2010)
ACT/RFT Reader's Update: Final 2009 Review (July, 2010)Science and Practice: ACT /RFT Reader’s Update: Final 2009 Review
Welcome to the ACT/RFT Reader’s update. This is the last issue reviewing the literature on ACT and RFT from 2009. We will be publishing updates for 2010 in late summer, fall and winter.
To kick off the issue, we want to extend a thank you to Dr. Chad Drake who has been with the Update since its inception. We thank Chad as he closes the “Update chapter of his life” and wish him much success in his new and fun endeavors. Thanks Chad!
In this issue, we summarize articles on assessment, ACT and diagnostic populations, experiential avoidance, behavioral health, RFT, mindfulness and “The Great Debate”.
The attached PDF includes a Table of Contents that allows you to “click” directly to the summary of multiple articles covering a topic and/or references and abstracts that you may be interested in. In addition, citations for the latest books, book chapters, editorials, and unpublished dissertations are listed.
Our aim with this update is to provide information that is clinically relevant, scientifically sound, and of interest in the ACT/RFT community. We have worked to keep the “busy” reader in mind and hope that you find the Update useful.
** If you are a graduate student working on an ACT/RFT study and would like to have us include your dissertation or thesis citation in this update,please send us an email backchannel.
**If you have published an editorial you would like us to include that citation, please send us an email back channel.
We hope you will find our e-mail updates of interest and value.
Our editors and reviewers include:
Robyn Walser, PhD
Maggie Chartier, PhD, MPH
Katie Sears, PhD
Thuy Tran, BS
Chad Drake, PhD
Elizabeth Gifford, PhD
Ian Stewart, PhD
Christi Ulmer, PhD
Miguel Rodríguez Valverde, PhD
Darrah Westrup, PhD
ACT/RFT Reader's Update (December, 2009)
ACT/RFT Reader's Update (December, 2009)| Science and Practice: ACT/RFT Reader’s Update December, 2009 |
___________________
Acceptance and Values-Based Action in Chronic Pain: A Study of Treatment Effectiveness and Process Cognitive-behavioral approaches to pain management have an established record of empirical support. However, as true with other behavioral problems, the mechanism by which improvement occurred is inconsistent with the theoretical underpinnings of CBT. In a recent paper, Vowles and McCracken add to their ongoing line of research in acceptance-based approaches to the treatment of chronic pain. In their paper, they present their findings of an inter-disciplinary treatment program based in Acceptance and Commitment Therapy, with a focus on acceptance and values-based action. One-hundred seventy-one participants completed the program which consisted of 3 to 4 weeks of inpatient treatment for about 30 hours per week. Participants improved across almost all domains, including pain, depression, pain-related anxiety, disability, medical visits, work status, and physical performance, and effect sizes for these improvements were medium to large. Analysis of reliable change revealed that 75.4% of participants improved in at least one key domain assessed. In contrast with CBT-based approaches to pain management, improvements across these domains were associated with ACT's proposed mechanisms of action, namely, acceptance of pain and values-based action. The authors conclude that these findings provide support for the ACT model of treatment for chronic pain, and the processes associated with improvement – acceptance and values-based action.
Vowles, K., & McCracken, L. (2008). Acceptance and values-based action in chronic pain: a study of treatment effectiveness and process. Journal of consulting and clinical psychology, 76(3), 397-407.
___________________
Rule-Governed Behavior and Psychological Problems Humans, uniquely among animals, can come to understand and respond to linguistic rules, both effective ones and not so effective ones. The effective ones help us to learn and adapt to our environment. The ineffective ones can cause maladaptive behavior and diminish our lives considerably. This paper presents a functional analysis of patterns of rule-governed behavior (RGB) and shows how rules can contribute to psychopathology. Rules have been described as antecedent stimuli that alter the functions of stimuli in our environment. They allow us to respond to that environment in complex and efficacious ways. But what are rules? Relational Frame theory suggests that we humans learn to respond in accordance with abstract relational patterns based on cues (e.g., SAME). Rules are essentially combinations of cues that specify particular relations between environmental stimuli and between environment and behavior and thus allow us to respond in new ways (‘transformation of function’). The paper describes three functional patterns of RGB. These are pliance, tracking and augmental rule following. Pliance is RGB under the control of a history of socially mediated reinforcement for coordination between behavior and antecedent verbal stimuli (rules). A typical example might be a child obeying the rule ‘Don’t touch my laptop’ because their parent has given them this rule and because their parent has previously provided consequences for following or not following rules. Tracking is RGB under the control of a history of coordination between the rule and the way the environment is arranged independently of the rule. An example might be a child obeying the parental rule ‘Eat your breakfast because it will give you more energy’ because in the past the child has experienced the effect of other rules that have been accurate in their description of the environment. If this rule also shows coordination (i.e., the child finds an increase in energy when they eat breakfast), then this will further strengthen tracking behavior. Augmenting is RGB due to relational networks that alter the degree to which events function as consequences. The example given is ‘Eat your vegetables to be a big strong boy’. If this rule makes vegetable eating more reinforcing then it might be described as augmenting. Each of these patterns has its advantages and its disadvantages, including maladaptive behavior. It’s useful for children to learn pliance since this allows them to acquire useful adaptive habits, but doing things just because one is told to can make one insensitive to one’s environment. Tracking allows independence from social whim, but tracking can also lead to ineffective behavior; for example, tracking short term reinforcement can mean one misses longer term reinforcement. Augmenting is the most advanced form of rule governed behavior and as such it can interact with and reinforce either of the other two functional patterns resulting in strongly adaptive or maladaptive patterns. Experiential avoidance can be a product of the latter while valuing, an important part of the antidote to EA, is an example of the former. Törneke, Luciano and Valdivia (2008) have provided an excellent description of RGB and its relationship to psychopathology.
Törneke, N. Luciano, C. & Valdivia Salas, S. (2008). Rule-Governed Behavior and Psychological Problems. International Journal of Psychology and Psychological Therapy, 8 (2), 141-156.
___________________
Brief Review: A Parametric Study of Cognitive Defusion and Believability The effects of the “Milk, milk, milk” exercise are dependent upon the length of the intervention: Reducing distress in respect to private events has been a major emphasis of traditional behavioral and cognitive behavioral therapies. The inclusion of mindfulness interventions in some contemporary therapies like ACT has shifted this focus from distress reduction to changing the behavior regulatory functions of distressing private events. One means of examining this change is by asking clients about the believability of their thoughts. Defusion interventions represent efforts to disrupt this behavior regulation, and the “milk, milk, milk” exercise is the intervention examined in this article. Two studies examined the effect of this exercise on the emotional discomfort and believability of a negative, self-relevant word identified by the participant as sufficiently problematic. Each study varied the amount of time spent repeating the word – 0, 3, or 20 seconds in study 1 and 1, 10, or 30 seconds in study 2. A rationale for the procedure and training with the word “milk” was provided before each intervention. Results showed that emotional distress reduced significantly within 3-10 seconds, while believability reduced significantly only after 20-30 seconds. The difference in timing for these reductions suggests that discomfort and believability are functionally distinct behaviors. The authors suggest extending defusion exercises until the believability of thoughts, rather than just emotional distress, diminishes.
Masuda, A., Hayes, S. C., Twohig, M. P., Drossel, C., Lillis, J., & Washio, Y. (2009). A parametric study of cognitive defusion and the believability and discomfort of negative self-relevant thoughts. Behavior Modification, 33, 250-262.
___________________
Brief Review: Relational Frame Theory and Social Categorization The Matching-to-Sample procedure can transform the functions of arbitrary stimuli in the Implicit Associations Test: This study examined the acquisition of obesity stigma to arbitrary stimuli. More specifically, the matching-to-sample (MTS) procedure was used to provide relational conditioning sufficient to generate a transformation of stimulus functions for stigma to images of either horizontal or vertical lines. The Implicit Associations Test (IAT) was used to detect this transformation of functions. Fifty undergraduate psychology students engaged in a series of five computerized tasks: (1) an IAT containing evaluative words and images of horizontal and vertical lines, to confirm a lack of pre-existing bias, (2) an established IAT for detecting implicit evaluative bias toward obesity, to confirm the presence of pre-existing bias, (3) two MTS tasks providing relational conditioning sufficient to generate the transfer of positive and negative evaluative functions to images of horizontal and vertical lines, (4) the same IAT used in step 1, to assess for the acquisition of bias, and (5) the same IAT used in step 2. Results confirmed no pre-existing bias at time 1, a large and significant predicted bias at time 2, and a small and significant predicted bias at time 4. The results of this study are discussed in respect to an RFT account of the development of stigma and social categorization and contrasted with a more mainstream, cognitive account known as the Social Knowledge Structure.
Weinstein, J. H., Wilson, K. G., Drake, C. E., & Kellum, K. K. (2008). A relational frame theory contribution to social categorization. Behavior and Social Issues, 17, 39-64.
| Revised/Reviewed by: Walser, R., Chartier, M., Sears, K., Drake, C., Valverde, M., Stewart, I., Ulmer, C., & Westrup, D. Read the ACT RFT Reader's Update: References & Abstracts, 2008 in an interactive PDF, attached below. |
ACT/RFT Reader's Update (Fall, 2008)
ACT/RFT Reader's Update (Fall, 2008)Science and Practice: ACT /RFT Reader's Update Fall, 2008
Welcome to ACT/RFT Reader's Update:
In our second issue we summarize 5 articles recently published in peer-reviewed journals. The references to full citations and whether they are available for download on the ACBS website is also included. Citations for the latest books, book chapters, and unpublished dissertations are listed at the end of the update. If you don't see your recently published article….hang on, we continue to work on future issues and have a fair number of articles that are being reviewed and summarized for our coming issues. However, if you are publishing or have recently published please make us aware by either sending us the reference or pdf. Thanks.
We hope you will find our e-mail updates of interest and value.
Enjoy your read!
Our editors and reviewers/writers:
Editors:
Robyn D. Walser, Ph.D.
Maggie Chartier, MPH, MS
Reviewers/Writers:
Chad Drake, MA
Miguel Rodríguez Valverde, PhD
Ian Stewart, PhD
Christi Ulmer, PhD
This issue of Science and Practice: ACT/RFT Readers Update contains 5 summaries:
ACT ARTICLES AND RELATED TOPICS
Acceptance and commitment training reduces prejudice and promotes diversity-oriented behaviors in college students
Despite increased efforts at promoting diversity in recent years, prejudice continues to result in diminished quality of life for ethnic, racial and religious minorities across numerous life domains. Interventions designed to reduce prejudice have been moderately successful with short-term improvements, but do not seem to promote sustained equitable attitudes and behavior. In fact, in some instances, the interventions actually result in an increased bias. ACT may be particularly applicable to prejudice due to its focus on intransigent and difficult cognitions. Luoma and Hayes compared a brief ACT Training protocol to an education-based prejudice awareness training intervention for reducing racial and ethnic prejudice in college students. Material was presented to students using a counterbalanced within-group design such that the impact of each approach could be evaluated independently. The outcome measure, developed for this study, consisted of items assessing the following: awareness of bias; acceptance and flexibility; thought control and defusion; and positive actions. Student responses suggest that the ACT training produced greater reductions in prejudice across most dimensions, and that only ACT training promoted greater intention to engage in diversity-oriented behaviors. Changes in these positive intentions were partially mediated by acceptance and flexibility, and defusion processes explained more variance in positive intention outcomes than acknowledgement of bias. The authors suggest that the combined findings of this study and a previous ACT-based study on prejudice lend preliminary support to an ACT-RFT based model of understanding and reducing prejudice. The findings are also consistent with the theory underlying acceptance-based approaches stating that it is the relationship with thought rather than the content of thought that matters. Limitations of the study include the use of an unvalidated outcome measure, the potential self-selection bias of students who choose to enroll in a class on the psychology of racial differences, the potential for bias of the interventionist in favor of ACT, and a short follow-up interval. Future studies are proposed using a more intensive intervention and assessing longer-term outcomes. Given the need for empirically supported approaches to address prejudice, the findings of the current study are promising. In terms of clinical application, the authors propose that similar processes are likely in play with regard to mental health stigma, and that cognitive processes that promote prejudice are themselves psychologically damaging.
Read the Article:
Lillis, J., & Hayes, S. C. (2007). Applying acceptance, mindfulness, and values to the reduction of prejudice: A pilot study. Behavior Modification, 31(4), 389-411.
________________
ACT and CT for anxiety and depression, a randomized controlled effectiveness trial
For some period of time there has been discussion and even argumentation between those who hold true to cognitive models of intervention (e.g. Beckian) and acceptance models of intervention (e.g. Hayesian). Forman and colleagues take a closer look. They explain that Cognitive Therapy (CT) has a mixed record of success in producing theoretically-consistent mediation of treatment outcomes while Acceptance and Commitment Therapy (ACT) has a relatively impressive, though preliminary record, of the same. Given that only a handful of studies have directly compared these treatments and that all contained methodological shortcomings the authors undertook that task of comparing each therapy's ability to produce mediation and positive outcomes among an outpatient sample of college students in a well-controlled trial. Services were provided by clinical psychology doctoral candidates working at a student counseling center. Outcome measures included self-reports of symptoms (BDI-II, BAI, OQ-45) and self-reports of quality of life (QOLI, SLS). Two mediational measures were administered (KIMS, AAQ). The study also included measures of treatment fidelity, therapist allegiance, and participant expectancies of treatment. Results showed that all measures were comparable between treatments, and that each treatment generated large effect sizes. Mediational analyses showed that the observing subscale of the KIMS more strongly (though nonsignificantly) predicted outcomes for CT, while the AAQ and the acting with awareness and acceptance subscales of the KIMS more strongly (and significantly) predicted outcomes for ACT. The authors reported that "changes in "observing" and "describing" one's experiences were more strongly associated with outcomes for those in the CT group relative to those in the ACT group, whereas experiential avoidance, acting with awareness, and acceptance were more strongly associated with outcomes for those in the ACT group" (p. 792). Although, the authors concluded that "these findings support the notion that CT and ACT are functionally distinct from one another" (p. 792), it was never explained why the capacity to observe and describe one's private experiences is a fundamental component of CT but not ACT.
Read the Article:
Forman, E. M., Herbert, J. D., Moitra, E., Yeomans, P. D., & Geller, P. A. (2007). A randomized controlled effectiveness trial of Acceptance and Commitment Therapy and Cognitive Therapy for anxiety and depression. Behavior Modification, 31, 772-799.
RFT ARTICLES
How does multiple-exemplar training and naming establish derived equivalence in an infant?
Stimulus equivalence at its simplest can be described as follows. Imagine I train someone in the following two relations between physically different arbitrary stimuli: Pick stimulus B when you see stimulus A, and pick stimulus C when you see stimulus B. If given the opportunity, a verbally able human might subsequently go on to demonstrate further relations, without being trained to do so, including picking A when he sees B, and picking B when he sees C (i.e., reversing the trained relations, referred to as symmetry), picking C when he sees A (i.e., combining the trained relations, referred to as transitivity) and picking A when he sees C (a combination of symmetry and transitivity). This pattern of derived responses has been called stimulus equivalence, because it appears that, suddenly and unexpectedly and without being trained to do so, the person is treating a number of physically different stimuli as mutually substitutable for or equivalent to each other. There is growing interest in stimulus equivalence research as only verbally able subjects seem to be able to show this pattern readily, suggesting a link between equivalence and language. But what is the nature of this link? How are the two connected? The present paper discusses two theoretical approaches that claim to account for this link - Relational Frame Theory (e.g., Hayes et al., 2001) and Naming Theory (Horne & Lowe, 1996). More importantly, however, the paper reports a series of experiments involving training an infant in relational responding that provide important additional evidence pertaining to the debate between these approaches. More specifically, the results add to evidence in favour of the RFT account, while demonstrating a phenomenon that directly contradicts Naming Theory. This study is a significant empirical contribution for a number of reasons (i) It demonstrates the use of multiple exemplar training to establish generalized contextually controlled receptive mutual entailed relational responding; (ii) it provides the youngest empirical example of coordinate (sameness) combinatorial entailed relational responding (equivalence) ever recorded; and (iii) it provides extremely important evidence vis-a-vis the Naming Theory / RFT debate by providing empirical evidence that directly contradicts a core tenet of Naming Theory while being consistent with RFT.
Read the Article:
Luciano, C., Becerra, I. G., & Valverde, M. R. (2007). The role of multiple-exemplar training and naming in establishing derived equivalence in an infant. Journal of the Experimental Analysis of Behavior, 87(3), 349-365.
________________
Can the Implicit Relational Assessment Procedure be faked? First evidence says no.
The Implicit Relational Assessment Procedure (IRAP) is a computer-based task for the assessment of implicit cognitions recently devised within the theoretical framework of RFT. It is a latency-based response measure that intends to assess the participants' existing verbal-relational networks (i.e. beliefs). It works by requiring participants to respond as quickly and accurately as possible across trials when presented with particular relations (among sample and target stimuli) that may be consistent or inconsistent with their beliefs (i.e. relational networks). The idea is that participants will be faster when required to respond to stimulus relations that are consistent (e.g. categorizing words like love or peace as pleasant, and words like vomit or death as unpleasant) than to stimulus relations that are inconsistent with their verbal histories (e.g. categorizing vomit or death as pleasant, and love or peace as unpleasant). This idea is supported by empirical evidence from several recent studies. As with other implicit measures, like the Implicit Association Test (IAT), one of the strengths of the IRAP is that it may be less sensitive than questionnaires and other explicit measures to assess deliberate attempts to conceal information about one's own socially sensitive attitudes. This study attempted to see to which extent this is the case (i.e. whether the IRAP can be faked). Three groups of participants underwent two consecutive exposures of the IRAP task with the same stimuli (the words pleasant and unpleasant as samples, the words similar and opposite as response options, one set of six pleasant target words, and one set of six unpleasant target words). Between both exposures, one group was informed about how the IRAP works. Another group received the same information and was told to fake the IRAP, without a specific strategy to do so. The third group received the same information and were also provided with a strategy, namely slowing down on consistent trials and going fast on inconsistent trials. Results showed no evidence of faking in any condition. All groups showed an IRAP effect in the second exposure regardless of the instructions or strategies received. According to a post-task questionnaire, only two participants in the third group reported using the specific strategy they had received. All in all, participants found it difficult to fake the IRAP, even if provided with specific strategies. This contrasts with previous findings with the IAT, which can be successfully faked when explicitly told how to do so. This observed resistance to deliberate attempts to fake performance renders the IRAP a solid procedure for the assessment of implicit cognitions.
Read the Article:
McKenna, I., Barnes-Holmes, D., Barnes-Holmes, Y., & Stewart, I. (2007). Testing the Fake-ability of the Implicit Relational Assessment Procedure (IRAP): The First Study. International Journal of Psychology and Psychological Therapy, 7, 253-268. (in English)
______________________
What can RFT add to the study of pain?
The current study focuses on an RFT interpretation of the way that pain takes part in complex behavioural episodes for humans. It is a theoretical/conceptual study that reviews functional-contextual approaches to the study of private events specifically related to pain and with a special emphasis in recent research in verbal behaviour, behaviour-behaviour relations, and transformation of psychological functions. The review is divided into four parts. The first summarizes the philosophical assumptions of functional-contextualism and its implications for the study of pain (e.g. the extent to which explanations of pain allow for effective action as the criterion against which these explanations should be tested). The second focuses on the classical behaviour-analytic point of view, where pain experiences have been conceptualized as private events that exert discriminative control over subsequent behaviours (e.g. abuse of pain-killers, inactivity, social isolation, etc.). This discriminative function (behaviour-behaviour relation) is the product of specific histories of reinforcement along the individual's development, in direct-contingency terms. This view is illustrated with the presentation of the contributions of Schoenfeld and, more specifically, of Fordyce. RFT is proposed as a more comprehensive framework for the behaviour ral study of pain, a framework where verbal (derived) histories can be included as part of the explanation. In line with this, pain-related clinical problems are conceptualized as a form of experiential avoidance disorder, where it is the verbal functions of pain, rather than pain itself, that limit the individual's life (i.e. the consideration of pain as a literal barrier for engaging in valued actions). This is described in the third part of the article. Finally, the last part of the article presents a general overview of ACT and describes its implications for the treatment of pain-related problems.
For more information, read the original article in Spanish:
Gutiérrez Martínez, O., & Luciano Soriano, C. (2006). Un studio del dolor en el marco de la conducta verbal. International Journal of Clinical and Health Psychology, 6, 169-188. [A study of pain in the framework of verbal behavior: from the contributions of W. E. Fordyce to Relational Frame Theory (RFT)]
(for correspondence and reprints): [email protected]
BOOKS
Ciarrochi, J. V., & Bailey, A. (2008). A CBT practitioner's guide to ACT. Oakland, CA: New Harbinger.
BOOK CHAPTERS
DISSERTATIONS
Barthold, C., & Hoffner, C. (2007). Factors affecting the generalization of 'wh-' question answering by children with autism. Dissertation Abstracts International Section A: Humanities and Social Sciences, Vol 68(4-A): 1403.
EDITORIALS AND COMMENTARIES
Hayes, S. (2007). Hello Darkness. Psychotherapy Networker, Sept/Oct. 46-52.
Hummelen, J. W., & Rokx, T. A. J. J. (2007). Individual-context interaction as a guide in the treatment of personality disorders. Bulletin of the Menninger Clinic, 71(1): 42-55.
Muran, J. C. (2007) Commentary: Language, Self, and Diversity. In S. C. Hayes (Ed.), Dialogues on difference: Studies of diversity in the therapeutic relationship ) pp. 275-279. Washington, DC, US: American Psychological Association.